
Abstract
Purpose:
Management of Blount disease in adolescents and young adults is complex and associated with high risk of morbidities. Gradual correction with external fixator can minimize soft tissue injury and allow subsequent adjustment in degree of correction. This study investigates the surgical outcome and complication rate of gradual correction of neglected Blount disease through single-level extra-articular corticotomy.
Methods:
Patients treated for Blount disease using external fixator from 2002 to 2016 were recruited for the study. We used Ilizarov and Taylor Spatial Frame (TSF) external fixator to perform simultaneous correction of all the metaphyseal deformities without elevating the tibia plateau. Surgical outcome was evaluated using mechanical axis deviation (MAD), tibial femoral angle (TFA), and femoral condyle tibial shaft angle (FCTSA).
Results:
A total of 22 patients with 32 tibias have been recruited for the study. The mean MAD improved from 95 ± 51.4 mm to 9.0 ± 37.7 mm (medial to midpoint of the knee), mean TFA improved from 31 ± 15° varus to 2 ± 14° valgus, and mean FCTSA improved from 53 ± 14° to 86 ± 14°. Mean duration of frame application is 9.4 months. Two patients developed pathological fractures over the distracted bones, one developed delayed consolidation and other developed overcorrection.
Conclusions:
Correction of Blount disease can be achieved by gradual correction using Ilizarov or TSF external fixator with low risk of soft tissue complication. Longer duration of frame application should be considered to reduce the risk of pathological fracture or subsequent deformation of the corrected bone.
Introduction
Blount disease, also known as tibia vara, is a rare condition characterized by defective development of posteromedial area of the proximal tibia physis. 1 The condition was first described by Erlacher in 1922, 2 but later Blount reported his series with more details and noted two separate types, namely infantile and adolescent forms. 3 More recently some clinicians preferred to group them into early-onset and late-onset depending on whether the deformity was first noticed before or after the age of 4 years. In infantile or early-onset Blount disease, distal femur compensatory valgus deformity and depressed medial proximal tibia plateau are commonly noted. 4,5 They are also more likely to have bilateral involvements and less likely to be Black or male, as compared to their late-onset counterpart. 6 The etiology remains unknown, but it is most likely a combination of genetic and environmental factors. Natural history of Blount disease is progressive deformity associated with abnormal gait, reduced effort tolerance, and secondary osteoarthritis.
Most children with Blount disease would require surgery to realign the lower limb mechanical axis and maintain a horizontal knee joint. Surgical options include acute correction internal fixation, 7,8 growth modulation, 9,10 and gradual correction with external fixator. 11,12 Acute correction is associated with risk of complication, namely compartment syndrome, nerve injury, and limb length discrepancy. 13 External fixators allow subsequent modification in the degree of correction and lengthening of shortened tibia, especially in unilateral Blount disease. With new generation of hexapod external fixators, rotational deformity can also be corrected simultaneously. 14,15 However, gradual correction is not free from complication, especially for those with morbid obesity. 13
In developing countries, some patients with lower limb deformities presented late partly because the condition is relatively asymptomatic. Some would go for alternative traditional therapy, or just accept the condition as the will of God. There were very few reported series on treatment outcome of patients with neglected Blount disease who presented late as adolescents or adults. We decided to study the short-term surgical and radiological outcome for a group of these patients treated with gradual correction using ring external fixators.
Materials and methods
This is a retrospective clinical study on the patients with neglected Blount disease who presented as adolescents or young adults. After we obtained the approval of the institution’s Research Ethics Committee, we searched the department and hospital database for patients diagnosed with Blount disease from 2002 to 2016. All patients who have undergone gradual correction surgery using Ilizarov external fixators at the age of 10 years and above were included. Indication for gradual correction of genu varus deformity in our institution was tibial femoral angle (TFA) of more than 30° varus, and this was the recruitment criteria for this study. Clinical information and radiographs of patients were reviewed and analyzed. We contacted a few patients for missing information, and those who have incomplete data or genu varum secondary to other etiologies such as trauma or metabolic diseases were excluded.
