
Abstract
Introduction:
Coronal plane knee deformities are frequent in children and may arise from idiopathic or nonidiopathic causes, leading to cosmetic, functional, or early degenerative issues. Guided growth using tension band plates is an established corrective method, but its predictability – especially in nonidiopathic cases – needs further evaluation. This study analyzed correction rates (CR) and treatment outcomes in different etiologies.
Methods:
A retrospective review included patients treated for coronal plane deformities with tension band plates from 2009 to 2021. Patients were classified according to etiology. Radiographic measurements (mechanical axis deviation, mLDFA, and mMPTA) were compared between baseline and end of correction. Analyses regarding treatment success, CR and predictors for CR and success were performed.
Results:
The analysis included 654 growth modulations in 313 children; distal femur (55.4%), proximal tibia (44.6%), both (42.2%. The average CR for mLDFA was 0.67 (+/−0.55)°/month and for mMPTA 0.43 (+/−0.38)°/month. CR significantly varied by etiology (p < 0.001), with older age at surgery and varus deformity predicting lower CRs. Neutral mechanical axis was achieved in 68.7% of patients. Significant differences between etiologies were seen, and complete correction was achieved significantly more often in patients with idiopathic etiology compared to nonidiopathic etiologies; 78.2% vs. 66.3% respectively, p = 0.02.
Conclusion:
Hemi-epiphysiodesis is effective for correcting coronal plane deformities in children, but CR differs by etiology and incomplete correction is not uncommon. These factors should inform treatment planning and follow-up.
Level of evidence:
Level IV, case-series
Introduction
Angular coronal plane deformities around the knee1–3 are encountered relatively frequently in children due to disturbances in skeletal growth. A broad range of idiopathic and nonidiopathic etiologies lead to either varus or valgus deformity. 4 Depending on the severity, lower limb angular deformity may lead to cosmetic complaints, functional problems, pain, gait disturbances, and subsequently joint degeneration.5–8
Temporary or permanent hemi-epiphysiodesis is an elegant way of correcting lower extremity deformity in the growing child.2,4,9 Although several techniques exist, the use of tension band plates, as introduced by Peter Stevens, is a popular method. 9
Challenges remain regarding the predictability and outcome for guided growth as a method of deformity correction.10,11 Reports on the correction rates and outcome for nonidiopathic cases are limited to smaller series, and there is limited comparison between the underlying etiologies.12–15
Our objective was to analyze correction rate (CR) and treatment success in the management of angular coronal plane lower limb deformities in idiopathic and nonidiopathic etiologies. We also aimed to assess other factors influencing CR and treatment success.
Methods
Following approval from the institutional ethical review boards (reg. no. SE21.03 and MEC-2023-0673), a retrospective cohort study was performed at The Royal National Orthopaedic Hospital, Great Ormond Street Hospital, and Erasmus MC – Sophia Children’s Hospital
Patient selection
We included patients treated with hemi-epiphysiodesis using tension band plates at the distal femur and/or proximal tibia for coronal plane angular deformity around the knee in the period 2009 to 2021. Other inclusion criteria were the availability of appropriate long leg radiographs at baseline and follow-up until skeletal maturity or deformity correction, defined as the moment when the tension band plate was removed.
Limb segments were excluded from the analysis if a concurrent alignment corrective osteotomy of the same segment (femur or tibia) had taken place either at the time of tension band plate insertion or during the guided growth correction period.
The same surgical technique and treatment principals were followed throughout the study period in all three institutions. 9 All procedures were performed under general anaesthesia. For each segment, through a 2–3 cm incision, a single tension band plate was placed on the convex side of the deformity and fixed with two cannulated cancellous bone screws. Specifically, either the PediPlates (OrthoPediatrics, Warsaw, IN) or the eight‑Plate Guided Growth System (Orthofix Srl, Verona, Italy) was used depending on institution and availability. The plates were placed on the periosteum, in a submuscular and subfascial position. Screws were positioned to avoid physeal damage and joint penetration, and the plate was positioned centrally on the physis in the sagittal plane. Hardware position was verified intraoperatively using fluoroscopy. Postoperatively, full weightbearing was allowed and early mobilization encouraged.
Measurements
The following demographic details were obtained from the patient records: gender (female or male), age (years), side affected (left, right or bilateral), type of deformity (whole limb varus/valgus, as assessed by positive or negative mechanical axis deviation, MAD), segment affected (femur and/or tibia), associated interventions such as corrective osteotomy at an adjacent segment and complications during treatment.
Underlying aetiology was recorded for each patient, and these were categorized into eight groups:
Idiopathic
Congenital longitudinal reduction defects (including femoral, tibial or fibular dysplasia)
Blount’s disease
Skeletal dysplasia (including achondroplasia, hereditary multiple exostosis, multiple epiphyseal dysplasia)
Rickets (predominantly nonnutritional subtypes)
Metabolic disorders (including mucopolysaccharidosis)
Acquired growth disturbance (trauma, infection, avascular necrosis)
A ‘complex’ group encompassing children with underlying genetic and/or neuromuscular conditions which were not classifiable into any other distinct group. All lower limb physes in these children appeared radiographically normal.
