
Abstract
Purpose:
This study aims to report the epidemiology of patellar sleeve injuries, describe diagnostic findings and treatment, and assess functional outcomes following different treatments.
Methods:
A medical database was queried from 1990 to 2016 to identify patients ≤18 years presenting to a single pediatric institution with a patellar sleeve injury. Patients with significant comorbidities or previously operatively treated for ipsilateral knee injuries were excluded. Standard demographic data, mechanism of injury, skeletal maturity, injury-related radiographic parameters, along with treatment paradigms, post-treatment clinical and radiographic findings, and patient-reported outcomes were collected.
Results:
A total of 90 patients, mean age of 10.7 years (range: 7–17) was included, of which 69 (77%) were male. Seventy-three percent of all injuries occurred while playing sports (particularly football/basketball/soccer), with “direct blow” or “landing” being the most prevalent mechanisms of injury. Twenty-six (29%) underwent operative treatment, with transosseous suture fixation being the most popular surgical technique (73%). Of the 64 (71%) non-operatively treated patients, 18 (39%) were placed in a hinged knee brace locked in extension with the remainder split between casting and standard knee immobilizer. Compared to the non-operative cohort, a higher percentage of the operative group had a pre-treatment extensor lag (p < 0.001) and greater fragment displacement (p < 0.001) with patella alta (p < 0.001) on imaging. There was no difference in outcome scores (Pedi-IKDC/Lysholm) or patella alta on radiographs between groups. Post-treatment surveys indicated no difference in residual pain or ability to return to sport.
Conclusion:
This large case series provides valuable epidemiologic, clinical, and radiographic data describing patellar sleeve fractures, along with outcomes following non-operative and operative treatments.
Level of evidence:
IV.
Introduction
Patellar sleeve injuries, though rare, account for the most common patella fractures in children and adolescents. 1 Developmentally, the patella begins to ossify at age 3, with multiple ossification centers localized to the center of the patella, progressing peripherally as the child grows and matures.1,2
During this period, a powerful contraction of the quadriceps against resistance, such as jumping or landing, provides a sudden force which is more likely to avulse cartilage and newly formed patellar bone than tear the patellar tendon collagen fibers. This primarily occurs at the distal pole of the patella, although it may affect the superior pole.3,4 When the injury occurs, a complete sleeve or cuff of tissue, which can involve a small amount of bone with a large amount of articular cartilage, is pulled away from the circumference of the patella resulting in elongation or complete disruption of the extensor mechanism. 2 Adolescents are the most susceptible, likely due to the combination of intensity of sporting activity, rapid growth, and osteochondral transformation at the periphery of the patella. While the peak incidence occurs at 12.7 years, the average age range is 8–16 years. 5
Patellar sleeve avulsion injuries can be difficult to detect since cartilage, rather than calcified bone, may be all that has avulsed. Since this is not readily visible on plain radiograph, clinical findings including a palpable defect at the distal pole of the patella, knee effusion and/or edema, extensor lag or inability to straight leg raise, and patella alta on radiograph may be the only evidence of this injury. 6 Other diagnostic imaging such as ultrasound and magnetic resonance imaging (MRI) may be useful in making the diagnosis.
Due to the difficulty with which this diagnosis is made, patellar sleeve injuries may be misdiagnosed, leading to delay in treatment. This can carry serious consequences including knee instability, chronic extensor lag, quadriceps weakness and wasting, chronic anterior knee pain, patella magna, or duplication of the patella.7,8 Once a diagnosis is made, treatment may be operative or non-operative. Historically, with minimally displaced injuries, closed treatment in a cast in full extension was considered acceptable. 9 However, there are reports that non-operative management, even in minimally displaced cases, may lead to chronic patella alta, ossification of the patellar tendon, or need for future surgery in cases of delayed presentation.6,10 Operative management typically consists of transosseous suture repair, tension banding, or intraosseous anchor repair. 11 The outcomes of each treatment have yet to be compared.
Due to the rarity of this serious injury, most of the literature to date is based on case reports and small series.3 –6,8,10,12,13 This large retrospective case series aims to better understand and report on the epidemiology of patellar sleeve injuries, describe common diagnostic findings and treatment types, and assess functional outcomes following different treatment paradigms.
Materials and methods
Study design
This is a single-center, retrospective case series. Approval was obtained by the Institutional Review Board prior to data collection.
Eligibility criteria
A medical record database was queried from 1990 to 2016 to identify patients 18 years or younger presenting to a single pediatric institution with a patellar sleeve injury diagnosis treated either operatively or non-operatively. Patients were identified using the institution’s search engine to search for the following key words within operative reports and clinic notes: “patella/r sleeve fracture,” “patella/r avulsion,” “patella/r sleeve injury,” and/or “patella/r sleeve-type fracture.” Patients with significant comorbidities including syndromic and neuromuscular conditions were excluded from the study. Patients previously treated operatively at an outside hospital for patella sleeve injury, other ipsilateral knee injury, and previous diagnosis of osteochondrosis affecting the patella pole were also excluded.
