
Abstract
Objective:
The traditional percutaneous vertebroplasty (PVP) could induce massive radiation and side injuries to the tissues around the fractured centrum. This study was designed to reduce the radiation and damage and improve the treatment efficiency of PVP.
Methods:
Forty four patients who diagnosed to be acute osteoporotic single vertebral compression fractures were collected and randomly divided into traditional group and improved group, and these two groups were separately treated by the traditional and improved PVP which assisted by the preoperative digital design. The treatment outcome between these two groups was compared and analyzed by Students’ t test and χ 2 test.
Results:
Compared with the traditional PVP, the improved PVP could significantly reduce the X-ray fluoroscopy times for determining puncture point (14.41 ± 4.00 vs. 6.82 ± 2.15, p < 0.001) and puncture route (22.73 ± 3.89 vs. 13.36 ± 3.39, p < 0.001), the X-ray fluoroscopy times during the operation (76.59 ± 12.4 vs. 34.82 ± 6.74, p < 0.001), operation duration (28.64 ± 7.43 min vs. 15.23 ± 4.4 min, p < 0.001), and total radiological dose (588.85 ± 53.86 cGycm2 vs. 276.5 ± 58.17 cGycm2, p < 0.001). The improved PVP could also significantly decrease the visual analog score at intra-operation (7.68 ± 0.78 vs. 4.50 ± 0.67, p < 0.001) and 1 day after the operation (2.45 ± 0.51 vs. 2.16 ± 0.36, p < 0.05). Besides, the improved PVP could not significantly affect the Oswestry disability index after operation (p > 0.05).
Conclusion:
The improved PVP operation could significantly reduce the total radiological dose and X-ray fluoroscopy times, protect the patients and medical staff, and reduce the pain caused by the operation.
Trial registration:
This trial was registered in China clinical trial registration center and the registration number was ChiCTR-INR-17011557.
Keywords
Introduction
As China was gradually stepping into the aging society, the amount of patient who was diagnosed to be acute osteoporotic single vertebral compression fractures (AOVCF) had also increased in past decades. 1 –3 Recently, the percutaneous vertebroplasty (PVP) had become more and more mature in clinical application because of its fast development and wide application. 4 –6 Even though the PVP had shown its advantages in the clinical treatment on AOVCF, there were still many shortages that should be overcome. 7 During the operation, the C-arm fluoroscopy was inevitable to be frequently used to determine the puncture point, puncture route, and the operation process. 8,9 As the patients and medical personnel might be harmed by the X-ray from the C-arm fluoroscopy as it could lead to the functional degradation, distortion, and carcinogen for the thyroid, gonad, and gland. 10,11
In traditional PVP operation, the puncture point and route need to be determined and adjusted frequently by X-ray fluoroscopy and this could further lead to the increase of radiation exposure. 12,13 Besides, the adjustment of the puncture point and route would damage the issue around, and this would lead to the discomfort and pain to the patients, and it could further negatively affect the pain relief. 13 Hence, it was necessary to take measures to guide the puncture in PVP operation to avoid the extra adjustment. 14 Recently, the guiding technology and instrument had been widely researched to improve the PVP operation which was mainly based on computed tomography scaning. 15,16 Based on the guiding technology and instrument, it could effectively reduce radiation exposure, shorten operation time, and increase the success rate for AOVCF. 14
From the 1980s, the digital information technology had been gradually applied in medical science and clinical treatment. 17,18 Based on the digital information technology, the spine had been analyzed through constructing the three dimensional (3-D) model. 19 Hence, in this study, the PVP operation was improved by the preoperative digital design for constructing the 3-D model of the fractured centrum, educing the exposure times caused by adjusting the puncture route, reducing the damage and discomfort, and improving the treatment efficiency.
Subjects and methods
Patients
After approved by the ethic institution, 44 patients were collected from Beijing Shijitan Hospital between June 2017 and January 2018 (10 males, 34 females; age range: 57–91; mean age: 76.3 ± 9.8). All of these patients were diagnosed to be AOVCF, and among them, the fractures for 2 cases occurred at T10 (4.5%), 3 cases at T11 (6.8%), 15 cases at T12 (34.1%), 13 cases at L1 (29.5%), 5 cases at L2 (11.4%), 3 cases at L3 (6.8%), and 3 cases at L4 (6.8%). These patients were randomly divided into two groups which were the traditional group and improved group. The patients in the traditional group were treated by traditional PVP operation, and the patients in the improved group were treated by improved PVP operation.
