
Abstract
Introduction:
Defective mineralization of osteoid matrix prior to physeal closure causes rickets. Poor calcification of the cartilage matrix in the zone of provisional calcification causes flattened skull, rachitic rosary, bowed legs, coxa vara and brittle bones. The recent literature has seen an increase in the incidence of the disease in both developing and developed nations. We evaluated behaviour of lower limb deformities due to nutritional rickets in 117 patients.
Materials and methods:
A prospective study was conducted from January 2009 to December 2011 for clinical and radiological evaluation of knee deformities in nutritional rickets. A total of 117 patients with 198 coronal plane knee deformities between 2 years and 12 years age of rickets were enrolled in this study.
Results:
In our study, there were 65 genu varum and 133 genu valgum deformities. Seven genu varum (10.7%) and 37 genu valgum (28%) deformities were regarded as failure. Fifty eight genu varum got corrected completely obtaining an average of 5° of valgum in an average of 6.3 months. The average rate of spontaneous correction was 1.9° a month. Ninety six valgum got corrected obtaining an average of 4.7 valgum in an average of 13.3 months. The average rate of spontaneous correction was 0.92° a month.
Conclusion:
Most of the rachitic deformities get corrected with age. Genu varum is having better chances and a faster rate of correction as compared with genu valgum. Early surgery may be indicated in late presenting cases. We believe varum above 4 years and 18° of valgum above 9 years usually do not correct and may require surgical intervention.
Introduction
Defective mineralization of osteoid matrix of bones prior to their physeal closure causes rickets. There is poor calcification of the cartilage matrix in the zone of provisional calcification causing a wide variety of orthopaedic manifestations, including flattened skull, rachitic rosary, bowed legs, coxa vara and brittle bones. Vitamin D plays a pivotal role in calcium metabolism and its subsequent mineralization during the growth period. 1 It is ironic that, in spite being the only vitamin which body can synthesize from sunlight, vitamin D deficiency still remains common. The recent literature also shows an increase in the incidence of the disease not only in developing but also in developed countries. 2,3 Lower limb deformities, particularly coronal plane deformities around the knees, are among the most common rachitic deformities presenting in a paediatric orthopaedic clinic.
It is particularly difficult to define genu varum and genu valgum in paediatric patient owing to constantly changing tibiofemoral angle with age. Studies have define normal development of tibiofemoral angle. 4,5 However, the natural history of coronal plane knee deformities due to nutritional rickets has not been described in the literature for Indian population. We undertook this study with the aim to describe the coronal plane rachitic deformities and the rate of spontaneous correction of these deformities after vitamin D admiration and to define cases where conservative management fails.
Materials and methods
A prospective study of nutritional rachitic knee deformities was performed from January 2009 to December 2011. Institutional review board approval was sought prior to the study. Informed consent from parents or immediate guardians of all patients was sought in all cases.
Based on extensive literature regarding normal development of tibiofemoral angle, a working definition was formulated for the study. 4 –7 Varus angle above the age of 2 years or a valgus angle >12° was considered as abnormal in our study. The deformities in our study were measured both clinically and radiologically. Clinically, tibiofemoral angles and intercondylar and intermalleolar distances were noted in all patients initially and after 3-month interval as described below. On standing position with patella facing outwards, anterior superior iliac spine (ASIS), centre of patella and centre of ankle (point between midpoint of medial and lateral malleoli) were marked by using vernier caliper. Two lines joined ASIS to centre of patella and centre of patella to centre of ankle. By using goniometer, tibiofemoral angle was measured using the above lines. Intercondylar and intermalleolar distances were also noted in standing patient. 5 These clinical measurements were measured on all subsequent visits by the same personnel and recorded by different person to omit any bias.