Data collection through chart review
The primary outcomes included descriptive reporting of patient, injury, and treatment characteristics, as determined by medical review. Standard demographic data (including patient age, sex, body mass index (BMI)), skeletal maturity, mechanism of injury, and sport(s) played were collected. Clinical and diagnostic findings were also examined including knee effusion, (in)ability to straight leg raise, extensor lag (defined as inability to fully extend the knee during active quadriceps contraction), and any palpable defect adjacent to the patella. These findings were recorded according to the clinical notes documented by the treating orthopedic surgeons. Radiology parameters were also collected including fragment size, displacement, and Caton–Deschamps index (CDI) on radiographs and advanced imaging, when available. Patella alta was defined as a CDI > 1.3. Radiographs, when available, were examined to assess the skeletal maturity based on the distal femoral physis, which was recorded as a binary variable. Specific treatment paradigms for both non-operatively and operatively treated injuries as well as post-treatment complications and return-to-sport were recorded.
Prospective data collection through questionnaire
Functional outcomes were collected as the study’s secondary outcome and measured by a one-time questionnaire administration at least 1 year postoperatively (operative cohort) or 1 year post-injury (non-operative cohort). The questionnaire was distributed in English to all patients who met eligibility criteria in the study through the mail. Those participants who did not respond to the questionnaire within 2 weeks of mailing were sent a second mailing. Those who did not respond to either of the two mailings were contacted via telephone call to discuss participation in the study and determine whether another copy of the questionnaire was required