The inclusion criteria of patients in this study were as follows: (1) patients who were diagnosed with AOVCF; (2) the preoperative imaging data were complete (X-ray, magnetic resonance imaging (MRI), computed tomography (CT), and 3-D reconstruction
Besides, to make certain specific fracture part of vertebral body and perform the operation more accurately, CT scan and 3-D reconstruction were applied to all enrolled patients. Final, the diagnostic standard for the single vertebral compression fracture was the MRI image data.
Preoperational modeling and detection
Two masks, which were named to be 1 and 2, were constructed based on the DICOM format data collected by Mimics 19.0 through CT scanning, and the Hu value was set to be 180–2000 to let the centrum clearly shown. Fractured centrum in mask 1 was erased and isolated, and the target centrum (mask 3) was extracted by subtracting the mask 2 by mask 1 by Boolean operation (Figure 1). After the 3-D model was constructed (Figure 2), the operation process was simulated to let the puncture needle at the optimal position (Figure 3). Then, corresponding data was collected including inserting depth, abduction angle, and rake angle of the puncture needle (Figure 4). The distance between two electrodes which were closest to the designed inserting position at the skin was measured and recorded. All of the patients collected had provided written informed consent before joining in this study.

Process of constructing 3-D model of the fractured centrum. (a) Side image of the erased centrum in mask 1; (b) cross-section image of the erased centrum in mask 1; (c) side image of the mask 3; and (d) cross-section image of the mask 3. 3-D: three dimensional.

The 3-D model of the fractured centrum. 3-D: three dimensional.

The simulated optimal puncture position. (a) and (b) Simulated optimal puncture position in 3-D model. (c) and (d) Simulated optimal puncture position in CT image. 3-D: three dimensional; CT: computed tomography.

Measurement about the rake angle between different punctures and the design of the puncture point at skin. (a) and (b) Measurement about the rake angle between different punctures. (c) and (d) Design of the puncture point at skin.
Operation methods
The improved PVP operation was carried out at the following steps. After the physical examination was performed to the patients in the improved group, the patients lied on the sickbed in the prone position. Then, the location of the fractured centrum was estimated on the body’s surface. Three metal location topograms (material: stainless steel, diameter: 10 mm; hollow) were prepared, and a topogram was placed at the junction of posterior midline at the back skin and the horizontal line of the body surface projection of the fractured centrum. Then, the other two topograms were placed at the location 3 cm above and below the first topogram, respectively. The skin under the hollow was blacked, and the topograms were all fixed by a transparent film and covered by surgical dressing until the operation (3M Company, Maplewood, Minnesota, USA). After it, the fractured centrum and adjacent centrums were diagnosed by CT thin thickness scan (thickness <2 mm), and before the CT scanning, the gradienter was placed above the edge of the surgical dressing to record the values about the long horizontal axes (Figure 5). Then, the 3-D model was constructed after the CT data was read into the Mimics 19.0 using the method above mentioned. When the operation began, the patients kept the prone position at electric operation bed which was the same as the position in the CT scan by letting the data recorded by the gradienter the same through adjusting the electric operation bed (Figure 6). After it, the puncture point was determined according to the 3-D modeling and fine-tuning based on X-ray, and the puncture point was the intersection point between the two arcs whose centers were the two electrodes closest to the designed inserting position at pre-operation (Figure 7). After the regular local anesthesia, the puncture though trans arch of the vertebra was performed with the assist of ruler and protractor (Figure 8), and it was as shown in Figure 9. Besides, the following operation steps were the same as the traditional PVP operation.