The initial laboratory and radiological investigations included serum calcium, phosphorus and alkaline phosphatase (ALP) levels; X-rays of bilateral wrist; and scanogram of bilateral lower limbs. Other investigations such as kidney function tests, 24-h urinary calcium and phosphorous, parathormone and vitamin D levels were done on required basis. Patients with nutritional rickets were enrolled for the study and other causes of rickets and coronal deformities of knee were excluded. ALP levels of over 450 IU/L were regarded as abnormal along with classical radiographic signs of rickets, that is, widened physis with cupping and fraying of metaphysis. The patients were divided as mild (0–4), moderate (4–7) and severe rickets (>7) on the basis of radiological score proposed by Thacher et al. 8
Children with nutritional rickets were treated by vitamin D supplementation and dietary intake of calcium and phosphorus. Supplementation of vitamin D was given by stoss therapy. 9,10 Intramuscular route was preferred as it was economical and better compliance rate than oral route. Patients were also started on oral calcium. The children were also advised adequate dietary calcium, phosphorus and adequate sunlight. 1,11 These patients were reassessed after 3 weeks with repeat ALP and X-rays. Decrease in ALP and healing line on X-rays were regarded as favourable outcome (Figure 1(a) and (b)). Those with no decrease in ALP or healing line on X-rays were given a second dose of 600,000 IU of vitamin D intramuscularly. These were re-evaluated after 3 weeks. Those not responding were excluded from the study and were evaluated for other causes of rickets. No bracing of any sort was used in any case.

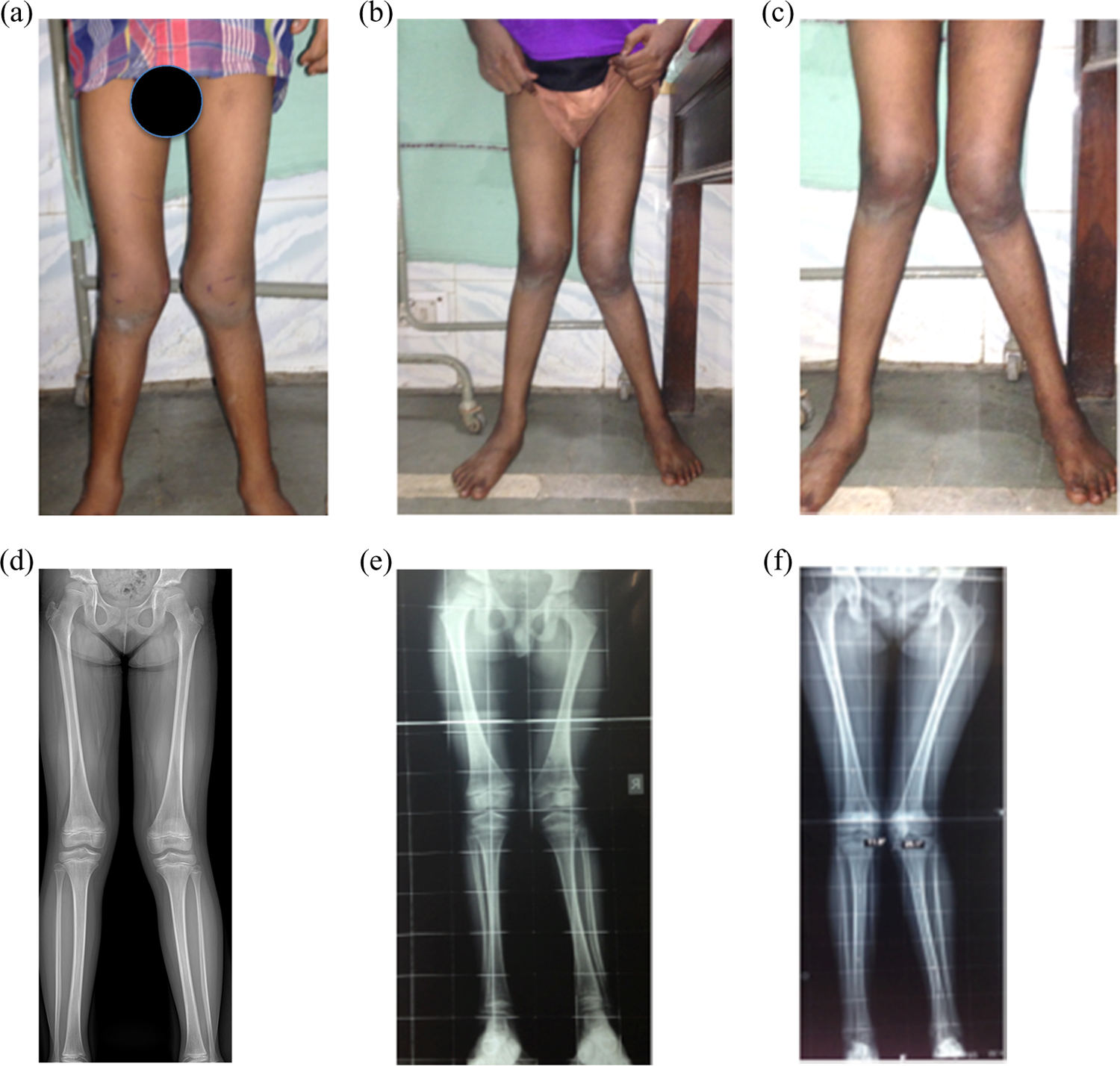
(a) Clinical photographs of 7-year-old child with bilateral genu valgum deformity with rickets. Note the prominence of bilateral malleoli. (b) to (d) Serial photographs of same child after rachitic treatment at 6 weeks, 3 months and 7 months. Note the complete correction of deformity. (e) AP X-ray of knee of same child at 3 weeks after treatment with vitamin D. Note valgus deformity, with signs of rickets healing. White line of healing is prominent. (f) to (h) Serial scanograms of same child at 6 weeks, 3 months and 1 year. Note compete resolution of deformity.