to be mailed. Phone calls were repeated, with 1 week between phone calls if the first attempt to contact the patient was unsuccessful. The components of the questionnaire included several validated patient-reported outcome tools: the Pedi-IKDC Subjective Knee Evaluation Form (a knee-specific measure of symptoms, function, and sports activity), 14 the Lysholm Score (a knee-specific measure of symptoms and function), 15 and the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS), a description of post-treatment activity level. 16
Statistical analysis
Patient demographics were summarized for the cohort by mean and standard deviation (SD) or median and interquartile range (IQR) for continuous characteristics, and by frequency and percentage for categorical characteristics. We used a normative Pedi-IKDC score of 85 with a SD of 15, based on previous data, 17 to conduct a power and sample size analysis using a two-sided, one-sample t test with an alpha set to 0.5%. Our analysis determined that a sample size of 20 would be needed to achieve 80% power to show the minimal clinically important change of a 10-point difference in outcome scores between our cohort and the normative group. Normality of the data was assessed using a Shapiro–Wilk test. Continuous variables were compared using a Mann–Whitney U test or Student’s t test, as appropriate, based on normality. Categorical variables were compared using a chi-square test or Fisher’s exact test as appropriate based on the number of subjects. Pedi-IKDC functional outcome scores were compared to the normative values using the Mann–Whitney U test or Student’s t test, as appropriate, based on normality. An ordinary least squares linear regression was used to look at predictive factors for Pedi-IKDC scores and binomial logistic regression to investigate predictive factors for surgical complications. A p value of <0.05 was considered statistically significant. Statistical analysis was conducted using R version 3.6.1 (R Foundation, Vienna, Austria) and Jamovi version 1.6 (The Jamovi project, 2021).