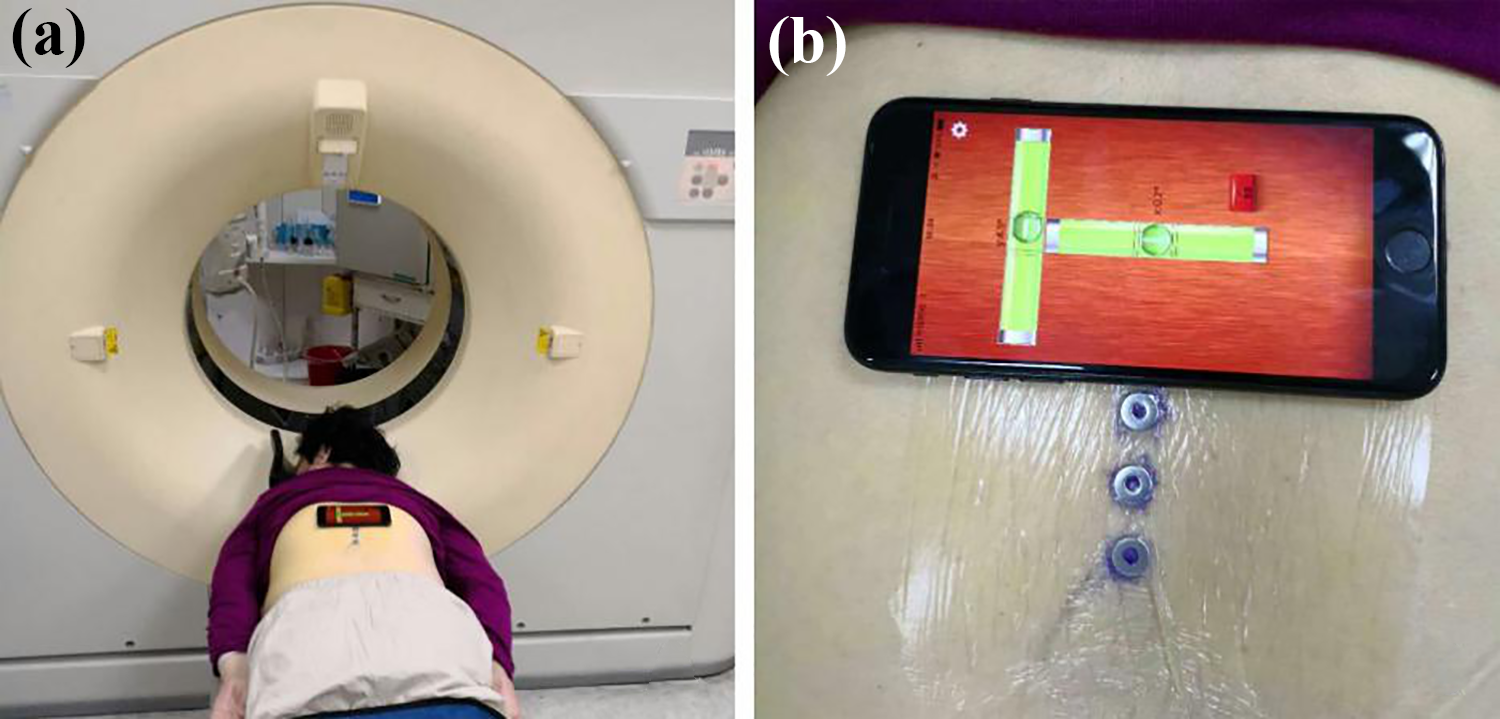
CT scan for the fractured centrum. (a) The prone position in CT scan and (b) measurement for the values about the long horizontal axes. CT: computed tomography.

Recovery of the prone position at electric operation bed.

Determination of the puncture site.

Puncture though trans arch of the vertebra with the assist of ruler and protractor.
