
Abstract
Objective:
To prospectively evaluate with magnetic resonance imaging (MRI), the relationship between the distance from the incision of the drain output location and postoperative spinal epidural hematoma (SEH) in patients performed with microendoscopic decompressive laminotomy (MEDL) for lumbar spinal stenosis.
Methods:
Between January 2016 and June 2018, three different kinds of drain placement techniques, according to the drain output location, were performed to a total of 184 patients after MEDL for single-level spinal stenosis. The location of the drain output was within the incision in group 1, 1 cm lateral of the incision in group 2, and 5 cm lateral of the incision in group 3. At 24 h postoperatively, before removal of the drain, MRI examination was carried out in patients. A specific classification was developed by the authors to measure SEH, and the groups were evaluated by comparison.
Results:
The mean postoperative dural sac cross-sectional area was 1.73 cm2 (standard deviation (SD): 0.711) in group 1, 1.66 cm2 (SD: 0.732) in group 2, and 1.52 cm2 in group 3 (SD: 0.841).The mean cross-sectional area of the postoperative hematoma was 1.45 cm2 (SD: 1.007) in group 1, 1.57 cm2 (SD: 1.053) in group 2, and 2.11 cm2 (SD: 1.024) in group 3. Four grades were defined according to the specific classification. According to this classification, grades C and D postoperative hematomas were determined at a statistically significantly higher rate in group 3 patients (drain output 5 cm lateral from the incision) compared to the other groups (p = 0.000). No significant difference was determined between groups 1 and 2 in respect of hematoma classification.
Conclusion:
In conclusion, it was determined that better drainage was provided in groups 1 and 2, where the drain output location was in the incision or close to it.
Keywords
Introduction
Postoperative spinal epidural hematomas (SEH) have been reported at extremely high rates (33–67.6%) in the literature. 1 –3 Compared with conventional laminotomy, SEH is seen more in microendoscopic decompressive laminotomy (MEDL) due to the limited area and small incision from where there could be bleeding. 4 The development of SEH in a patient delays the recovery of preoperative symptoms, and, sometimes, a second operation is required to drain the hematoma.
Prevention of SEH plays a very important role in obtaining intraoperative bleeding control. However, it may sometimes be difficult to control bleeding coming from the epidural deep venous plexus. Even in patients where very good bleeding control has been obtained, hypertension may occur when waking or later, and there may then be bleeding again. 4,5 Therefore, the use of a drain postoperatively is vital. However, the high rates of SEH seen despite the use of a drain raise the question of whether the drain is working effectively.
In hydrodynamic physics, the loss of fluid from within a pipe, when the direction of the pipe is changed, is known as “exit loss.” Exit loss is related in direct proportion to the angle of the pipe and in inverse proportion to the radius of the section which is bent. 6
Generally, surgeons have a tendency to place the drain after MEDL far from the incision to prevent the infection. From the starting point of the above-mentioned theory, the hypothesis of this study was that the output location of the drain placed after the MEDL procedure could affect the size of hematoma that could form.
Methods
This prospective study included patients with single-level spinal stenosis treated between January 2016 and June 2018. Patients were excluded if they had intraoperative dural tears, revision surgery, and coagulopathy or if the drain tip was not in the sublaminar area when checked on magnetic resonance imaging (MRI) and computed tomography (CT) at 24 h postoperatively. All patients were randomly selected and operated on by the corresponding author. The same medical treatment was applied postoperatively and the same drain type was used in all patients (Jackson-Pratt Silicone Round Drain, Cardinal Health, Waukegan, IL, USA). The patients were divided into three groups as group 1 (direct), group 2 (+1 cm), and group 3 (+5 cm) according to the distance between the incision site and drain output (Figure 1).