Results
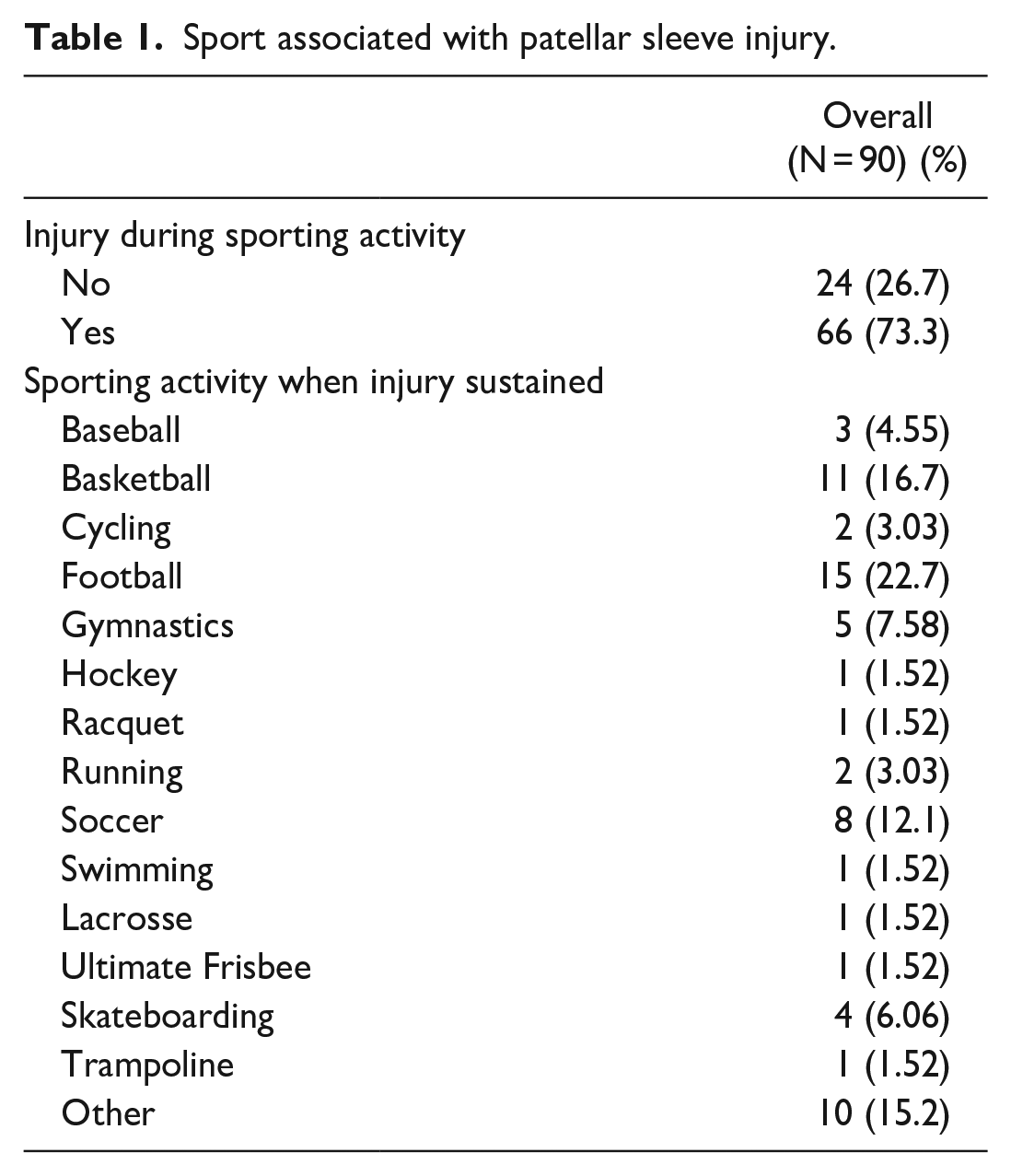
A total of 90 patients were included in the study with a mean age of 10.7 years (range: 7–17), of which 69 (77%) were male and 21 (23%) were female. The patients had a mean BMI of 20.3 ± 4.2 and nearly 80% of the patients self-identified as athletes. The majority (73%) of patellar sleeve injuries occurred while playing sports, with football, basketball, and soccer being the most common, respectively (Table 1), and “direct blow” (34.4%) or “landing” (21.1%) being the most common mechanisms of injury (Figure 1). There was no statistically significant difference between the types of trauma.
Sport associated with patellar sleeve injury.
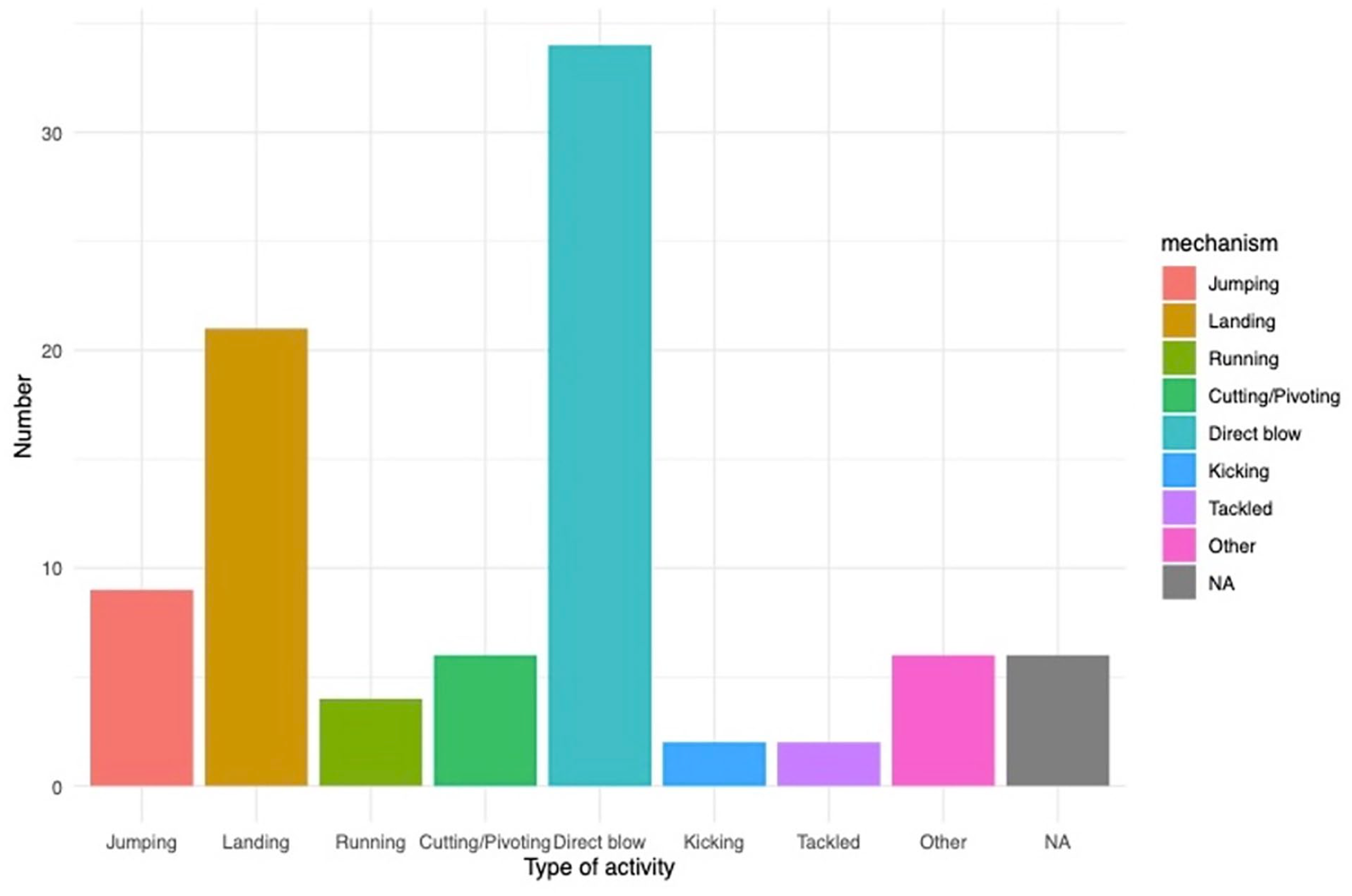
Bar graph depicting most common mechanisms of injury in patients sustaining patellar sleeve injuries in this cohort.
On physical examination, 44% of all patients presenting with a patellar sleeve injury had a knee effusion and 49% had a documented extensor lag (i.e. inability to actively achieve full extension of the knee or active range of knee extension was less than their passive range of extension). In comparing the cohort of patients who ultimately underwent operative compared to non-operative treatment, on initial/preoperative examination, a higher percentage of the operative group had a high-riding patella (p < 0.001) and a palpable defect of the affected patellar pole (p < 0.01). Patients who underwent operative fixation also had a significantly higher rate of extensor lag or inability to fully extend the knee (p < 0.001) (Table 2).
Knee examination comparison between operative and non-operative cohorts.
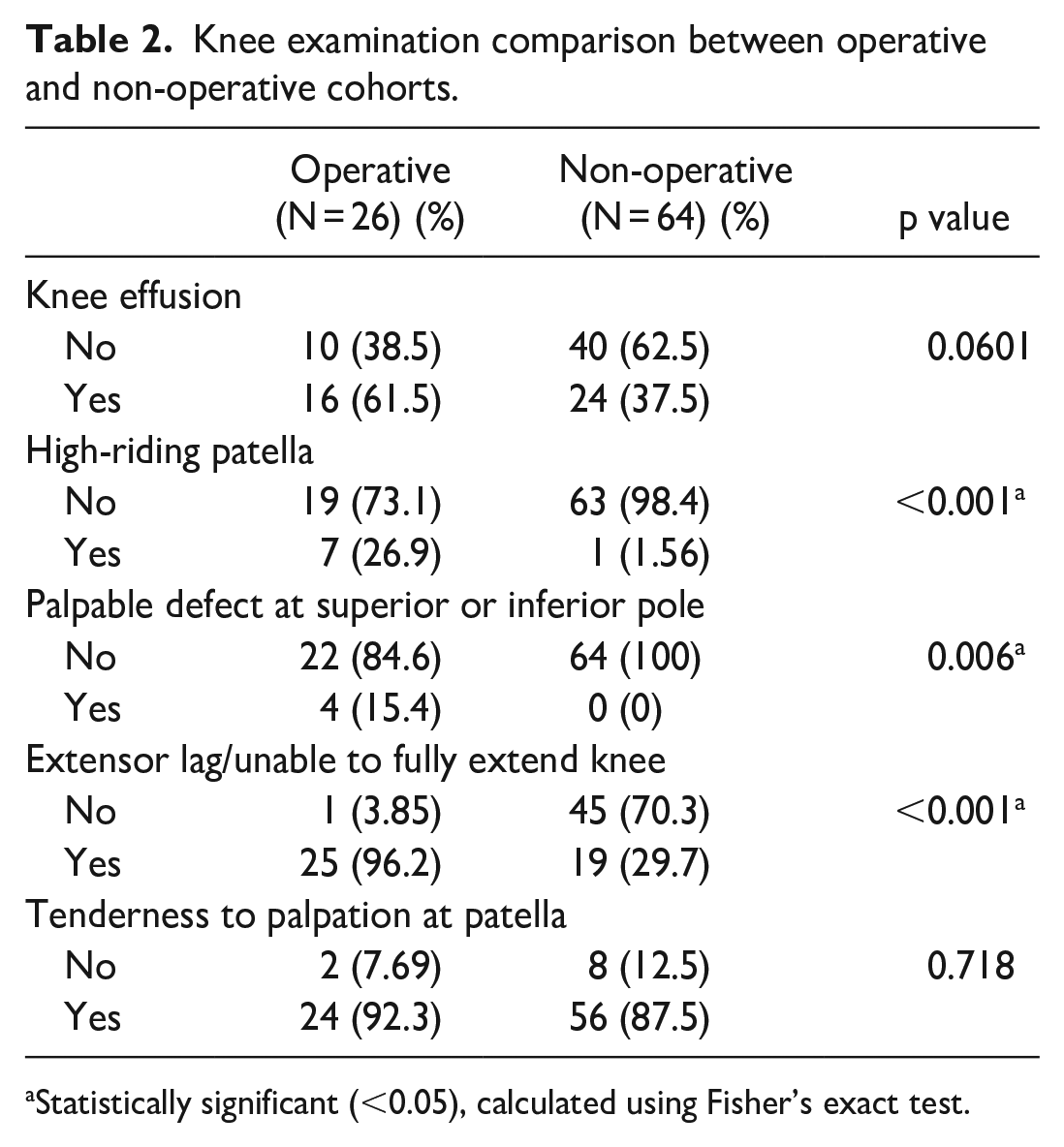
Statistically significant (<0.05), calculated using Fisher’s exact test.