Radiographic measurements were performed on digital standardized standing long leg AP radiographs. These were considered appropriate when all landmarks for measurement of mechanical axis and joint line angles were visible and patellae were facing forward to avoid rotational errors. In patients with a leg length difference, this was equalized during imaging using a corresponding block under the shorter leg.
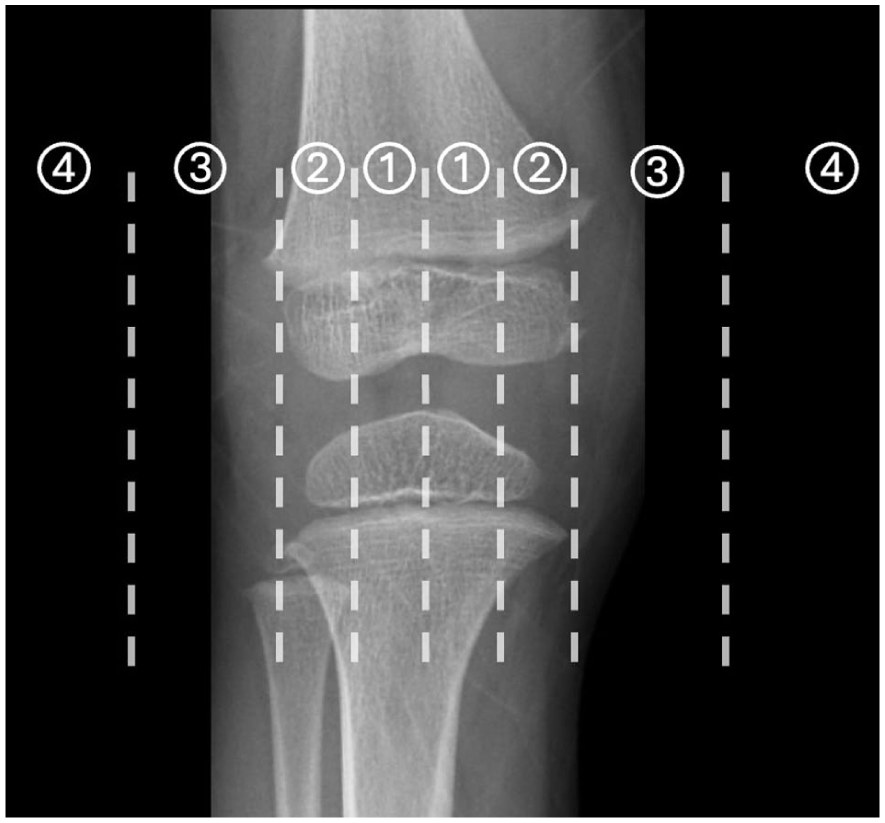
All measurement were performed using Traumacad (Brainlab company, Munich, Germany). 16 Mechanical axis deviation was divided into four zones as described by Stevens. 17 (Figure 1) Mechanical lateral distal femur angle (mLDFA) and medial proximal tibia angle (mMPTA) were measured in degrees.
Baseline radiographic measurements (T0) were obtained on the radiograph taken prior to plate insertion surgery. Follow-up measurements (T1) were performed either on the last radiograph before plate removal surgery or at the first follow-up at skeletal maturity in patients where plates were not removed before the end of growth. Baseline and follow-up dates were defined for each segment separately.
Analysis
Descriptive statistics were presented as means with standard deviations or median and interquartile range for continuous variables depending on data distribution and as counts and percentages for discrete variables.
Correction time was calculated as the time between T0 and T1. Correction rate was calculated as the change in mLDFA or mMPTA divided by the correction time in months and reported as degrees/month. Correction time and correction rate analyses were performed on a limb segment level (i.e. for femur and tibia on each side separately).
A comparison of correction rate in patients with different underlying etiologies was performed using ANOVA or Kruskall–Wallis test depending on normality of data distribution.
Analysis of factors influencing correction rate, corrected for underlying aetiology was performed using linear regression modelling. Candidate predictors were age at surgery, sex, type of deformity and severity of initial deformity.
Treatment success was defined as achieving a mechanical axis in zone 1 at the end of the correction period. Undercorrection was defined as a mechanical axis falling in zone 2 or higher on the same side as the initial deformity, while overcorrection was defined as a mechanical axis falling in zone 2 or higher on the opposite side of the initial deformity (varus to valgus or vice versa). Analysis for mechanical axis correction was performed on a limb level. For analysis of the mechanical axis we excluded patients who had had an acute correction of the other segment of the ipsilateral limb. Treatment success stratified for aetiology was compared using chi-square test and analysis of factors influencing treatment success was performed using logistic regression modelling, with age at surgery, sex, type of deformity, affected segment and severity of initial deformity as candidate predictors.