The subsequent visits were made at 3-month interval. No improvement in angle for 12 months or any further deterioration on subsequent visit was regarded as failure of conservative management. All patients were followed for minimum 3 years after correction of deformity.
Statistical analysis
All quantitative variables were expressed as means ± standard deviation. All patients were divided in one of two groups based on outcomes – favourable or unfavourable. Patients responding to conservative treatment were regarded as favourable group while those requiring surgery as unfavourable group. Student’s t-test was used for normally distributed continuous variables (age and body mass index (BMI)) and Mann–Whitney t-test was used for non-normally (degree of deformity) distributed variables to compare parameters between genu varum/valgum patients or favourable/unfavourable groups.
Results
We observed 243 knee deformities in 143 patients over 3 years due to rickets. Twelve of these patients with 19 knees were not able to complete the study and were lost to follow-up. Fourteen patients with 26 knees had rickets due to cause other than nutritional rickets. The distribution of these patients is shown in Table 1. Results of 198 knee deformities in 117 patients are presented below.
Causes of non-nutritional rickets in the study.

The average age of the patient in our series was 6.3 years (2–12 years). Seventy-nine patients had genu valgum, 33 patients had genu varum and 5 patients had wind swap deformity (Figure 1(a) to (c)). All the patients were of Indian origin (North India).
Tables 2 and 3 give age and sex distribution of genu varum and valgum deformities, respectively. We observed that most children with genu varum were under the age of 5 years, while those with valgum deformities were over the age of 5 years. However, in both groups, younger patients generally had bilateral deformities and older patients had unilateral deformities. Average age in bilateral genu varum cases was 2.8 years compared with 4.1 years in unilateral genu varum cases (p = 0.01). Similarly, average age of bilateral genu valgum was 2.8 years compared with 9.1 years in unilateral cases (p = 0.001).
Age and sex distribution of cases of genu varum.

Age and sex distribution of cases of genu valgum.