Sagittal and coronal plane deformities were mainly evaluated using standing whole-limb plain radiography, while rotational deformity was determined by clinical assessment. In our setting, Blount disease with severe deformity is usually treated with gradual correction to reduce the risk of soft tissue complications. We use either Ilizarov (Smith and Nephew, Memphis, Tennessee, USA) or Taylor spatial frame (TSF) (Smith and Nephew) external fixator to correct all deformities in sagittal, coronal, and axial planes through a single-level proximal tibia corticotomy just below the tibia tubercle. Fibula osteotomy or resections were performed in all cases. We did not perform any intra-articular surgery like medial tibia plateau elevation or ligament reconstruction. No prophylactic lateral fasciotomy or release of peroneal nerve was performed.
Since most of our Blount patients were obese, we relied on one tensioned stainless steel wire (1.8 mm diameter), and three stainless steel half pins (5.0 mm diameter) to secure stable bone fixation of the proximal bone segment in the coronal and sagittal plains. The first procedure was to osteotomize, or resect a segment of fibula, depending on the severity of deformity. One wire was inserted just anterior to the fibula head, parallel to the knee joint represented by distal femur condyles (Figure 1(a)). Proximal ring was then fixed to the wire and tensioned to 110 kg. This was followed by fixation of the distal ring using a half pin over the anteromedial aspect of the tibia shaft. Once the position of external fixator frame was confirmed with C-arm, additional two half pins were introduced at the same level below the proximal ring from the anterior–medial and anterolateral aspects using two single hole Rancho cubes (Figure 1(b)). Both the half pins were slightly converging toward the posterior cortex, but they should not cross the midline of the tibia (Figure 1(c)). Two or three additional half pins were then inserted at different levels and preferably different planes to fix the tibia shaft. Percutaneous corticotomy were then performed. Once the complete break of the cortex had been confirmed, an additional half pin was introduced obliquely from the lateral aspect close to the corticotomy site (Figure 1(d)) to provide additional sagittal plane stability for the proximal tibia (Figure 1(c)). In most of our later patients, we performed percutaneous corticotomy through multiple drill holes created using a double-barrel drill sleeve with a guide tip (Figure 2) that was modified from innovative invention published by Yasui et al. 16

Fixation of ring fixator to proximal tibia. (a) Transverse wire fixation at the level of fibula head above the proximal ring. (b) Fixation of two half pins below the ring at the same level. (c) Cross section of upper tibia showing direction and placement of half pins below the proximal ring. (d) Oblique corticotomy below the level of tibia tubercle. (e) Oblique half pin in sagittal plane close to the corticotomy.

Double-barrel drill sleeve with guide tip used for corticotomy.
All our early cases were corrected using the Ilizarov external fixator. With the introduction of TSF in 2007, patients with clinical evidence of internal tibia torsion were treated with this type of hexapod external fixator. All deformities were corrected simultaneously, although further modification of the tibia length was common following subsequent radiographic evaluation at the end of angular and rotational correction.
All radiographic measurements were made by a single investigator (one of the authors) who had not been involved in treating the patients. Relevant radiographic parameters were measured from the last preoperative radiograph and the most recent follow-up radiograph for each patient, using the digital imaging software system (PACS, GE Healthcare, Chicago, Illinois, USA) digital imaging system. Metaphyseal diaphyseal angle and Langenskiold’s classification are not very useful in Blount disease in older children and adults. 17 We document and compare the deformities according to parameters described by Hefny et al. 18 Mechanical axis deviation (MAD) was used to evaluate the degree of lower limb malalignment. Although TFA was used to evaluate the coronal plane joint orientation/varus angulation in children, in adolescents and young adults, femoral condyle tibial shaft angle (FCTSA) may be more accurate because distal femur condyles are more reliable to represent the knee joint line, and angulation of tibia shaft to the condyles is probably a better guide to the degree of correction required. We also measured the angle of depressed medial tibial plateau (aDMTP) before surgery and on the last review (Figure 3(a) to (c)).