For all analysis statistical significance was set at p < 0.05.
Results
Six hundred and fifty four completed growth modulations in 313 children were included for analysis. Hemi-epiphysiodesis was performed at the distal femur in 362 cases (55.4%) and the proximal tibia in 292 (44.6%), in 276 cases (42.2%) both were addressed. Baseline demographics are presented in Table 1.
Patient characteristics.
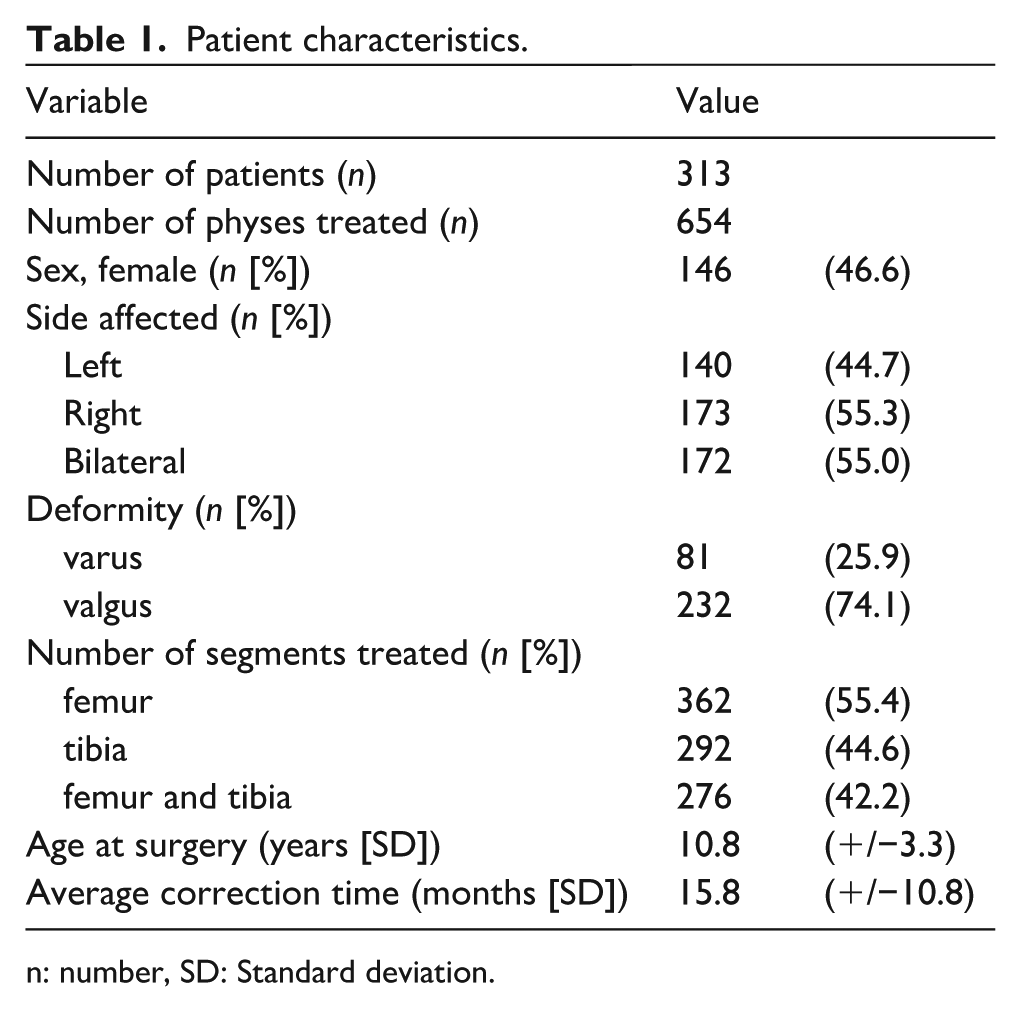
n: number, SD: Standard deviation.
The overall average CR of the mLDFA was 0.67 (+/−0.55)°/month and for mMPTA 0.43 (+/−0.38)°/month.
Both femoral and tibial growth modulations showed significant differences in CR between etiologies (p < 0.001 and p < 0.001, respectively, one way-ANOVA). For tibial growth modulation, slowest correction rates were seen in patients with skeletal dysplasias and metabolic conditions, with fastest correction rates occurring in those with a longitudinal reduction defect or rickets. For femoral growth modulations, slowest correction rates were again observed in those with a skeletal dysplasia and highest rates again in patients with rickets. A detailed description of correction rates is presented in Table 2.
Patient distribution and deformity correction rate according to underlying aetiology.