Of the 90 patients included in the study, 79 patients had pre-treatment radiographs (87.8%) and 26 patients had pre-treatment MRI (28.9%) that were able to be viewed and analyzed on the institution’s imaging system. All but one patient was skeletally immature at the time of injury. The patient who was deemed skeletally mature based on the distal femoral physis on plain radiograph was 17 years of age at the time of injury. Looking at the overall cohort of patellar sleeve injuries, 25 (32%) had patella alta on radiograph. Compared to the patients treated non-operatively, patients who underwent surgical intervention had both a higher rate of patella alta (p < 0.001) and a higher mean fragment displacement (p < 0.001) on pre-treatment imaging compared to the non-operative group (Table 3). The most common location of the patellar sleeve injury as identified on the MRI was the inferior pole (Table 3).
Imaging comparison between operative and non-operative cohorts.
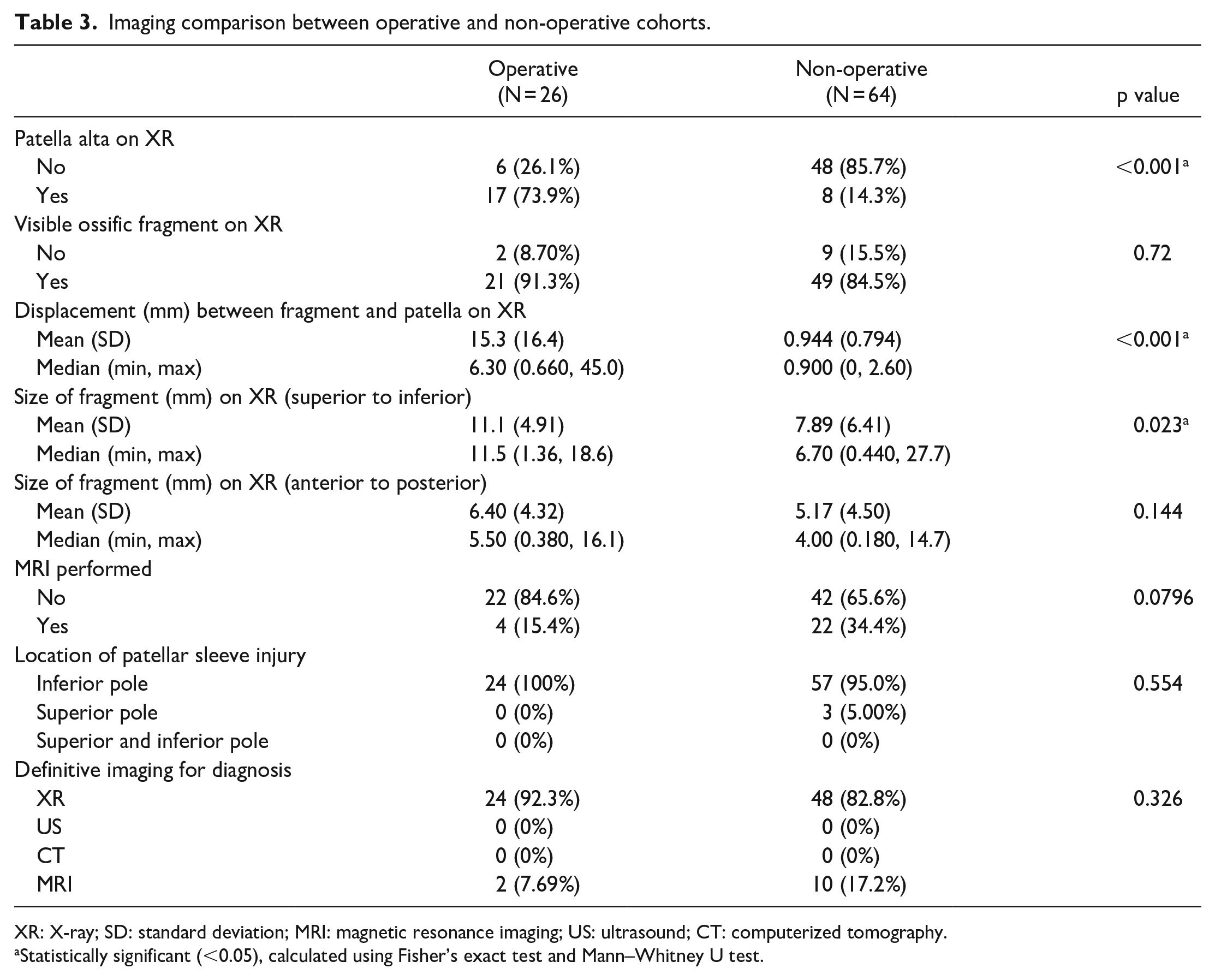
XR: X-ray; SD: standard deviation; MRI: magnetic resonance imaging; US: ultrasound; CT: computerized tomography.
