
Abstract
Study Design:
Systematic review and meta-analysis.
Objective:
Percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) are minimally invasive techniques widely used for the treatment of neurologically intact osteoporotic Kümmell’s disease (KD), but which treatment is preferable remains controversial. Therefore, this study aimed to shed light on this issue.
Methods:
Six databases were searched for all relevant studies based on the PRISMA guidelines. Two investigators independently conducted a quality assessment, extracted the data and performed all statistical analyses.
Results:
Eight studies encompassing 438 neurologically intact osteoporotic KD patients met the inclusion criteria. Compared to PVP, PKP was associated with greater improvement in the short- and long-term Cobb angle [SMD = −0.37, P = 0.007; SMD = −0.34, P = 0.012], short-term anterior vertebral height [SMD = 0.43, P = 0.003] and long-term middle vertebral height [SMD = 0.57, P = 0.012] and a lower cement leakage rate [SMD = 0.50, P = 0.003] but produced more consumption (cement injection volume, operative time, fluoroscopy times, intraoperative blood loss and operation cost). However, there were no differences between the 2 procedures in the short- and long-term VAS and ODI scores, long-term anterior vertebral height, overall complications or new vertebral fractures.
Conclusions:
Both procedures are equally effective for neurologically intact KD in terms of the clinical outcomes, with the exception of a lower cement leakage risk and better radiographic improvement for PKP but greater resource consumption. Based on the evidence available, good clinical judgment should be exercised in the selection of patients for these procedures.
Introduction
Kümmell’s disease (KD) is defined as delayed posttraumatic vertebral collapse secondary to pathological vertebral compression fractures and is characterized by vertebral microtrauma with an asymptomatic period, followed by aggravated pain recurrence and progressive kyphosis deformity months or years later, which predominantly affects older individuals with osteoporosis.1-3 The lesions are usually located in the thoracolumbar region and affect a single-level vertebra in the majority of cases.4,5 KD has rarely been reported in previous studies and can easily be misdiagnosed as a pathological fracture. With advanced imaging technology and additional medical knowledge, more KD cases are being detected, and the prevalence of KD ranges from 7% to 37% among people with osteoporotic vertebral fractures. 6 Currently, KD is diagnosed mainly on the basis of a combination of clinical symptoms and imaging characteristics. The intravertebral vacuum cleft phenomenon on plain radiography has been deemed a representative imaging sign of vertebral avascular osteonecrosis, the most widely accepted pathophysiology of KD.7,8 In addition, intravertebral gas-like, fluid-like, or mixed signals detected by MRI scans can be used to predict osteonecrosis derived from vertebral microfractures, with high sensitivity (86%) and specificity (100%). 9 Even so, the definite pathogenesis, natural history and diagnostic criteria of KD remain controversial.
Due to the rarity and complexity of KD, no consensus has been reached regarding a management protocol or a single definitive treatment for KD. 10 Considering that the affected vertebra develops insidiously and fails to heal spontaneously, traditional conservative treatments (e.g., analgesics and bed rest) are usually ineffective and may even contribute to delayed neurological damage.11,12 In terms of surgical treatments, different procedures have been adopted according to the development phase of KD. For patients with neurological deficits, open surgeries (anterior, posterior, or combined anterior and posterior approaches) are routinely recommended to decompress the spinal canal, restore spinal alignment and conserve spinal stability.13,14 For neurologically intact KD, minimally invasive techniques are feasible choices and have the advantages of fast deformity correction, pain relief and functional recovery. 15 Percutaneous kyphoplasty (PKP) and percutaneous vertebroplasty (PVP) have been widely accepted by surgeons and patients and possess several advantages over open surgeries, including smaller wounds, lower costs, earlier mobilization and faster rehabilitation. 16
Generally, it is believed that PVP is more economical than PKP because there are no additional consumables, such as balloons.17,18 The evidence available has confirmed that PVP is a safe and effective surgical procedure for KD.1,5,19 PKP is more conducive to restoring vertebral height and correcting kyphosis and is considered a better choice for patients with significant vertebral height loss (HL) and old fractures with pseudarthrosis.20-22 However, because bone cement is injected into the compressed vertebral body under a large pressure, PKP and PVP may cause associated complications, with bone cement leakage being the most common complication.16,23 It is generally acknowledged that the incidence of cement leakage in PKP is lower than that in PVP when OVCFs are treated.17,24-28 A previous systematic review of 69 clinical studies demonstrated that the cement leakage rate was 9% in PKP and 41% in PVP. 24 Subsequently, Zhan et al 28 conducted a meta-analysis with 2872 OVCF patients (4187 vertebrae) and reached a similar conclusion: the incidence rates of cement leakage for PVP and PKP were 18.4% and 54.7%, respectively. Moreover, cement leakage in PKP and PVP was observed in 13.6% and 37.9% of patients with cancer-related vertebral compression fractures. 