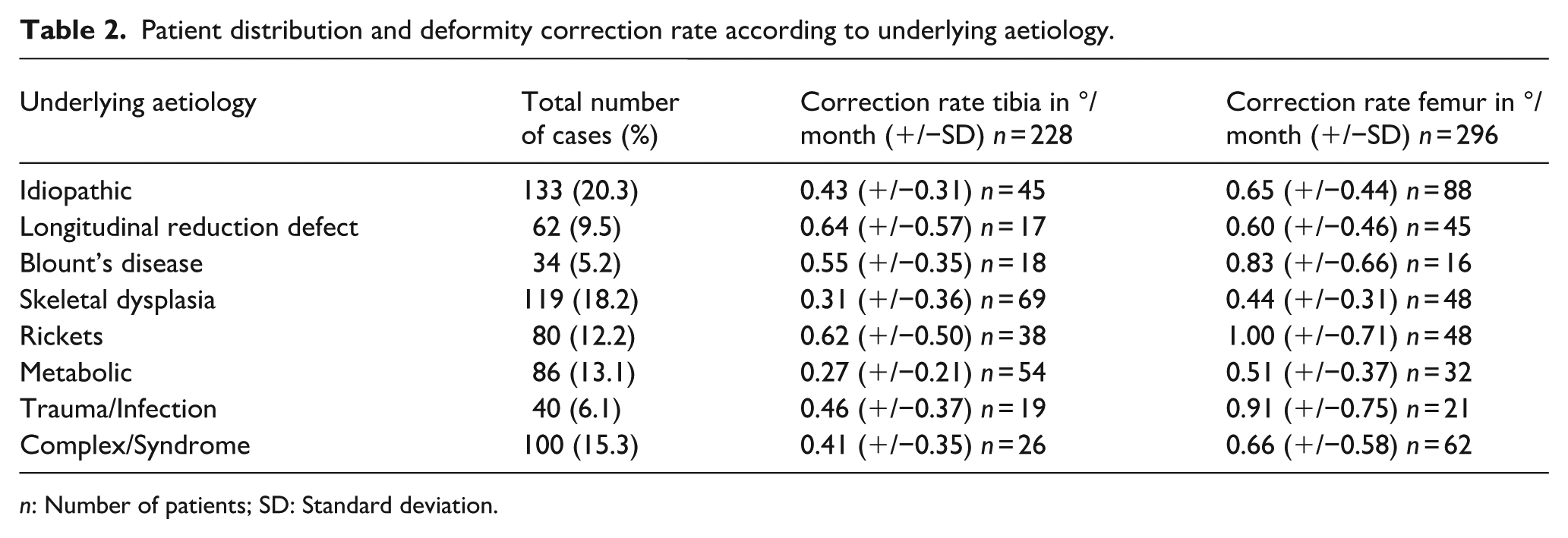
n: Number of patients; SD: Standard deviation.
Multiple linear regression analysis, corrected for underlying aetiology, showed that higher age at surgery was an independent predictor of lower CR both in the femoral and tibial corrections (p < 0.001; Table 3). Moreover, for femoral corrections varus deformity was related to lower CR’s (p = 0.006). Overall, model fit for the mLDFA correction rate model was adjusted R2 = 0.268 and for the MPTA correction rate model adjusted R2 = 0.190.
Linear regression of factors influencing correction rate.
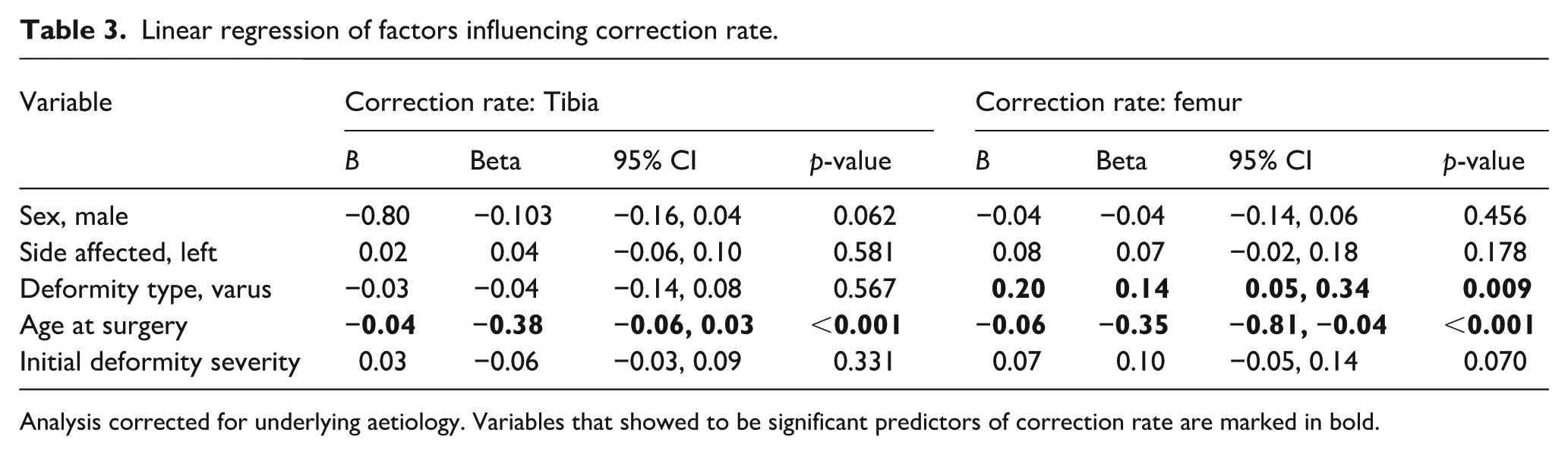
Analysis corrected for underlying aetiology. Variables that showed to be significant predictors of correction rate are marked in bold.