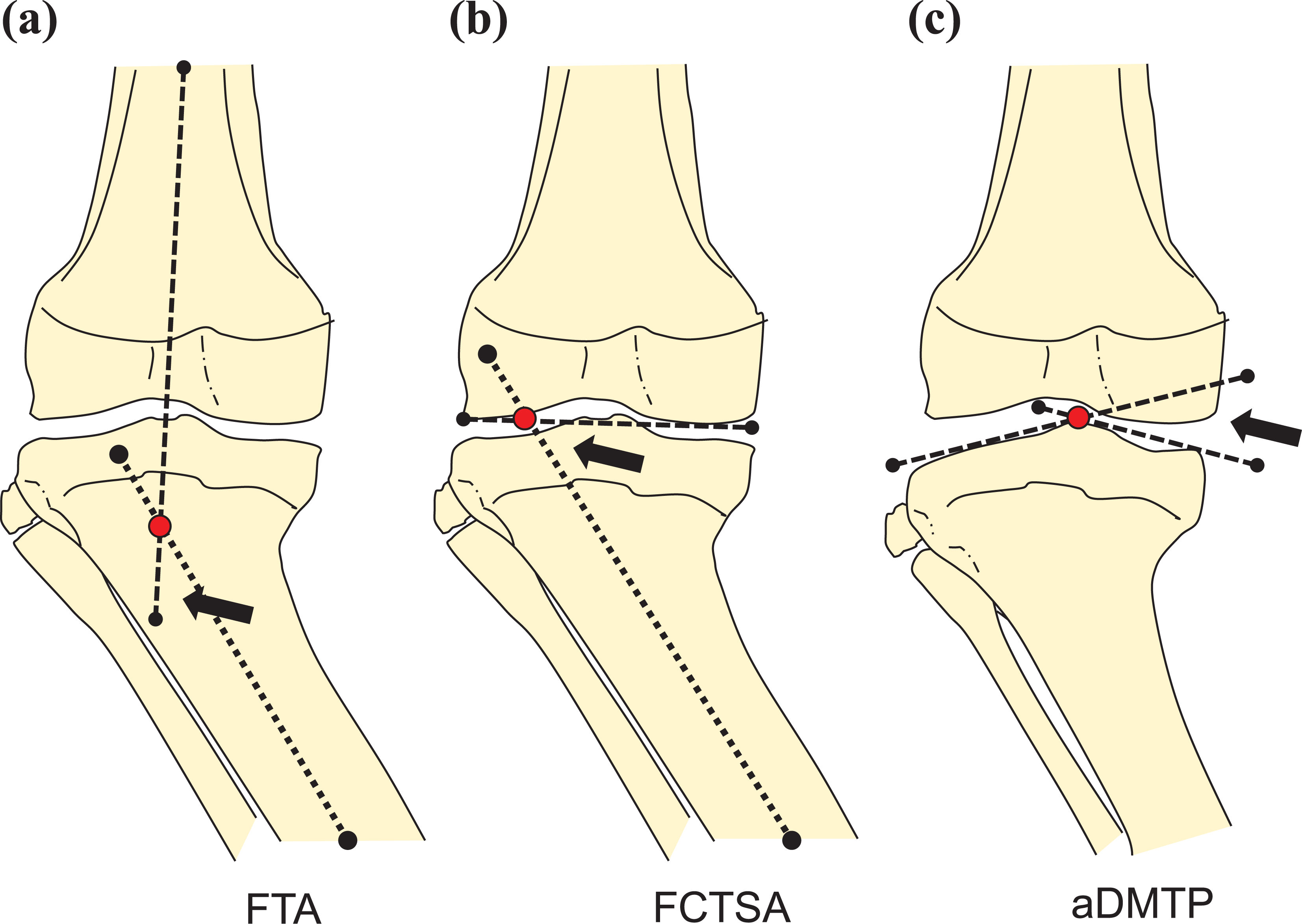
Radiological evaluations of proximal tibia genu varum. Black arrows indicate the measured angles: (a) TFA, (b) FCTSA, and (c) aDMTP. TFA: tibial femoral angle; FCTSA: femoral condyle tibial shaft angle; aDMTP: angle of depressed medial tibial plateau.