Statistically significant (<0.05), calculated using Fisher’s exact test and Mann–Whitney U test.
Examining the management of patellar sleeve avulsion injuries, 26 patients (29%) underwent operative treatment, whereas 64 patients (71%) were treated non-operatively. No patient initially underwent a trial of non-operative management, followed by operative treatment. Within the operative cohort, open reduction and internal fixation (ORIF) with transosseous suture was the most common surgical technique (73%) followed by transosseous wire fixation then screw fixation. Within the operative cohort, one patient underwent revision of fixation, three reported surgical site infections (superficial or deep), and eight patients (31%) ultimately underwent removal of hardware. Within the non-operative cohort, the utilization of a hinged knee brace locked in extension was the most common initial treatment option (39%) followed by casting in extension (26%) or a standard knee immobilizer (26%). Total time in any form of immobilization was 48 days on average.
Post-treatment analysis revealed no significant difference in patellar tendon ossification on final radiographs. While the operative cohort had a slightly higher CDI postoperatively, there was no statistically significant difference in patella alta between the two groups post-treatment. Of note, three patients in the operative cohort were found to have an extension lag at the final follow-up compared to no patients in the non-operative group (p < 0.05). Based on chart review of all patients, there was no difference in return-to-sport between the two cohorts (Table 4).
Clinical and radiographic outcomes.
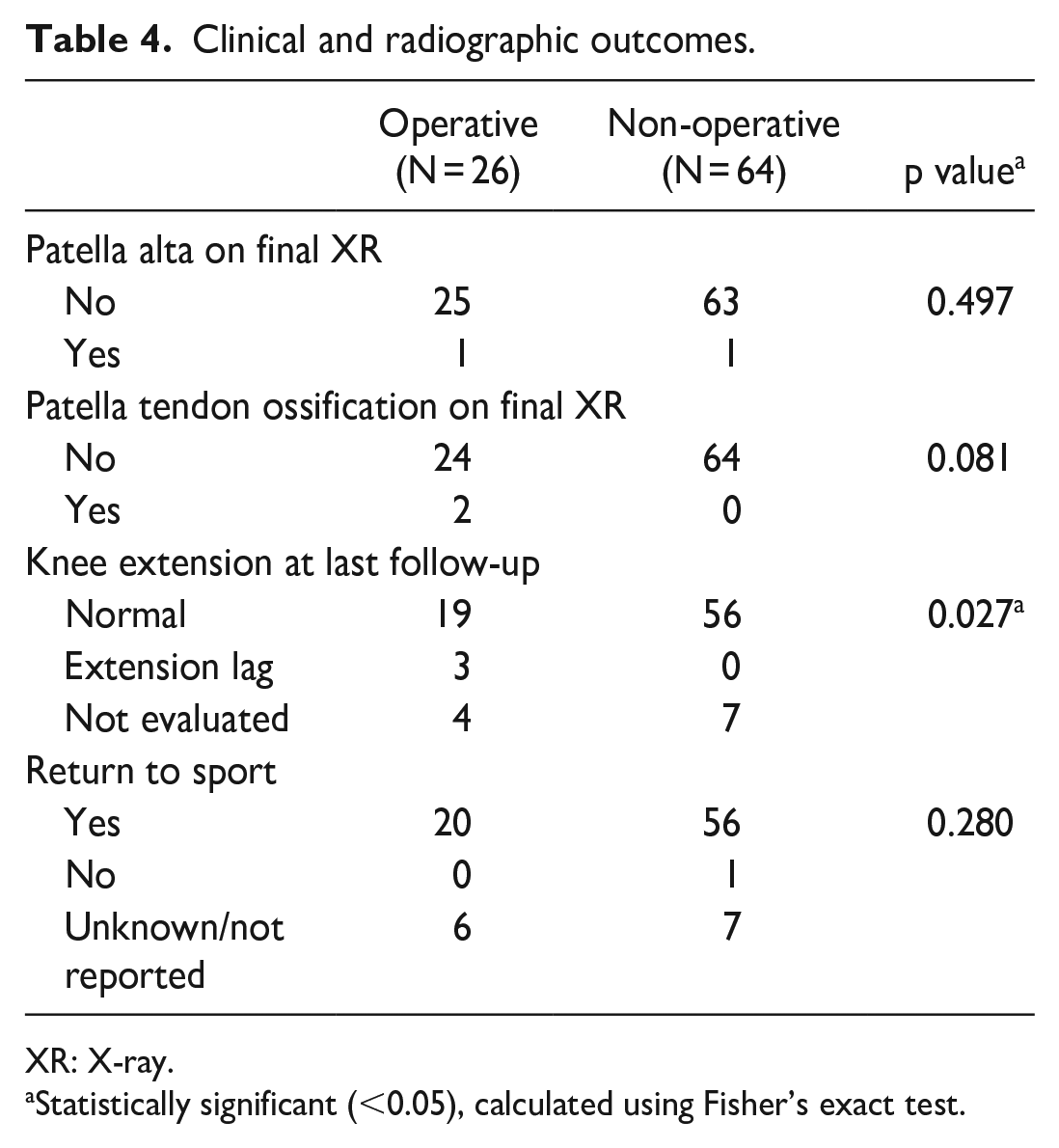
XR: X-ray.