29 Currently, an increasing number of studies have specifically reported the leakage rates of PVP and PKP for the treatment of KD. However, these studies were limited by a small sample size such that some of the results were conflicting rather than conclusive. For instance, Kong et al 30 concluded that the cement leakage rate in the PVP group (66.7%) was significantly higher than that in the PKP group (20.7%), whereas Chang et al 31 found that there were no significant differences between the 2 procedures (10.7% vs. 17.9%, P > 0.05). Bone cement leakage can not only lead to severe neurological complications such as paraplegia and root compression through the spinal canal or the intervertebral foramina 32 but also cause pulmonary or intracardiac embolism and even death through the pulmonary artery.33,34 Therefore, it is of vital importance to determine which method has the highest effectiveness and leads to the fewest complications for neurologically intact KD.
Reportedly, both procedures have been proposed for the treatment of KD without neurologic impairment and have demonstrated high clinical satisfaction, but high-quality studies directly comparing PVP and PKP in terms of clinical efficacy and safety are so scant that the preferable choice for neurologically intact KD remains controversial. To the best of our knowledge, there are no meta-analyses that have provided reliable evidence on this issue. Therefore, we collected the best available evidence and performed a meta-analysis to systematically evaluate the clinical outcomes, imaging improvements, perioperative complications and intraoperative resource consumption associated with PVP and PKP for the treatment of neurologically intact osteoporotic KD, which provided evidence-based guidance for clinical practice.
Materials and Methods
Search Strategy
The meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 35 PubMed, Cochrane Library, EMBASE, Web of Science, CNKI and Wanfang Data was searched for relevant studies without language restrictions from their inception dates to September 1, 2020. The following search terms were used in all searches: (i) kummell [Title/Abstract]) OR avascular osteonecrosis of vertebral body [Title/Abstract]) OR vertebral osteonecrosis [Title/Abstract]) OR vertebral pseudarthrosis [Title/Abstract]) OR intravertebral vacuum cleft [Title/Abstract]) OR delayed vertebral collapse [Title/Abstract]); AND (ii) kyphoplasty [Title/Abstract]) OR vertebroplasty [Title/Abstract] OR PVP [Title/Abstract]) OR PKP [Title/Abstract]). Moreover, the reference lists of eligible studies were searched for additional papers that had not been identified by the primary search strategy. All titles, abstracts, and full texts were screened independently by 2 reviewers. Disagreements were resolved by arriving at a consensus through comparing notes.
Inclusion Criteria
The inclusion criteria were as follows: (1) the study population included adult patients definitively diagnosed with stage I and II Kümmell’s disease; (2) the interventions included PVP and PKP; (3) at least one of the following outcome indicators were included: functional evaluation (Oswestry Disability Index (ODI), visual analog scale (VAS) score), imaging evaluation (Cobb angle, anterior vertebral height, middle vertebral height), complications (bone cement leakage, new vertebral fracture) and consumption (injection volume of bone cement, fluoroscopy times, intraoperative blood loss, operation time); and (4) the study design was a randomized controlled trial (RCT) or comparative observational study.
Exclusion Criteria
The exclusion criteria were as follows: (1) single-armed follow-up studies; (2) reviews, case reports, letters and comments; (3) studies that used cadaveric specimens or animal models; and (4) studies presenting incomplete or inappropriate data. If duplicate data or data from the same population was used in more than one study, the most recent or complete study was included in the analysis.
Quality Assessment
The Cochrane risk of bias tool was used to evaluate the methodological quality of the RCTs in terms of selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias. The study was classified as having a high, an unclear, or a low risk of bias for each domain. The Newcastle-Ottawa Quality Assessment Scale (NOQAS) was used to assess the methodological quality of nonrandomized comparative studies with 3 main items and a total score of 9 points: selection (0–4 points), comparability (0–2 points), and the measurement of exposure factors (0–3 points). Studies with more than 6 points were considered high quality. The quality assessment was conducted independently by 2 reviewers. Any disagreements were resolved by reaching a consensus.