We do not have big sample population since there were not many patients with Blount disease presented for treatment after 10 years of age. The study is based on convenient sampling of all cases treated in our institution over the period of 14 years. The normality test was performed to determine the distribution of data. Based on the normality test using Shapiro–Wilk test, the data were normally distributed with p > 0.05. Since the data were normally distributed, further analysis using parametric test, that is, paired t-test, was performed. We will consider difference to be significant when the p value is less than 0.05.
Results
We identified 71 patients over the year of 10 years treated surgically for genu varum over the study period. Only 24 patients were diagnosed as Blount disease. Two patients were excluded due to incomplete follow-up data; therefore, we have 22 patients and 32 knees as our sample population (Table 1). Half of them have bilateral deformities (11 of 22) with slight male predominance (12 of 22). Five of them had early-onset Blount disease, while the remaining 17 were of late-onset category (Table 1). Only one patient with early-onset Blount disease had bilateral proximal tibia corrective osteotomy when he was 7 years old. He presented for bilateral gradual distraction at the age of 23 (Figure 4(a) to (c)).
Patient demographics and disease summary.
aEarly-onset: limb deformity observed before the age of 4. Late-onset: limb deformity observed at or after the age of 4.
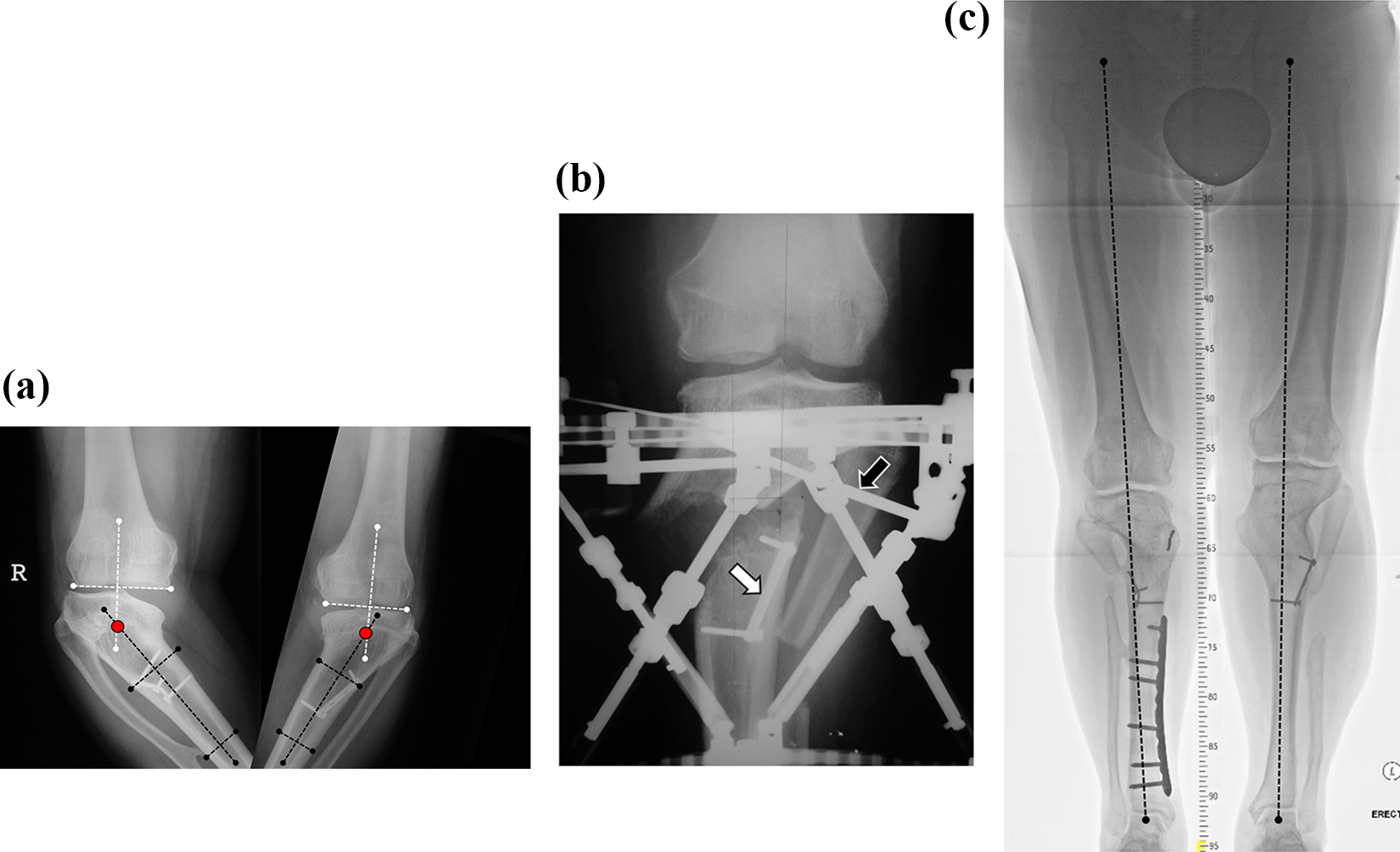
Bilateral Blount disease in a young adult treated with bilateral TSF fixators. (a) Close up antero-posterior knee radiograph showing FCTSA. Red dots indicate CORA. (b) Left knee antero-posterior radiograph showing placement of oblique half pin above the level of corticotomy in the sagittal plain (black arrow). Also shown is the old plate (white arrow). (c) Lower limb full-length standing radiograph on the last follow-up showing restoration of mechanical axes. Right tibia was treated for fracture that happened few years following treatment of Blount disease. TSF: Taylor spatial frame; FCTSA: femoral condyle tibial shaft angle; CORA: center of rotation of angulation.
Our study showed significant improvement in all the main parameters for limb alignment and bone/joint orientation after surgical treatment (Figure 4(a) to (c)) The mean MAD improved from 95 ± 51.4 mm (medial to midpoint of the knee) to 9.0 ± 37.7 mm (medial to midpoint of the knee). Mean TFA improved from 31 ± 15° varus to 2 ± 14° valgus, and mean FCTSA improved from 53 ± 14° to 86 ± 14°. Interestingly, we also noted a reduction in the mean aDMTP from 38 ± 11° to 26 ± 17°, despite the fact that no intra-articular procedures were performed for these patients (Table 2). All the changes were statistically significant (Table 3). The mean duration of external fixator application was 9.4 months (range 3.5–23.4 months). The mean follow-up duration of all patients is 43.3 months (range 9.6 months to 10 years). All children were skeletally matured on the last review.