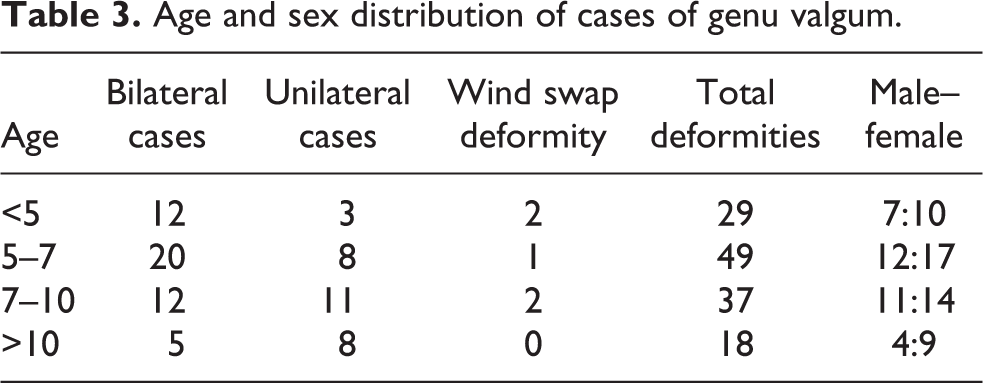
Table 4 compares the clinical features and outcomes in both the deformities. Both deformities not only showed striking differences in presentation but also in terms of their response to treatment. Tibia was found to be the most important contributing bone in cases with genu varum, while femur was exclusively the cause of deformity in genu valgum. Another important finding was that not only most rachitic genu deformities get corrected with time on conservative management; the rate of correction was much faster than genu valgum, which failed to achieve correction in 28% cases (Figures 1(a) to (h) and 2(a) to (g)). Figure 3(a) and (b) shows the scatter diagram of correction of deformity of genu varum and valgum, respectively. It shows that varum deformity was not only earlier to correct, but the rate was faster than genu valgum deformity. Mean time for correction for genu varum was 6.3 months and genu valgum was 13.3 months (p = 0.000). However, in both groups, the correction of deformity was not found to be related to initial severity of presentation as determined by the radiological score proposed by Thacher et al. 8
Clinical and radiological comparison of genu varum and valgum deformity.a
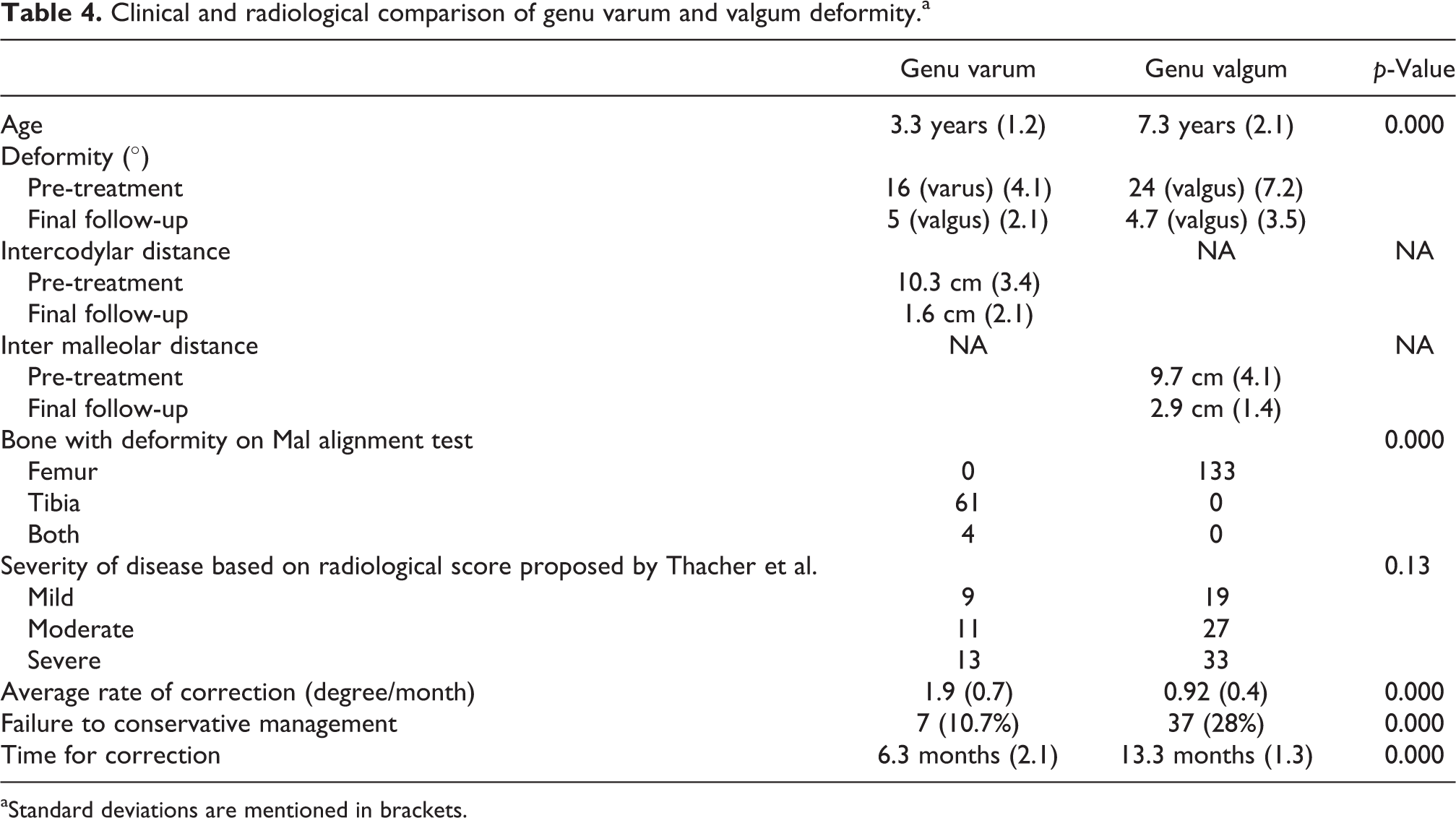
aStandard deviations are mentioned in brackets.