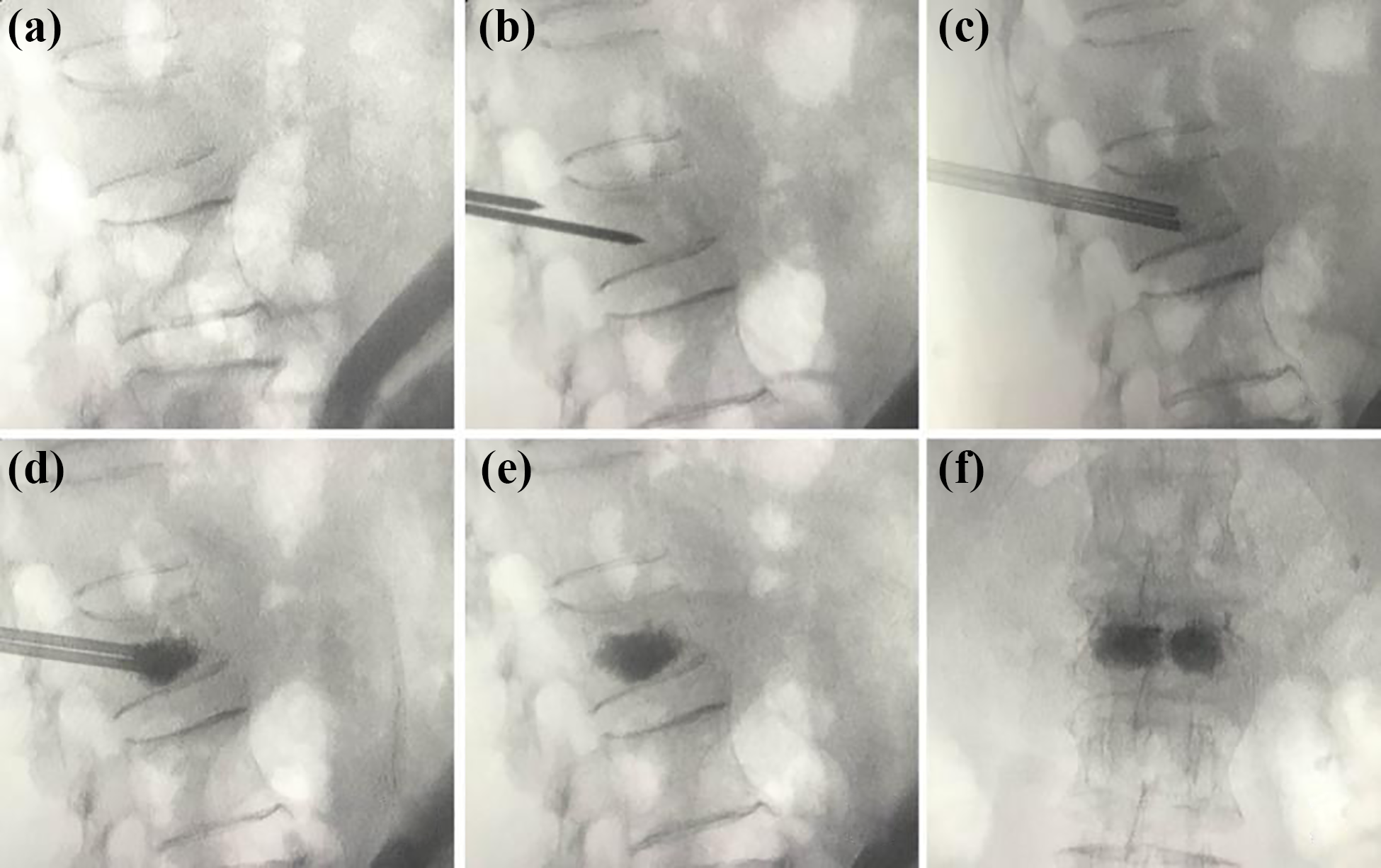
The performance of puncture under the X-ray fluoroscopy.
Key measurements
The key measurements include the following aspects: the number of X-ray for determining puncture point, number of X-ray for determining puncture route into trans arch of vertebra, total number of X-ray during operation, operation duration, total radiological dose, intra-operation visual analog score (VAS), VAS at 1 day after operation, VAS before discharge after operation, VAS at 3 months after operation, VAS at 6 months after operation, VAS at 1 year after operation, Oswestry disability index (ODI) at 1 month after operation, ODI at 3 months after operation, ODI at 6 months after operation, and ODI at 1 year after operation. The VAS and ODI were assessed by the Chinese version of the corresponding standard questionnaires.
Statistical analysis
In this study, the data were analyzed by IBM SPSS 23.0 (SPSS Inc., Chicago, Illinois, USA). The measurement data were analyzed by the Student’s t test and performed at the format of mean ± SD (
Results
Baseline characteristics
The baseline characteristics for the patients were statistically analyzed as presented in Tables 1 and 2. There was no significance for all of the variables between the patients in the traditional group and improved group in aspects of age, lumbar bone mineral density (BMD), lumbar T score, formal neck BMD, femoral neck T score, femoral neck total BMD, femoral neck total T score, pre-operation VAS, pre-operation ODI, gender, and fractured centrum (p < 0.05).
Baseline characteristics of the measurement data the study sample.

BMD: bone mineral density; VAS: visual analog score; ODI: Oswestry disability index.