Radiological outcome before surgery and on the last follow-up.

MAD: mechanical axis deviation; FTA: femoral tibial angle; FCTSA: femoral condyle tibial shaft angle; aDMTP: angle of depressed medial tibial plateau.
aMAD-positive values indicate mechanical axis is medial to knee joint.
bFTA-positive values indicate varus angulation at the knee.
Clinical outcome of gradual correction of deformity.

SD: standard deviation; MAD: mechanical axis deviation; FTA: femoral tibial angle; FCTSA: femoral condyle tibial shaft angle; aDMTP: angle of depressed medial tibial plateau.
a Positive MAD values indicate mechanical axis is medial to knee joint.
Two patients developed pin site infection which responded with oral antibiotics. One patient had delayed union requiring additional surgery for autologous bone grafting. A 24-year-old man who initially denied smoking turned out to be a chronic smoker. He defaulted follow-up for about 6 months, returned with delayed union and required bone grafting before the bone eventually united and consolidated after 23.4 months (Figure 5(a) to (d)). Two other patients had fracture at the osteotomy site after removal of the fixator frames. These patients required additional surgery to reapply with an external fixator, and both fractures eventually united without bone grafting. One patient had significant overcorrection of MAD of the left lower limb to MAD of 28.2 mm (lateral to knee joint center) following premature removal of the frame. The patient subsequently underwent acute corrective with closing-wedge osteotomy and internal fixation.

A young adult with left-sided proximal femur varus malunion. (a) Preoperative picture showing bilateral genu varum with mild internal tibia torsion. Left side was more severely angulated. (b) Preoperative radiograph showing left proximal tibia varus angulation with mild compensatory valgus angulation of distal femur. Varus deformity of the left knee appeared to be contributed by bowing of the femur. (c) Picture of patient just before frame removal showing correction of genu varus and internal tibia torsion of left lower limb. (d) Lower limb full-length standing radiograph on the last follow-up showing significant improvement of mechanical axes and good new bone formation following bone grafting for delayed union. We could not perform surgery for the right lower limb since he could not quit smoking.