(a) Clinical photographs of 2.5-year-old child with bilateral genu varum deformity with rickets. (b) to (d) Serial photographs of same child after rachitic treatment at 6 weeks, 3 months and 5 months. Note the complete correction of deformity. (e) AP X-ray of bilateral lower limbs of the same child with rachitic changes. (f) AP X-ray of bilateral lower limbs of same child at 6 weeks with healing of rickets. (g) Scanogram of the same child at 6 months with complete correction of deformity.

(a) and (b) Scatter diagram showing rate of correction of deformity in genu varum and valgum. Note the faster rate and earlier correction of genu varum deformity compared with genu valgum. Most varum deformity got corrected by 6 months, whereas valgus deformity took 9–12 months.
In order to find out factors that can predict the prognosis of coronal plane deformities, both the deformities were divided in favourable and unfavourable groups based on success or failure of conservative treatment (Table 5). Presenting age was the most important factor contributing to success of conservative management (Figure 4(a) and (b)). The chances of spontaneous correction were inversely proportional to age of the patients. Little spontaneous correction occurred after 4 years in cases of genu varum and after 9 years in genu valgum (Figure 5(a) to (f)). Sex, BMI, height, weight, bone contributing to deformity and severity of rickets at initial presentation were not found statistically significant. Similarly, initial ALP and vitamin D levels were not related to prognosis of the deformity. However, we found that in unfavourable cases, ALP levels took significantly larger time to return to normal value compared to favourable cases in all coronal plane deformities (3.2 weeks vs. 4.1 week, p = 0. 031). Degree of initial deformity was not significantly related to prognosis of genu varum patients, but, interestingly, it was found significantly related to the outcome of genu valgum patients. Larger deformities over 18° were more commonly associated with surgical treatment compared with deformities less than 14° in cases with genu valgum.
Comparison of favorable and unfavorable cases in genu varum and valgum cases.

M: male; F: female; ALP: alkaline phosphatase; b/l: Bilateral; u/l: Unilateral.

(a) and (b) Bar graph showing rate of correction is dependent on age for both genu varum and valgum.
Clinical photographs of 9-year-old child with bilateral genu valgum deformity with rickets. Rickets was confirmed by raised ALP levels and decreased vitamin D levels. (b) and (c) Serial photographs of the same child with worsening of deformity at 3 and 6 months despite rachitic treatment and calcium supplementation. However, lab parameters were normal in all subsequent visits. (d) to (f) Scanograms of the same child at 3 weeks, 6 months and 12 months with no improvement and subsequent worsening. The child was subsequently taken for growth modulation. ALP: alkaline phosphatase.
Failure rate was also lower in genu varum compared with genu valgum (10.7 vs. 28%, p = 0.000). Surgical correction was undertaken for patients who failed to respond to conservative management. Growth modulation was done with patients having adequate growth left in both genu varum and valgum. Patients nearing skeletal maturity were treated with osteotomy. Genu valgum was treated with ‘V-type’ chevron osteotomy, while high tibial open-wedge osteotomy was done for cases with genu varum.
Discussion
The important findings of our study are most rachitic deformities that show spontaneous correction after restoration of metabolic deficiency without the use of brace or any surgical intervention. Genu varum not only has a better chance of complete resolution, but the rate of resolution is also faster compared with genu valgum deformity. The age of presentation is most important parameter that affects the success of conservative management. The extent of deformity is more important in cases of genu valgum compared with genu varum.