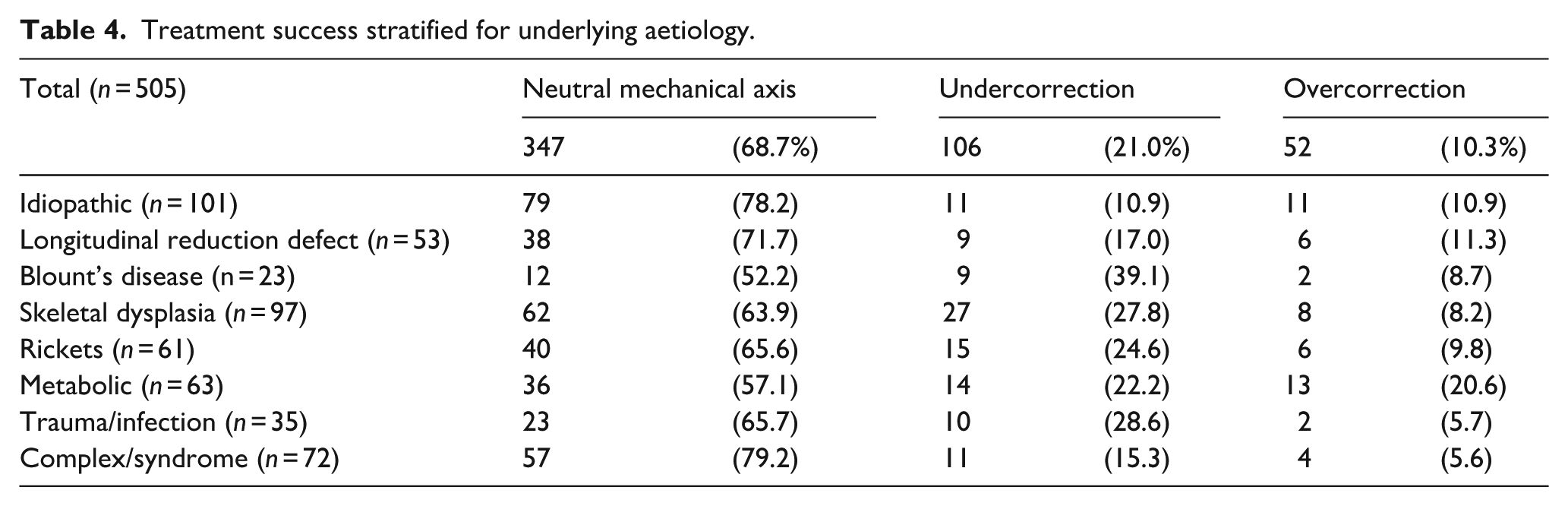
Distribution of mechanical axis zone at baseline and correction achieved at the end of correction is presented in Figure 2. Overall, a neutral mechanical axis was achieved in 347/505 limbs (68.7%) treated with guided growth. A total of 106 limbs were under corrected (21.0%) and 52 overcorrected (10.3%) at the end of the guided growth period. The highest success rate was seen in idiopathic cases, and lowest in patients with metabolic disorders and Blount’s disease (Table 4). The between-group differences were statistically significant (p = 0.042 Chi-square). Overall, complete correction was achieved significantly more often in patients with idiopathic aetiology compared to nonidiopathic etiologies; 78.2% vs. 66.3%, respectively, p = 0.021 chi-square.
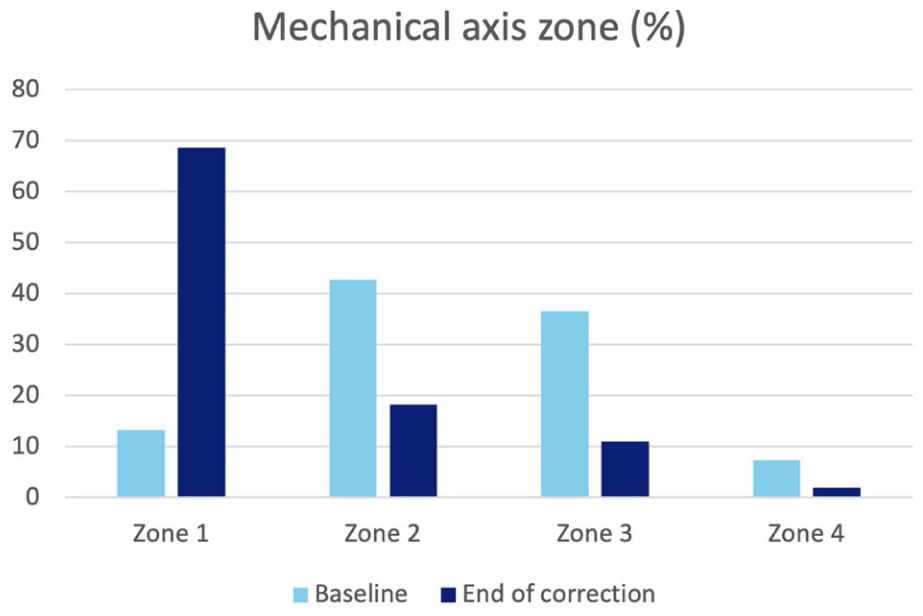
Mechanical axis distribution of patients in Stevens zones, at baseline and at the end of guided growth correction period.