Data Abstraction
Data from all included studies was extracted and put into a standard form independently by 2 investigators, and disagreements were resolved by discussion. The following essential information was abstracted: (1) study characteristics, including the author, publication year, country, and study design; (2) patients’ demographic and clinical information, including the population source, age, sex, surgical procedures, number of participants, and mean follow-up duration; and (3) outcome indicators, including the ODI and VAS scores, Cobb angle, anterior and middle vertebral height, and bone cement leakage. In addition to routine measurement, the anterior and middle vertebral body heights were measured and expressed as Ha (%) and Hm (%); A and M were divided by the mean value of the corresponding cortical heights of the 2 nearest nonfractured vertebrae, respectively (Figure 1).
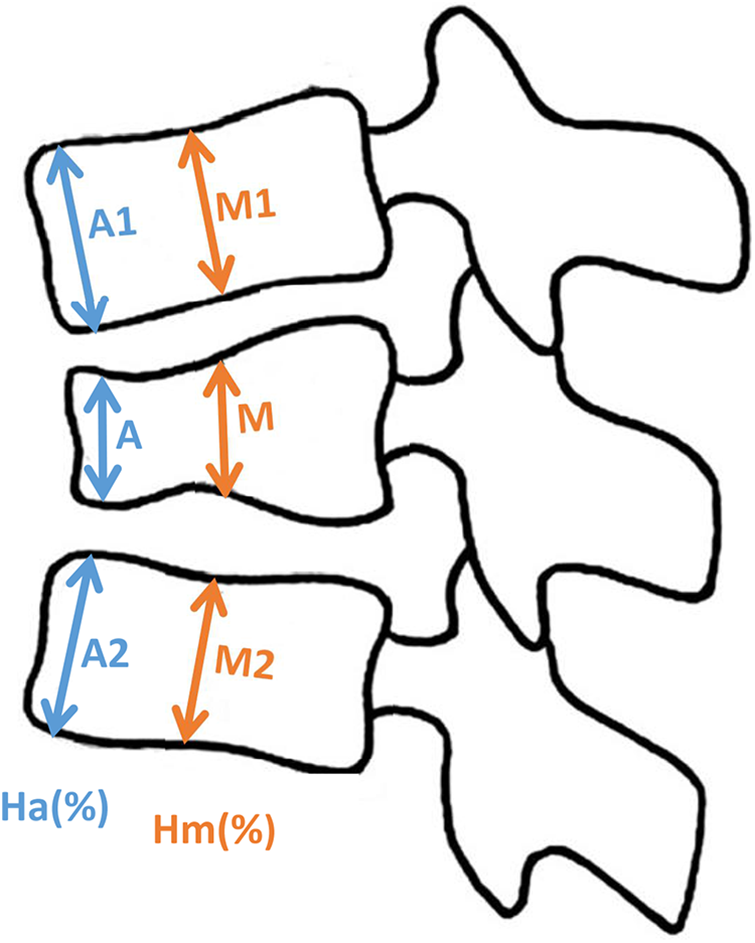
Measurement of the vertebral heights of the anterior and middle vertebral bodies. A (measured vertebral height of the anterior column), M (measured vertebral height of the middle column), estimated vertebral height of the anterior column = (A1+A2)/2, estimated vertebral height of the middle column = (M1+M2)/2), Ha(%) = A/estimated vertebral height of the anterior column, Hm(%) = M/estimated vertebral height of the middle column.
Statistical Analysis
All meta-analyses were conducted by Stata software 14.0. For the continuous outcomes such as the ODI and VAS scores, the mean difference (MD) or standard mean difference (SMD) and 95% confidence interval (CI) were used for estimates. For dichotomous outcomes such as the rate of complications, odds ratios (ORs) and 95% CIs were calculated. Statistical significance was identified by p values < 0.05. The level of statistical heterogeneity was assessed by the I-square test. I-square values of 25%, 50%, and 75% indicated low, moderate, and high heterogeneity, respectively. When I 2 < 50%, a fixed-effect model was applied, and when I 2 > 50%, a random-effect model was applied. If significant heterogeneity existed, subgroup analysis and sensitivity analysis was used to find the source of heterogeneity. All quantitative analysis results were demonstrated using forest plots. Publication bias was statistically assessed using the visual inspection of the funnel plot.