Baseline characteristics of the count data the study sample.

Clinical treatment
The clinical treatment was compared and analyzed for the traditional group and improved group as presented in Table 3. Compared with the traditional PVP operation, the improved PVP operation could significantly reduce the number of X-ray for determining puncture point (traditional: 14.41 ± 4.00, improved: 6.82 ± 2.15, p < 0.001), determining puncture route (traditional: 22.73±3.89, improved: 13.36 ± 3.39, p < 0.001), and the total number of X-ray during operation (traditional: 76.59 ± 12.4, improved: 34.82 ± 6.74, p < 0.001). Besides, the improved PVP operation could significantly reduce the operation duration (traditional: 28.64 ± 7.43 min, improved: 15.23 ± 4.4 min, p < 0.001). The total radiological dose was also significantly reduced in the improved group (traditional: 588.85 ± 53.86 cGycm2, improved: 276.5 ± 58.17 cGycm2, p < 0.001). For the score of VAS intra-operation and postoperation, the improved PVP operation could significantly reduce the VAS at intra-operation (traditional: 7.68 ± 0.78, improved: 4.50 ± 0.67, p < 0.001) and 1 day after the operation (traditional: 2.45 ± 0.51, improved: 2.16 ± 0.36, p < 0.05), while there was no significant difference for the VAS before discharge after operation, and the VAS at 3 months, 6 months, and 1 year after operation (p > 0.05). In the end, the improved PVP operation could not significantly decrease the ODI for the patients at 1 month, 3 months, 6 months, and 1 year after operation between the traditional group and the improved group (p > 0.05). In the end, no complication was observed after operation in both the traditional group and improved group.
Compared analysis of the clinical treatment in different groups.
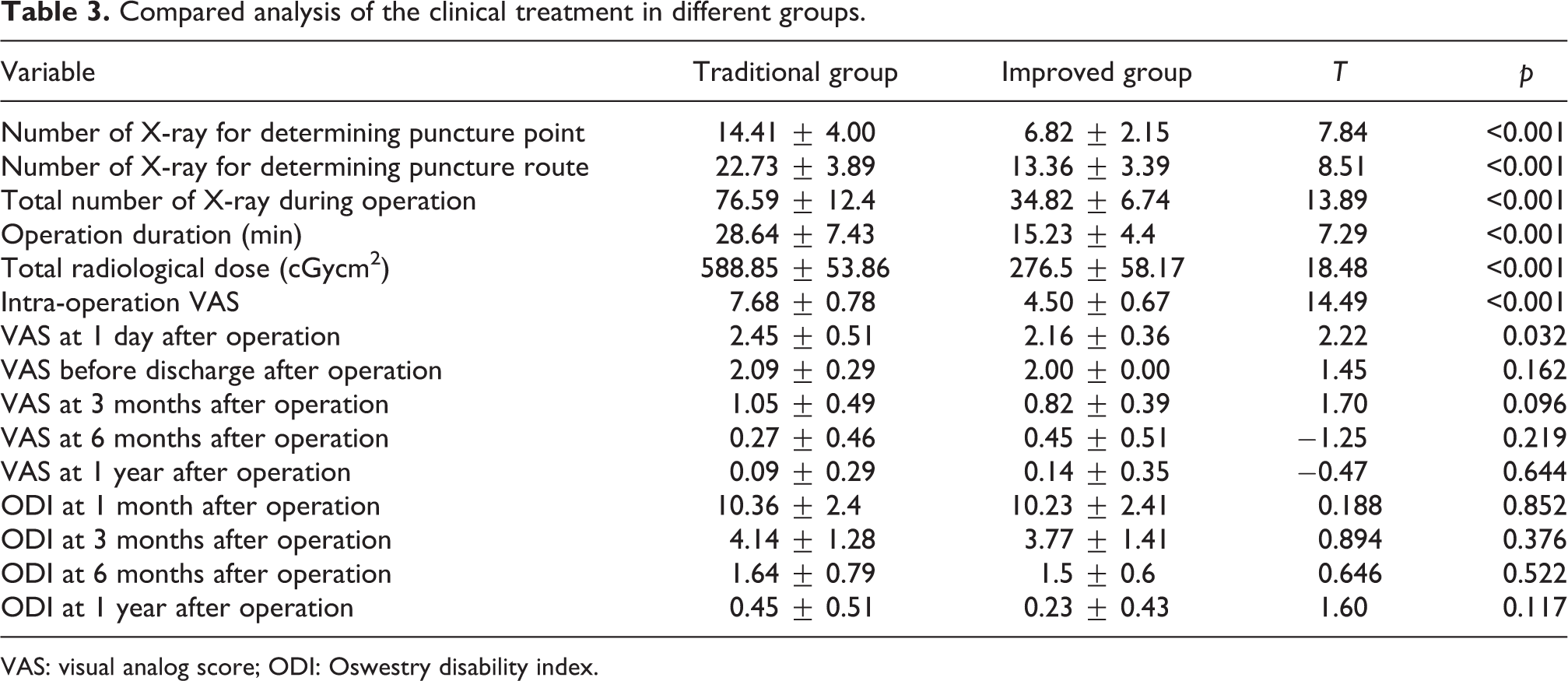
VAS: visual analog score; ODI: Oswestry disability index.