Treatment success stratified for underlying aetiology.
Predictors for under- and overcorrection are presented in Table 5. Patients with higher age at surgery, varus deformity and more severe initial deformity are at significantly higher risk of undercorrection. Overall goodness of fit of the model was Nagelkerke R2 = 0.174. Patients with lower age were at higher risk of overcorrection, overall goodness of fit of this model was R2 = 0.076.
Logistic regression of risk factors for under- and overcorrection of the mechanical axis.
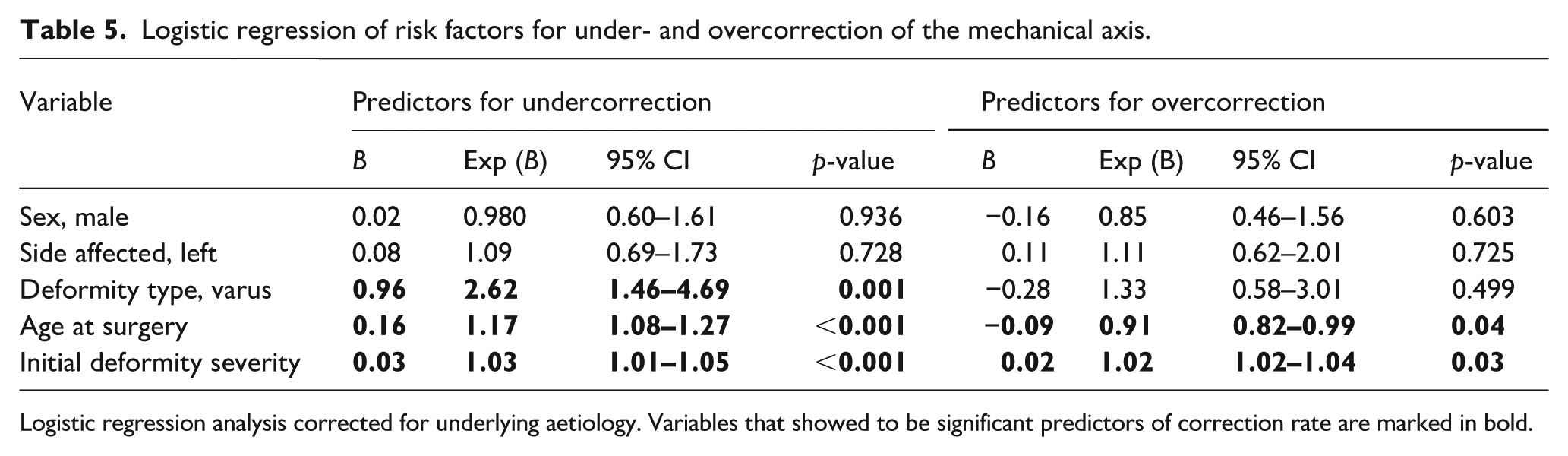
Logistic regression analysis corrected for underlying aetiology. Variables that showed to be significant predictors of correction rate are marked in bold.
Discussion
The main study findings were that both correction rate and treatment success varied significantly depending on the underlying aetiology. CR significantly varied by aetiology with older age at surgery and varus deformity predicting lower CRs. A neutral mechanical axis was achieved in 68.7% of patients, with also significant differences between etiologies seen and complete correction achieved significantly more often in patients with idiopathic aetiology compared to nonidiopathic etiologies.
The average correction rate of guided growth for coronal plane deformities around the knee has been reported in several studies.11,20 Overall, average correction rates of 0.87 °/month (0.65–1.0) for the distal femur and 0.72 °/month (0.5–1) for the proximal tibia have been reported. 20 Our correction rates (0.67 (+/−0.55)/month for the femur and 0.43 (+/−0.38) /month for tibial corrections) are slightly slower, but this could well be explained by the relatively large proportion of non-idiopathic cases in our cohort. Furthermore, it must be noted that the distribution of correction rates we report is quite broad, which is also in line with literature.11,20
Another point that warrants discussion is the distribution of varus and valgus deformities in our cohort, with one-quarter being varus cases. This makes varus deformity slightly more frequent in our series than in previously published series on guided growth in idiopathic deformities. 11 This is likely due to the broader range of etiologies included – such as Blount disease, metabolic conditions, and other complex pathologies – which are more frequently associated with varus malalignment. Despite the predominance of valgus deformities, our sample size remained robust, comprising 81 patients and 159 varus segments treated with guided growth. We therefore consider the cohort sufficiently large to reliably determine average correction rates and to evaluate the influence of varus deformity as an independent predictor of correction velocity and treatment success.