Pictures from three groups. Drain output is located (a) inside of incision in group 1, (b) 1 cm lateral from incision in group 2, and (c) 5 cm lateral from incision in group 3.
In MEDL technique, patients are placed in the prone position under general anesthesia. Bilateral decompression is performed with a METRx system microendoscope (Medtronic Sofamor Damek, Memphis, TN, USA) using a unilateral laminotomy. During surgery, hemostasis is achieved by bipolar electrocoagulation or hemostatic agents. The surgery is performed with the patient under hypotensive anesthesia with systolic blood pressure kept <90 mmHg. Before wound closure, the hemostatic agents were removed, the blood pressure is returned to normotension, bleeding control is checked again, and a drain is placed.
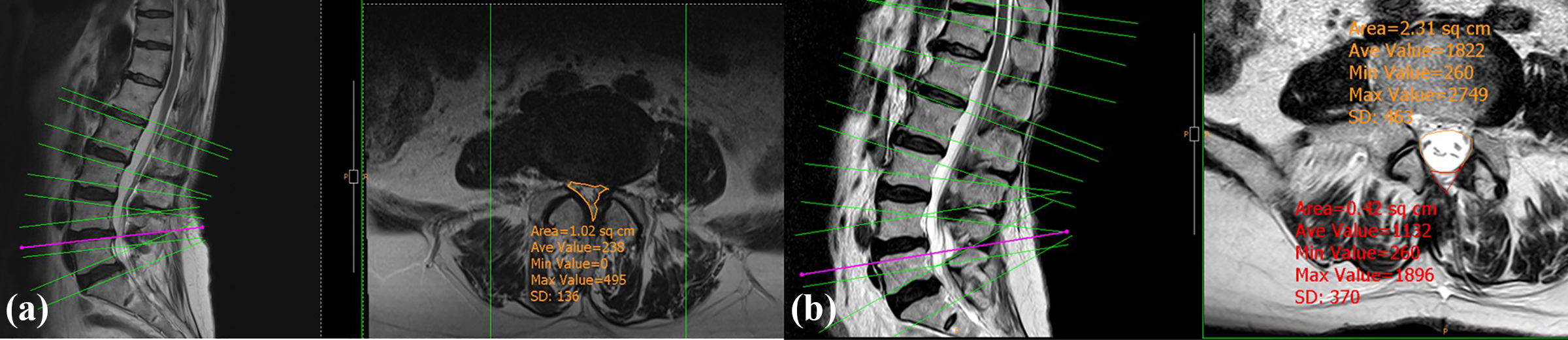
MRI and CT examinations were applied to the patients at 24 h postoperatively. Hematomas were divided into categories using a hematoma classification specifically designed by the authors of this study. According to this classification, the cross-sectional area of the preoperative dural sac (Pre DS), the cross-sectional area of the postoperative DS (Po DS), and the hematoma cross-sectional area under the line drawn from the spinous process to the ventral surface of the facet joint on the laminotomy side were measured (Figure 2). The measurements were taken using a DICOM viewer on the POP-net webserver (Image ONE Co., Tokyo, Japan) by two spinal surgeons determining the cross-sectional area on the line passing through the middle of the disc level with spinal stenosis. According to this classification: Grade A: Po DS has a round shape. There could be a small hematoma but not compressing the DS. Grade B: Po DS is not round in shape because of a small hematoma, but Po DS area > Pre DS area > hematoma area. Grade C: Moderate hematoma; hematoma area > Po DS area > Pre DS area. Grade D: Severe hematoma; hematoma area >Pre DS area> Po DS area.

Illustration of the new classification system of SEH. Grade A: Po DS has a round shape. There could be a small hematoma but not compressing the DS. Grade B: Po DS is not round in shape because of a small hematoma, but Po DS area > Pre DS area > hematoma area. Grade C: moderate hematoma; hematoma area > Po DS area > Pre DS area. Grade D: severe hematoma; hematoma area > Pre DS area > Po DS area.
The data obtained from the patient groups after hematoma classification were processed and transferred to the SPSS statistics program (SPSS for Windows 21.0 SPSS Inc., 2016, Armonk, NY, USA). For statistical analyses, the χ 2, one-way analysis of variance, and Kruskal–Wallis tests were used to compare the groups. The Wilcoxon signed-rank test was applied in the comparisons of pre- and postoperative DS size. The Tamhane T2 test was used for post hoc analysis. A value of p < 0.05 was accepted as statistically significant.
The written informed consent was obtained from the patients, and the study was performed in accordance with the Declaration of Helsinki and approved by the ethics committee of Ankara University School of Medicine.
Results
Evaluation was made of 184 patients, comprising 94 (51%) males and 90 (49%) females with a median age of 71.61 years (range: 48–91 years). Other patient characteristics are shown in Table 1. No significant difference was determined between the groups in respect of age, gender, operation level, and amount of drainage within the first 24 h and postoperative DS area.
Patients characteristics and results.