Statistically significant (<0.05), calculated using Fisher’s exact test.
The post-treatment survey was completed by 27 patients (30% of all patients), including 9 who received operative management and 18 who received non-operative management. Comparing operatively and non-operatively treated patients, there was no difference in outcome scores (Pedi-IKDC/Lysholm/Pedi-FABS). Post-treatment survey results also indicated no difference in residual knee pain or ability to return to same level of sport. A linear regression model with age, BMI, initial CDI, operative versus non-operative management, and amount of displacement on pre-treatment radiographs did not significantly predict the final outcome score, nor did they explain a significant amount of variation in the score.
Discussion
This large retrospective case series captures the basic demographic information, mechanism of injury, initial clinical examinations and radiographic features, and treatment paradigm of pediatric and adolescent patients who sustained a patellar sleeve avulsion injury and were evaluated at a single tertiary-care pediatric institution. Operative and non-operative post-treatment outcomes were analyzed and compared in a subgroup analysis to reveal comparable chart-based and prospectively collected patient-reported functional outcomes including return to sport.
Consistent with the known, albeit limited, literature to date,5,13 our series demonstrated patellar sleeve injuries more commonly occur in males with a rate of 3:1. All but one patient with available imaging to review was skeletally immature at the time of injury. Football, basketball, and soccer were the three most common sports being played at the time of injury. It is interesting to note that all three sports involve forceful quadriceps contraction, a known etiology of this injury, 2 and may involve a direct blow to the knee.
In evaluation of patellar sleeve injuries, consideration should be given to differential diagnoses for pathologies affecting the inferior pole of the patella in pediatric patients, such as isolated inferior pole fracture and Sinding–Larsen–Johansson (SLJ) syndrome, characterized by osteochondrosis of the inferior pole of the patella. 18 Devana et al. 13 reported patellar sleeve injuries may be differentiated through history, clinical features, and radiological findings. While it is interesting to note two cases described in the literature of a patellar sleeve injury occurring in a patient with SLJ syndrome, patients with SLJ were intentionally excluded from this study to remove ambiguity.18,19
Despite reports that non-operative intervention, even in minimally displaced cases, may lead to chronic patella alta or ossification of the patellar tendon,6,10 64 patients (71%) underwent non-operative management. None of these patients had patella tendon ossification on final radiographs and only one patient had patella alta, which was not statistically significantly different from the operative cohort in the subgroup analysis. The remaining 26 patients underwent operative treatment, the majority of whom (73%) had ORIF with transosseous suture fixation. While this study was neither designed nor powered for radiographic and clinical outcome comparison between patients undergoing different operative techniques, this would be interesting to examine more closely in future research.
Our subgroup analysis revealed clinical and radiographic differences between the operative and non-operative cohorts on their post-injury physical examination before treatment was commenced. A higher percentage of the operative group presented with an extensor lag or inability to fully extend the knee as well as a palpable defect about the patella. Radiographically, a higher percentage of the cohort who ultimately underwent operative management had a greater CDI with patella alta on presentation and a greater displacement between fragment and patella on plain radiographs. While MRI was performed in 28.9% of cases, it may be used in cases of high clinical suspicion to differentiate diagnoses, 13 exclude concomitant osteochondral fractures, 20 and provide additional information on the soft tissue–related injuries, such as the presence of bony edema or details on the avulsion fragment. 20 Of course, the nature of this study was not designed to analyze surgical indications, and it is certainly possible that the combination of the aforementioned findings led to the surgeons’ preferences to proceed with internal fixation.