When considering a normal ‘healthy’ physis versus a ‘sick’ one, 10 a differential correction rate can be expected. We report that an important determinant of the correction rate is the underlying aetiology. Lowest correction rates for tibial growth modulation were observed for skeletal dysplasia patients and metabolic conditions, and highest correct rates for longitudinal reduction defect patients and patients with rickets as underlying disorder. For the latter, the underlying pathological process is usually simultaneously treated with medical management, contributing to a relatively fast rate of correction of deformity. 21 For femoral growth modulations lowest correction rates were observed for skeletal dysplasia patients and highest rates also for rickets patients.
Previous studies have reported a faster correction rate in the idiopathic group compared to mixed pathologic groups 22 Our study stratified cases more distinctly and found that certain disorders, mainly those related to short stature, corrected more slowly. However, aetiologies that do not directly affect growth or the physis, such as the idiopathic and complex group, corrected faster. Surprisingly, acquired growth disturbances did not fare poorly in the current cohort, with correction rates slightly higher than those in idiopathic cases. This is consistent with previous reports, which have shown that in combination with a physeal bar resection, tension-band hemiepiphysiodesis is a viable option for correcting angular deformities. 23 It should be noted that this statement holds true only for cases in which hemiepiphysiodesis was attempted. For cases in which too large a part of the physis was affected, hemiepiphysiodesis was unlikely to have been attempted, leading to a selection bias in this cohort. Therefore, the relatively good correction rate in infection and posttraumatic cases at least partly reflects careful patient selection for this procedure and should not be extrapolated to all acquired angular deformities. Overall, our results support that hemiepiphysiodesis should be considered a viable treatment option for a range of aetiologies even when the physis is (partly) affected.
We also identified independent predictors for CR and treatment success. Higher age at surgery for both femoral and tibial corrections and varus deformity for femoral corrections are independent predictors for lower CR. Higher age at surgery, varus deformity and more severe initial deformity were independently predictive for failure to achieve a neutral mechanical axis with guided growth.
The finding that higher age is related to both slower angular correction and undercorrection might be related to the gradual slowing of growth velocity as the child approaches skeletal maturity. As correction relies on longitudinal growth, insufficient residual growth potential leads to increased chance of incomplete correction. Age, and skeletal age in particular, must be considered when planning growth modulations.24,25 Guided growth may initially prevent deformity progression, but then takes time to facilitate deformity correction. The same holds true for etiologies that affect longitudinal growth, such as MPS-IV (Morquio-A) classified under the metabolic disorders. 26 In all cases, the hemi-epiphysiodesis should be timed such that sufficient longitudinal growth remains to allow for desired angular correction to take place.
The lower correction rate observed in varus deformities in our cohort merits specific consideration. A substantial proportion of the varus cases in our series were associated with underlying pathologies such as Blount disease, skeletal dysplasia and metabolic bone disease, all of which are characterized by abnormal physeal architecture and altered loading conditions. These factors are likely to make growth modulation less efficient and less predictable than in idiopathic valgus deformities. Similar patterns have been reported previously: in a large multinational guided-growth study, Danino et al. 1 identified direction of deformity as an independent determinant of outcome, with femoral varus deformity exerting a negative effect on the amount of correction compared with valgus alignment. Likewise, Yilmaz et al. 27 found that in children with skeletal dysplasia treated with hemiepiphysiodesis, valgus deformities corrected more reliably than varus deformities, with correction achieved in 89% of valgus deformities versus 58% of varus cases. In our multivariable regression, we adjusted for underlying aetiology, and varus deformity still emerged as an independent negative predictor of correction rate and treatment success. This suggests that, beyond the effect of diagnosis, the direction of deformity itself may play a role in the responsiveness to guided growth. Clinically, these findings imply that expectations regarding correction should be more cautious in varus deformities, and that earlier intervention, close follow-up and a lower threshold for alternative or adjunctive procedures may be warranted in this subgroup.
We report that a neutral mechanical axis was achieved 68.7% of patients treated with guided growth. Considering the relatively high percentage of incomplete corrections over all aetiology groups and the strong relationship of age at surgery with incomplete correction, it seems advisable to time the procedure earlier rather than later particularly when growth charts confirm early cessation of growth or lack of an adolescent growth spell, for example, in achondroplasia or the mucopolysaccharoidoses. This must be balanced with the higher risk of recurrence when performing the procedure at a younger age. 28 Nevertheless, timing of the procedure in the current series seems to be on the conservative side, leading to a relatively high proportion of incomplete corrected limbs.