Discussion
Through this study, it mainly found that the improved PVP operation which assisted by the preoperative digital design could significantly improve the treatment outcome for the patients who were diagnosed to be the AOVCF.
At first, CT scan and 3-D reconstruction were very important for this study on account of the modeling. Relevant research had showed that the radiation dose of CT scan was too low to harm the patients, in other words, it could be ignored. Besides, the CT scan could clearly show the specific fracture part of vertebral body, especially the endplate and the wall, then, the preoperative design would be more accurate, thus the accuracy of the operation was improved as well.
The number of X-rays was decreased by improved PVP operation. This improvement might be the reason that the optimal puncture route and puncture point had been simulated based on the 3-D model of the fractured centrum, and the optimal puncture point and puncture route could be determined faster, besides, it could further reduce the number of X-ray for the determining puncture point, puncture route, and the total number of X-ray during operation. These findings were consistent with the report of Zhai et al. who reported that the application positioning guidance instrument which based on the CT scanning could reduce the X-ray fluoroscopy times. 16 In this study, the preoperative digital design was also a kind of positioning guidance technique for the percutaneous pedicle puncture. For the operation process, the assistance of the preoperative digital design could also significantly reduce operation duration and the total radiological dose. Under the guidance of the simulated optimal puncture point and route, the time used for the finding the puncture point and route could significantly reduce and the radiological dose could also be significantly reduced as the X-ray fluoroscopy times had been significantly reduced. These findings were similar to the report by Long et al., as their self-designed 3-D guiding instrument could significantly reduce the operation duration and the X-ray fluoroscopy times. 15
For the treatment outcome for the improved PVP operation which assisted by the preoperative digital design, the improved PVP operation could significantly reduce the VAS during operation and at 1 day after operation, and it could not significantly reduce the ODI at 1 month, 3 months, 6 months, and 1 year after operation. These findings reflect that compared with the traditional PVP operation, the improved PVP operation could reduce the pain caused by the operation, while it could not improve the health status faster. This improvement of the pain might be the result of the faster and accurate puncture speed improved by the preoperative digital design, and it could further reduce the damage caused to the tissue around the fractured centrum. Besides, as the improved PVP operation could not improve the surgery processed on the fractured centrum, it could not affect the recovery of the fractured centrum.
According to the research in this study, the improved PVP operation had the following advantages. At first, its operation process was simple as it could find the optimal puncture route and point by the ruler, compass, and the protractor. At second, as the sample operation process, the doctors could acquire the operation fast. Besides, as the fewer puncture times and effect on the tissue around the fractured centrum, the improved PVP operation could significantly reduce the total radiological dose and the X-ray fluoroscopy times and reduce the pain and discomfort to the patients. While this study had the following limitations. First, there were just 44 patients collected in this study, and this may not reflect the overall improvement of the improved PVP operation for the AOVCF. In the future study, the amount of the patients should be enlarged to fully analyze the treatment improvement for the improved PVP operation. Second, the patients collected were just from the same hospital which located in Beijing. It was necessary to analyze the treatment efficiency of the improved PVP operation in different hospitals and different areas.
Conclusion
The improved PVP operation assisted by the preoperative digital design could significantly reduce the radiation exposure and the pain for the patients who were diagnosed to be the AOVCF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by “YangFan” plan of Beijing Hospital Authority (grant no. XMLX201713).