Results
Included Studies
A total of 1072 papers were preliminarily retrieved from searches of the various electronic databases. First, 524 articles remained after the duplicates were removed with Endnote software. Then, we read the titles and abstracts and rejected 505 irrelevant studies. Based on the inclusion and exclusion criteria, 19 studies were excluded after the full texts were read. Finally, 8 eligible articles30,31,36-41 were included in this meta-analysis. The flow chart of the literature search process is shown in Figure 2.
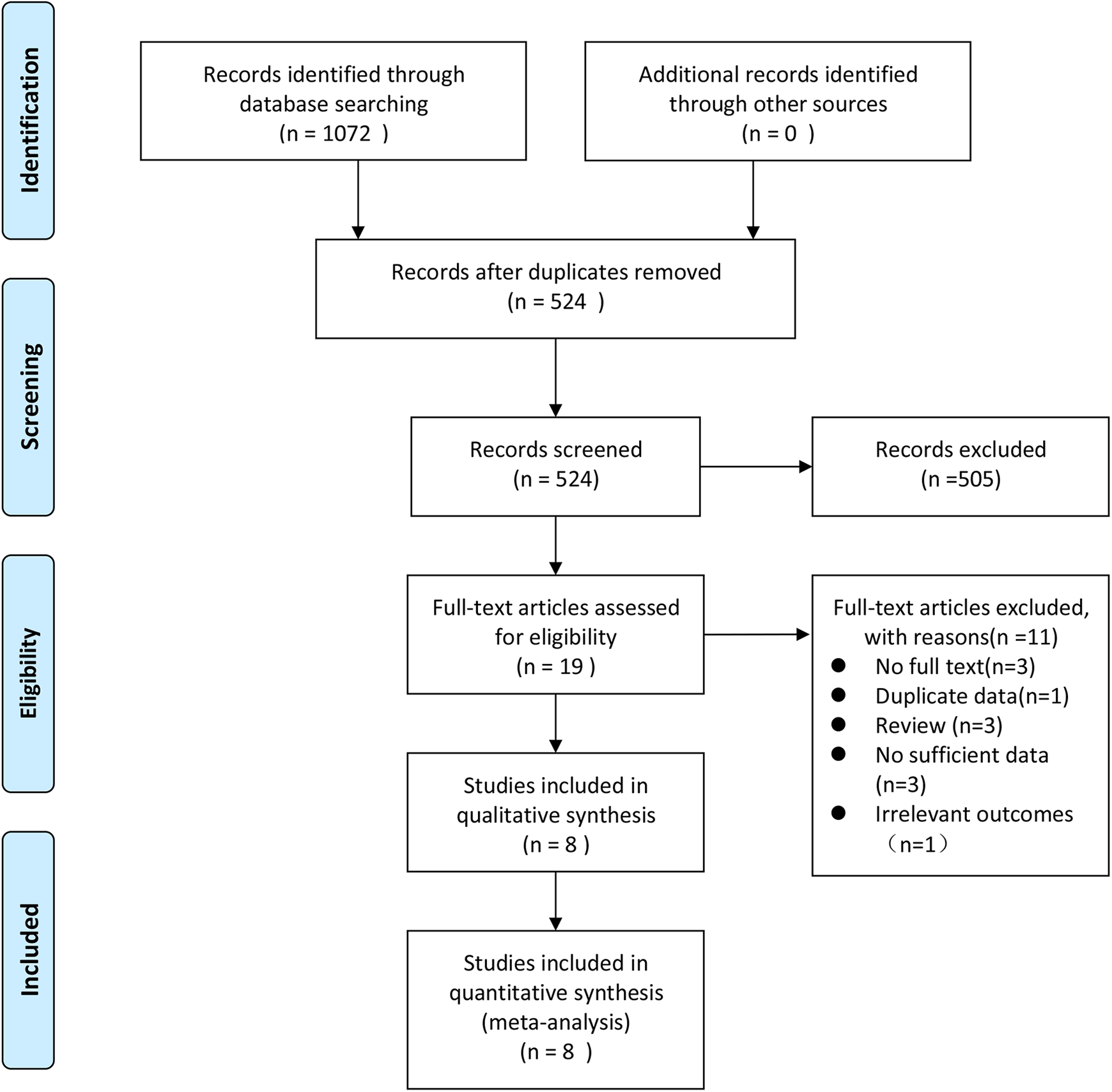
Flow diagram of the study identification and selection process.