More severe deformities were predictive of not achieving full correction, despite not being related to a lower correction rate. An explanation for this might be, that in general it is advised to leave tension band plates no longer than 2 years in situ, to avoid the risk of induced a permanent growth arrest.29,30 This was, at least in a small subgroup of the patients the reason to remove the plate before complete correction. After a rest period the deformity was then corrected further using guided growth, this is in line with previous reports that serial guided growth session are a feasible option. We did however not leave the plate in situ with only the epiphyseal screw attached, as a so-called ‘sleeper plate’. This is justified by recent reports that such a strategy poses more risk (e.g. formation of a bony bar or ongoing physeal tethering) than benefits.31,32
Caution should be taken when applying guided growth in younger children. Frequent follow-up is advisable, as our study has shown a faster correction rate especially and higher risk of overcorrection with lower age at the time of tension band plate implantation. Likewise, less frequent follow-up may be appropriate for those with short stature, more severe initial deformity and older age, this would reduce the number of clinic appointments and/or radiographic exposure. Follow-up should be tailored according to these parameters, using the mean correction rates for each aetiology provided by this study.
With all aetiologies, recurrent deformity is relatively common with a young age at the onset of treatment and a large initial deformity described as the main risk factors.33–35 Although, patients with underlying etiologies such as mucopolysaccharidosis (MPS) have been described to be at high risk of recurrence rebound does not occur in all at risk patients, 35 therefore, we recommend against routine overcorrection. 36 Unfortunately, based on this dataset, alignment change after tension band plate removal can not be evaluated. Therefore, defining the extent of rebound that can be expected in individual cases after guided growth procedure remains an important topic for future research.
Guided growth has been described as an adjunct to acute corrections, for example, to prevent recurrence in infantile Blount’s disease. 37 Because we analyzed the correction rate at segment level, these cases could not be included in the analysis, but as the number of cases where this was performed was limited in our series, we do not feel this has significantly affected our results. On the other hand, for these cases, the same principles are likely hold true; the growth potential of the physes and influence or underlying aetiology inform how much and how fast correction can be expected.
This study has several limitations that should be acknowledged. First, the retrospective design meant that data availability and completeness were dependent on existing clinical records, and data on rebound after implant removal were not available. This limitation could be addressed in future studies through prospective multicenter registries with standardized follow-up protocols extending at least 2 years post-implant removal to systematically capture rebound phenomena and long-term alignment stability. Second, patients were included from multiple centres, which may have introduced variation in indications for surgery, surgical techniques and follow-up protocols. On the other hand, this multicenter approach increases the generalizability and real-world applicability of our findings across different clinical settings and patient populations. Establishing consensus guidelines for treatment indications and standardized surgical protocols across centres would enhance comparability in future multicenter studies while preserving this external validity. Third, information on body weight and body height as well as growth speed velocity at time of treatment was lacking. These factors are potential predictors of correction speed and treatment success and should be considered as parameters in future research.
Conclusion
Hemi-epiphysiodesis with tension band plates is an effective method of deformity correction in children with a wide spectrum of underlying diagnoses and severity of deformity. Nevertheless, there are significant differences in correction rate between etiologies and incomplete correction is not uncommon. This should be taken in to account in planning and follow-up of guided growth. Especially children closer to skeletal maturity and/or with underlying skeletal dysplasia or metabolic disorders are at risk for slower and incomplete correction and therefore correction should be started early.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251411732 – Supplemental material for Guided growth for the correction of angular lower limb deformity: Correction rates for idiopathic and non-idiopathic aetiologies
Supplemental material, sj-pdf-1-cho-10.1177_18632521251411732 for Guided growth for the correction of angular lower limb deformity: Correction rates for idiopathic and non-idiopathic aetiologies by Jaap J Tolk, Lea M Keßling, Andrea Yeo, Sara Gargent, Menaz Menazirsha, Benu Wickremasinghe and Deborah M Eastwood in Journal of Children's Orthopaedics
Footnotes
Author contributions
Conceptualization DME; methodology JJT, AY, DME; formal analysis JJT, LMK; investigation JJT, LMK, AY, SG, MM, BW, DME; writing – original draft JJT, LMK, AY writing – review and editing JJT, LMK, AY, SG, DME; visualization JJT, LMK, AY supervision DME.
Data availability statement
All data generated or analyzed during this study are available from the corresponding author upon reasonable request. The datasets are not publicly available due to privacy restrictions and ethical approval restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical board approval
For this study ethical board approval was obtained at the Royal National Orthopaedic Hospital, Stanmore, United Kingdom (reg. no. SE21.03) and at Erasmus Medical Centre, Rotterdam, The Netherlands (MEC-2023-0673, non-WMO committee). We obtained a waiver of consent from the medical ethics committee at the Erasmus MC. This waiver was granted due to the nature of this study (medical records review only) and the burden of informed consent for (parents of) children with extensive medical needs.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.