Post-treatment outcomes revealed a statistically significantly higher CDI in the operative versus non-operative cohort; however, there was no difference in patella alta between the groups. That is to say, although the operative cohort had a higher post-operative CDI than the non-operative cohort post-immobilization alone, this higher CDI did not cross the threshold to be considered patella alta. Of note, medical record documentation revealed three patients with a post-treatment extension lag, all from the post-operative group; no patients from the non-operative group had a reported extension lag. The medical record did not specify the degree of residual lag, but it may very well be due to a greater preoperative fragment displacement or more extensive preoperative lag. Nevertheless, of the available documented return-to-sport outcomes, all but one patient (non-operative group) reported they were able to return to sport by their last documented follow-up appointment, indicating an excellent success rate following either treatment.
Given the rarity of this injury, a major strength of this retrospective study is its size, as the largest case series examining patellar sleeve injuries and management to date. In addition, we were fortunate that the detailed chart review included clear documentation of variables of interest, with 87.7% of patients (79 out of 90) with images available for review. Furthermore, the prospectively collected patient-reported outcome survey yielded a 30% return rate (27 patients), with overall excellent results and no specific differences in post-treatment pain or ability to return to the same level of sport between the groups.
Yet, this study must be considered in the context of several limitations. Inherent limitations are associated with a retrospective case series based at a single academic institution, such as incomplete medical records, poorly documented clinical exam findings, and lack of a formal control group. Moreover, the decision to progress with operative or non-operative treatment may have been influenced by the individual surgeon’s preference and prior experience or factors not considered in this study.
Interestingly, one patient was deemed to be skeletally mature, as the patient’s distal femoral physis was closed on plain radiograph. For the purpose of this study, skeletal maturity was recorded as binary data. Therefore, the skeletally mature patient, who was 17 years of age at the time of injury, may have demonstrated radiological closure of the distal physis though the patella may not be fully ossified. It was deemed suitable to include this patient within the overall cohort to serve as an important data point as a rare case and outside the previously estimated age range of 8–16 years. 5 Future studies may consider varying skeletal maturity, such as utilizing the Walls Classification system of physes being open, closing, or closed. 21
The response rate of 30% on a patient-reported outcomes survey at follow-up introduces potential nonresponse bias. Individuals who had worse outcomes may have declined participation in the follow-up survey or were unreachable despite several contacts. For instance, Mercier et al. 22 found that total hip arthroplasty patients who did not return the Hospital Consumer Assessment of Healthcare Provider and Systems survey were more likely to have had adverse events, readmission, or longer hospital stays. The prospective patient-reported outcomes survey was distributed by mail and by phone, though did not include clinical evaluation. While patients’ clinical outcomes were retrospectively recorded, there was no possible evaluation between patients’ clinical outcomes and patient-reported subjective outcomes at the same time point, which may limit the findings. Furthermore, while the patient follow-up is a strength of this study, the completion of a survey at a median of 3 months is susceptible to recall bias at the longer follow-up intervals and immature assessment at the shorter follow-up intervals. In addition, while there was no statistically significant difference found in the assessed functional outcomes between the operative and non-operative patients, it is possible that the study lacked sufficient power in its sample size to detect a significant difference if one, in fact, exists. Similarly, controlling for potential confounders was deemed inappropriate with this relatively modest sample size.
For these reasons, this study was primarily descriptive in an effort to provide a foundation for subsequent longitudinal, therapeutic, and prognostic observational investigations that will guide the development of an evidence-based management algorithm for patellar sleeve injuries in children. Further work would benefit from a prospective design with multi-institutional involvement to optimize statistical power. Future studies could investigate a specific “cut-off” displacement value to consider operative treatment. The difference in time to return to sport based upon treatment modality or specific operative technique can also be more closely analyzed. Given the variation in incidence identified in patellar sleeve fractures sustained from specific sports, such studies could help guide sports-specific prevention strategies and return-to-play recommendations.
This large case series provides valuable epidemiologic, demographic, and radiographic data describing patellar sleeve fractures, which can drive further research examining optimal management. While clinical and radiographic differences existed between patients with patellar sleeve fractures treated operatively versus non-operatively, in our series, patient-reported outcomes and return to sport were comparable between groups.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241228167 – Supplemental material for Management and subsequent outcomes of patellar sleeve injuries: A retrospective case series of 90 pediatric and adolescent patients
Supplemental material, sj-pdf-1-cho-10.1177_18632521241228167 for Management and subsequent outcomes of patellar sleeve injuries: A retrospective case series of 90 pediatric and adolescent patients by Joseph L Yellin, Aliya G Feroe, Ian T Watkins, Helena Franco, Borna Guevel, Daniel B Haber and Mininder S Kocher in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Joseph L Yellin: Study design, performed measurements, statistical analysis, manuscript preparation.
Aliya G Feroe: Study design, performed measurements, manuscript preparation.
Ian T Watkins: Performed measurements, manuscript preparation.
Helena Franco: Performed measurements, manuscript preparation.
Borna Guevel: Statistical analysis, manuscript preparation.
Daniel B Haber: Performed measurements, manuscript preparation.
Mininder S Kocher: Study design, performed measurements, statistical analysis, manuscript preparation, supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was received by the Boston Children’s Hospital Institutional Review Board (IRB approval number: IRB-P00027132). As a retrospective study, informed consent was not provided.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.