Salenius and Vankka in 1975 described normal clinical tibiofemoral angles in 1279 children. 4 They showed mean varus alignment of 15° was attained at neonatal period and decreased to approximately 10° of varus by the age of 1 year. At the age of 18–20 months, it becomes neutral and maximum valgus of approximately 12° was reached by 3–4 years of age. By the age of 7 years, normal valgus of 8° in women and 7° in men were achieved. Similar studies in Indian population showed varus alignment before the age of 2 years and then valgus alignment with maximum valgus 11–12° by the age of 3–4 years and 7°–8° of valgus by the age of 7–8 years. 5 This data formed the basis of working definition for our study. It was seen that physiological varus in all studies usually disappears by 2 years of age; therefore, any varus above this age is not normal and maximum valgus achieved is usually 12°, so a value at any age higher than this was regarded as abnormal.
Nutritional rickets is caused by dietary deficiency of vitamin D or calcium or both. 1 The burden of disease has increased in recent times not only in developing but also in developed nation. 2,3 Although rickets cause number of skeletal deformities, knee deformities owing to rapid growing physis are most common. 1 However, to the best of our knowledge, description of behaviour of rachitic deformities and their behaviour and rate of resolution with correction of deficiency have never been described.
Rickets primarily affects the growing physis and results in exaggeration of the physiological deformity. 1 This might be the reason of genu varum to be common before 5 years and valgum to be common after 5 years. No direct comparison has been made in the literature regarding age of varum or valgum in rachitic deformities; however, Aggarwal et al. in their study of adolescent nutritional rickets showed that 16 of 19 deformities were genu valgum. 12 Similarly. Echarri et al. showed only 16% cases in less than 5 years had genu valgum. 13 Another interesting finding was younger patients in both groups had bilateral deformity; however, unilateral deformity mostly occurred in older patients. Again, we did not come across any direct comparison; however, we noted that Agaja in their study of rachitic deformity in 0–5 years found over 80% deformity to be bilateral. 14 On the other hand, Das et al, in their study of patients from 5 years to 15 years, noted bilateral cases only in 8 of 54 cases. We believe more research on the topic may be required to find out the reason for this finding. 15
We observe that genu varum was corrected faster and more commonly than genu valgum. No such reference was found in literature regarding knee deformities. We feel that reason for this can be probably due to the fact that normal response is increasing valgus angle till 4–5 years, which helps the varus deformity. However, no such physiological ‘help’ is given to cases of genu valgum, in which most cases present after 6–7 years when the adult alignment is already reached.
Based on our observations, we believe that no orthotic or surgical intervention may be required for correction rachitic deformities, particularly genu varum. In the past, plaster correction and braces have been used for such deformities. 16 However, genu varum above the age of 5 years and genu valgum larger than 18° over 9 years may not be correct. Therefore, in such cases, a usual waiting period of 1 year used by most authors may not be required and early surgical intervention with growth modulation may help the treating surgeon to take full advantage of second growth spurt. 15
There are lots of strengths of our study. Firstly, we have a very large sample size. We believe that this is the first study to take into account such a large age group (2–12 years) with both the deformities and compare the nature of these deformities simultaneously. Also, this is the first attempt to define the rate of correction of both the deformities after correction of nutritional deficiency. Then, the indications for surgical intervention are better described. However, the study is not without limitations. Since such large age group is observed, not all parameters affecting the deformity at each age can be studied. Secondly, definition of failure of treatment was arbitrary, but we believe waiting for 12 months for resolution was enough. Deformities not decreasing in magnitude by 12 months would be less likely to do so in future.
Conclusion
The study concludes that most rachitic deformities get corrected with age. Genu varum has better chances of correction (90% in our series) compared with genu valgum (72%). The rate of correction is also faster in genu varum compared with valgum. The nutritional rickets is managed effectively by early diagnosis and vitamin D supplementation and prevention of vitamin D deficiency. Early surgery may be indicated in late presenting cases. We believe varum above 4 years and 18° of valgum above 9 years usually do not correct and may require surgical intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.