Pre DS: preoperative dural sac; Po DS: postoperative dural sac.
The Pre DS size was significantly smaller in group 2 (+1 cm; mean: 0.706 cm2, standard deviation (SD): 0.329) than in group 1 (direct; mean: 0.844 cm2, SD: 0.285) and group 3 (+5 cm; mean: 0.916 cm2, SD: 0,298; p = 0.012; Figures 3 and 4). Grades C and D hematomas were observed at a statistically significantly higher rate in group 3 (+5 cm; p = 0.000; Table 2). The hematoma size was significantly larger in group 3 (+5 cm; mean: 2.11 cm2, SD: 1.024) than in the other two groups (p = 0.000), and no significant difference was determined between group 1 (mean: 1.45 cm2, SD: 1.007) and group 2 (mean: 1.57 cm2, SD: 1.053; p = 0.706; Figure 5). The change between pre- and postoperative DS size was lower in group 3 (+5 cm) than in the other groups (p = 0.01), and there was no significant difference in this respect between groups 1 and 2 (p = 0.918; Figure 6).

Grade A hematoma in a patient in group 1 (direct): (a) preoperative MRI and (b) postoperative MRI. MRI: magnetic resonance imaging.
Grade A hematoma in a patient in group 2 (+1 cm): (a) preoperative MRI and (b) postoperative MRI. MRI: magnetic resonance imaging.
The distribution of the groups according to classification.


Grade D hematoma in a patient in group 3 (+5 cm): (a) preoperative MRI and (b) postoperative MRI, postoperative DS area was narrower than preoperative MRI. The drain tract was twisted. MRI: magnetic resonance imaging.

The distribution of the groups according the hematoma classification. Grades C and D hematomas were observed at a statistically significantly higher rate in group 3 (+5 cm; p = 0.000).
Discussion
SEH is a frequently seen event and MRI applied in the early stage is extremely useful in determination. 1,7,8 In several studies, SEH has been generally defined as symptomatic or asymptomatic. 5,9 –12 Symptomatic is defined as severe pain in the incision site or extremities or neurological worsening within hours. 9 In this study, patients were not evaluated clinically, but the aim was to investigate the relationship between the efficacy of the drain placed postoperatively and the distance from the incision. Therefore, with the development of a new classification system using MRI, it was aimed to determine the rates and dimensions of hematoma development in each group.
SEH incidence has been reported in the literature at varying rates (33–67.6%), 1 –3 and, in the current study, this rate was 100%. The point that can be stressed here is that it can be considered almost impossible not to have the formation of any blood collection following a surgical intervention. In the current study on patients with grade A hematoma on the postoperative MRI, hematoma was determined even if it was of a very small size. As the MEDL technique is a minimally invasive technique and the area created for surgery is small, it is possible for even a low-volume hematoma to become symptomatic.
There have been several studies in the literature related to the prevention of SEH and the determination of the risks. However, no consensus has yet been reached on the definition of all the risk factors. In a retrospective study by Awad et al., age >60 years, Rh+ blood group, intraoperative hemoglobin value <10 g/dl, and international normalized ratio (INR) > 2.0 within 48 h postoperatively were found to significantly increase the risk of SEH. 13 Kou et al. reported that multilevel procedures and preoperative coagulopathy increased SEH risk significantly. 14 In a prospective study of symptomatic patients by Sokolowski et al., there was reported to be a relationship between advanced age, multilevel procedures, INR, and large volume hematomas. 3
To the best of our knowledge, few studies have been conducted related to drains after spinal surgery. Nakamura et al. reported that significantly fewer hematomas were observed in patients with urokinase-treated antithrombogenic drain placement compared to those with standard drains. It was also stated that the drain may not always have been appropriately placed. 4 In the current study, the drain placement site was confirmed on MRI and CT applied postoperatively, and cases with incorrect placement were withdrawn from the study. The same type of drain was used in all the patients of this study. Ahn et al. compared 1.6- and 2.8-mm diameter drains and found no difference. 15 In another experimental study, also by Ahn et al., it was reported that a delay in drain placement and the intraoperative use of antihemorrhagic preparates increased hypercoagulopathy and caused obstruction in the drain. 16 As this delay could be valid in multilevel procedures, only patients applied with single-level spinal stenosis surgery were included in the current study and there was no delay in drain placement in any patient. Further homogeneity of the groups was obtained by all the operations being performed by the same surgeon.
Exit loss is calculated in physics with the formula as Δh = kV 2 /2g, 6 where Δh = exit loss, k = coefficient, V = mean velocity of the flow within the pipe, and g = gravity. The k coefficient increases in direct proportion to the angle of the pipe and in inverse proportion to the radius of the section which is bent (k = [0.13 + 1.85−[d/2r]3.5] ⊖/180) 6 (Figure 7). In addition, when the angle (⊖) increases in flexible pipes, such as a drain, the radius (r) of the section that is bent decreases. The k coefficients corresponding to some angle values are shown in Table 3. According to this, when the angle made in the pipe increases, the fluid drained decreases. For the output of the drain placed in the sublaminar area in the group 3 (+5 cm) patients, it was noted that in most patients, turns of approximately 70° had been made. This could explain the advanced grade of hematomas seen in this group compared to the other two groups (Figure 8).