Study Characteristics
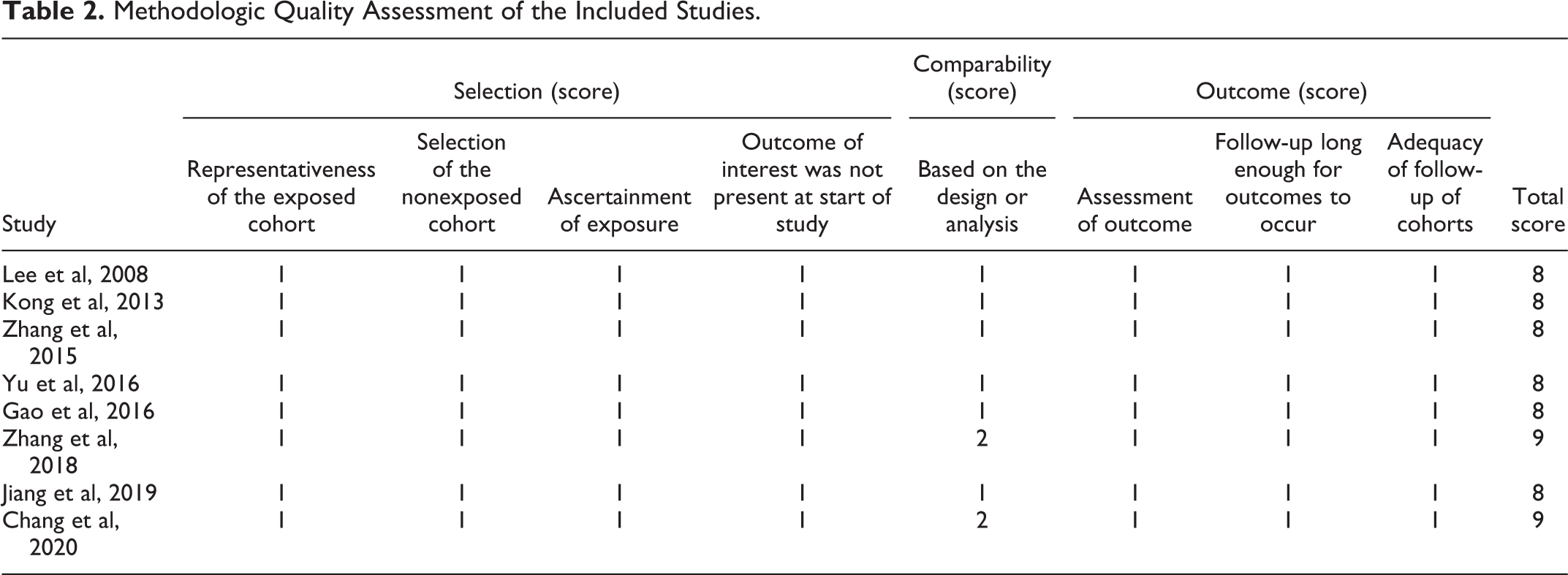
The included studies involved a total of 438 KD patients, 195 of whom were treated with PKP and 243 of whom were treated with PVP. All studies were nonrandomized observational studies, and there were 2 prospective and 5 retrospective case-control studies. Four studies30,31,37,40 were in English, three38,39,41 were in Chinese, and one 36 was in Korean. The publication years of these studies ranged from 2008 to 2020. The basic characteristics of the patients in the included studies, such as age and sex, were comparable. The minimum duration of follow-up across all studies was 12 months. The study features and patients’ demographic and clinical data are listed in Table 1. According to the NOQAS for nonrandomized studies, 2 studies31,40 scored 9 points, and 6 studies30, 36–39, 41 scored 8 points (Table 2). Therefore, methodologically, all included studies were considered of high quality.
The Demographic Characteristics of the Included Studies.