Discussion
Mean age of our Blount disease patients at the time of surgery was 15 years (range 10–37 years), with slightly more males compared to females. Most other studies reported male predominance in Blount patients who presented late. 14,15,19
We manage to reduce the MAD from 97.4 mm to 7.5 mm medial to the midpoint of the knee. In a series of 23 patients (mean age of 14.7 years) with 25 tibias, Sachs et al. 15 reported MAD reduction from mean of 51.4 mm to 16.9 mm (medial to midpoint of the knee) by gradual correction using TSF. Another study by Li et al. 14 treating 14 patients with more severe deformity around the same age range reported MAD reduction from mean of 90 mm to 10 mm (medial to midpoint of the knee). Lower limb alignment measured by MAD depends not only on deformity of the bones but also on laxity of the knee joint. This is the reason why full-length standing (weight bearing) plain radiograph is essential to evaluate MAD of the affected limb.
TFA of our patients was corrected from mean value of 31° varus to 2° (valgus). We always try to achieve over-correction of about 5° (valgus) in growing children in anticipation of recurrence of deformity due to continuing inhibition the medial physis, but there is no clear guideline on this consideration. A study by Clarke et al. 20 reported correction of TFA from mean of 25.2° varus to 3.9° valgus in a group of children with mean age of 10.6 years, using four different types of ring and unilateral external fixator. In our study, FCTSA improved from 53° to 86°. We feel that this is probably a better measurement to evaluate proximal tibia deformity due to existing abnormality of tibia plateau in Blount disease. Hefny et al. 18 reported correction of FCTSA from 58° to 84° in a group of 12 children with the mean age of 9 years. They also performed correction of distal femur using Ilizarov fixator and simultaneous elevation of medial plateau elevation. In our series, we did not perform corrective surgery of the femur or tibia plateau. Schoenecker et al. 21 reported that medial plateau elevation is not necessary for most late-onset Blount disease since degree of depression is usually not much affected as compared to children with early-onset Blount. In our series, the mean aDMTP for all patients on the last follow-up was 26°, and all patients have reached skeletal maturity. Secondary changes in the medial column including thickening of medial meniscus and articular cartilage may contribute toward integrity of the medial column, despite the apparent depression evidence on plain radiography. 22
Two of our patients fractured the correction site while one other developed over-correction following removal of frame. These complications were mainly related to premature removal of the frame. Mean duration of 9.4 months for frame application was relatively long since generally we designed the frame to provide about 10–20 mm lengthening during the gradual correction. In nearly all cases of Blount disease, the center of rotation of angulation was located at the level of or proximal to the tibia tubercle. By performing the corticotomy below the tibia tubercle, we would expect some degree of translation across the bone cut as predicted by the second rule of osteotomy. 23 Obliquity of the newly regenerated bone do not provide the ideal mechanical stimulus for bone formation and consolidation. In addition, many Blount patients were overweight or obese. This would probably contribute toward longer than expected duration for frame application, and we would advise against early frame removal to reduce the risk of subsequent deformation or pathological fracture over the correction site.
The main limitation of our study was small number of patients. We were not able to recruit earlier cases because facility for treatment with gradual correction using external fixator was not available. We were not able to study changes in clinical finding related to the knee stability due to lack of consistent documentation of physical examination findings in these patients before treatment. Long-term outcome especially on the rate of degenerative arthritis will provide useful information on the actual benefit of treatment. For future findings, magnetic resonance images of intra-articular structures would be very useful to study the development of medical compartment soft tissue structures and cartilage under abnormal loading and changes after surgical realignment procedure.
Conclusion
Neglected Blount disease in adolescents and young adults is commonly complicated with severe and complex multiplanar deformity. Gradual correction with Ilizarov or TSF external fixator through a single-level corticotomy below the tibia tubercle can achieve good bone and limb alignment alignment with minimal risk of soft tissue complication. Longer duration of frame application is recommended to reduce the risk of pathological fracture and subsequent deformation of the corrected deformity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.