Parameters with “exit loss” effect in obtuse angles: d, diameter of the flat section; r, radius of the bent section; ⊖, angle of the directional change.
Relationships between the coefficient (k), angle (⊖), radius in the bent area (r), and diameter of the flat section (d).a
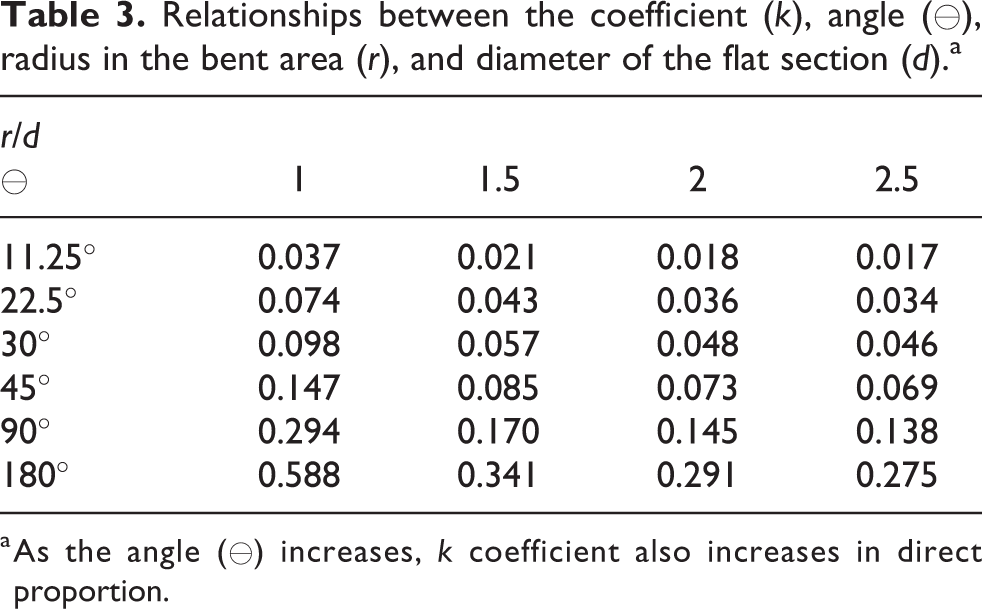
a As the angle (⊖) increases, k coefficient also increases in direct proportion.

CT scan of a patient performed 5-cm lateral drain output location. Arrows show the angled pipe about 70°. CT: computed tomography.
In a study by Kanayama et al. of patients performed with single-level lumbar decompression or discectomy, no difference was reported between patients with and without a drain in respect of hematoma and infection. 17 In the current study, despite the placement of a drain, grade A hematoma was determined in 65 patients, and in all the patients determined with grade B, hematoma was determined, even if small in size. When it is considered that the mean output of the drains was measured as 49.02 cc in the first 24 h, there is a strong possibility that if the drain had not been placed, a larger SEH would have been observed with the contribution of the drained amount. In patients where spinal decompression is not made, in other words, when the thecal sac is not exposed, restricting and halting the bleeding of the surrounding tissues with a tampon effect can be considered. However, in patients performed with spinal decompression, a direct tampon effect on the thecal sac is a serious risk. Therefore, the use of a drain is recommended for patients performed with decompression surgery.
A limitation of this study is that hematoma may expand throughout the craniocaudal axis; therefore, the cross-sectional measurements of hematoma may be meaningless. However, in the literature, hematoma size has usually been measured using cross-sectional area. 1,9,11,15 As a matter of fact, we did not find any hematoma extending in the longitudinal plan in our study. This can be considered as MEDL technique is a minimally invasive technique, in other words, the soft tissue remains largely intact along the long axis in this technique. Therefore the hematoma cannot find a cavity that can spread along the long axis.
Conclusion
In conclusion, the use of a drain is necessary after spinal decompression surgery and locating the drain output within or close to the incision without any angulation can be considered an effective method to protect against the development of SEH.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.