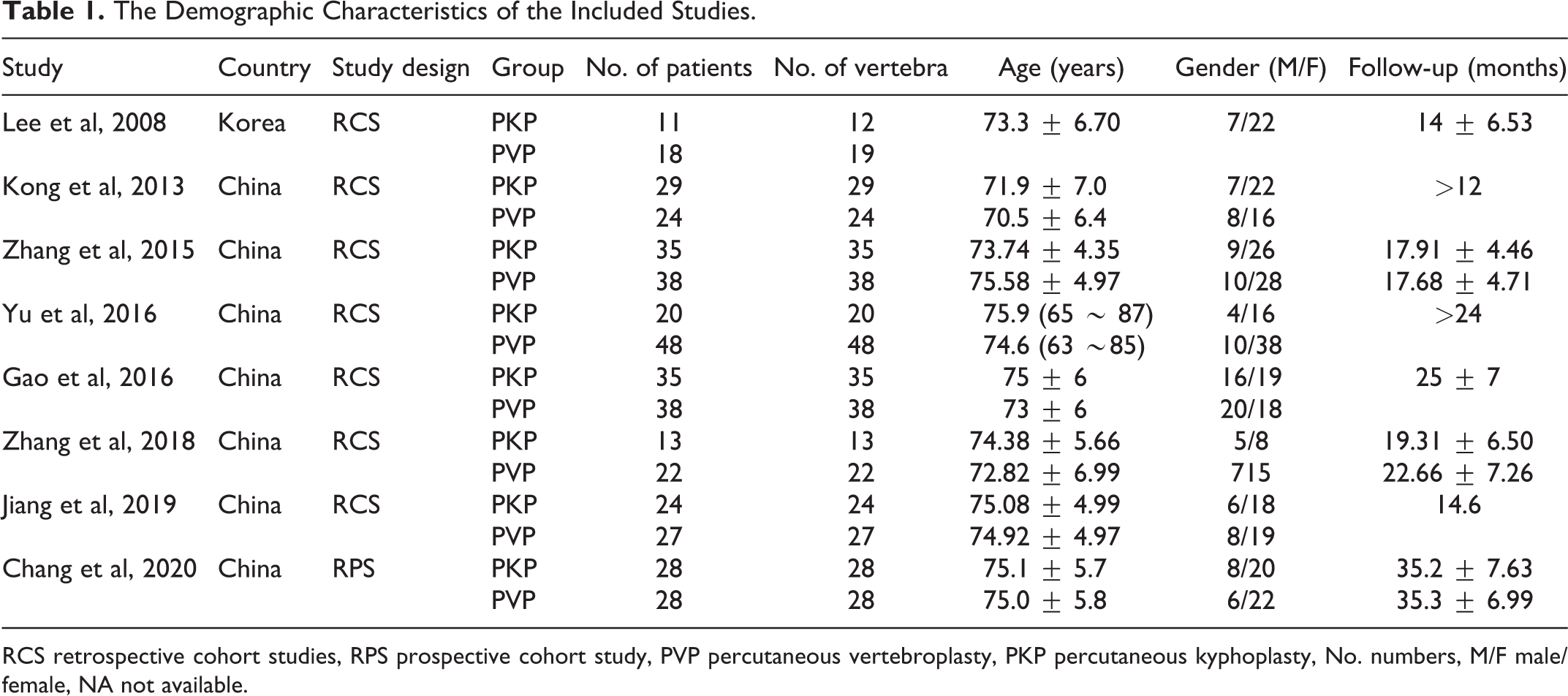
RCS retrospective cohort studies, RPS prospective cohort study, PVP percutaneous vertebroplasty, PKP percutaneous kyphoplasty, No. numbers, M/F male/female, NA not available.
Methodologic Quality Assessment of the Included Studies.
Meta-Analysis
Clinical Outcomes (ODI and VAS Scores)
The clinical outcomes, including the ODI and VAS scores, at different time points (before the operation, after the operation and at the final follow-up), were combined. All studies provided the VAS scores for the 195 patients undergoing PKP and 243 patients undergoing PVP. There were no differences between the PKP group and PVP group in the preoperative [SMD = −0.14, 95% CI (−0.33, 0.05), P = 0.158], postoperative [SMD = 0.03, 95% CI (−0.16, 0.22), P = 0.779] or last follow-up VAS score [SMD = −0.06, 95% CI (−0.25, 0.13), P = 0.531], which showed low heterogeneity (I 2 < 50%) (Figure 3).
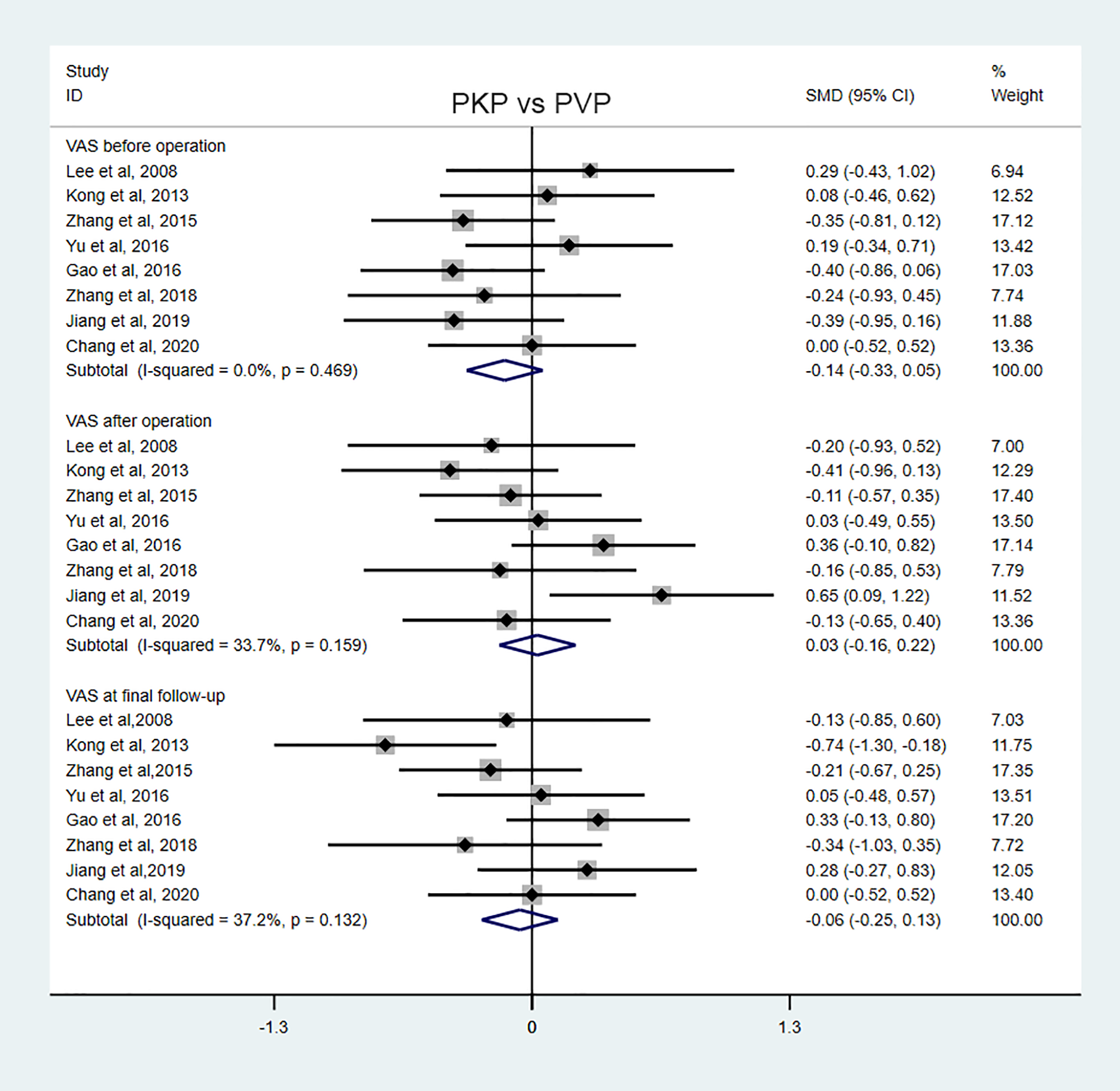
Forest plot of 2 studies estimating the short-term and long-term VAS scores.
A total of 6 studies including 149 patients in the PKP group and 187 patients in the PVP group reported the ODI score. Pooled analysis with low heterogeneity (I 2 < 50%) showed no significant differences between the 2 groups in the preoperative [SMD = −0.10, 95% CI (−0.32, 0.12), P = 0.358], postoperative [SMD = −0.20, 95% CI (−0.43, 0.04), P = 0.099] or last follow-up ODI score [SMD = −0.14, 95% CI (−0.36, 0.08), P = 0.208] (Figure 4).
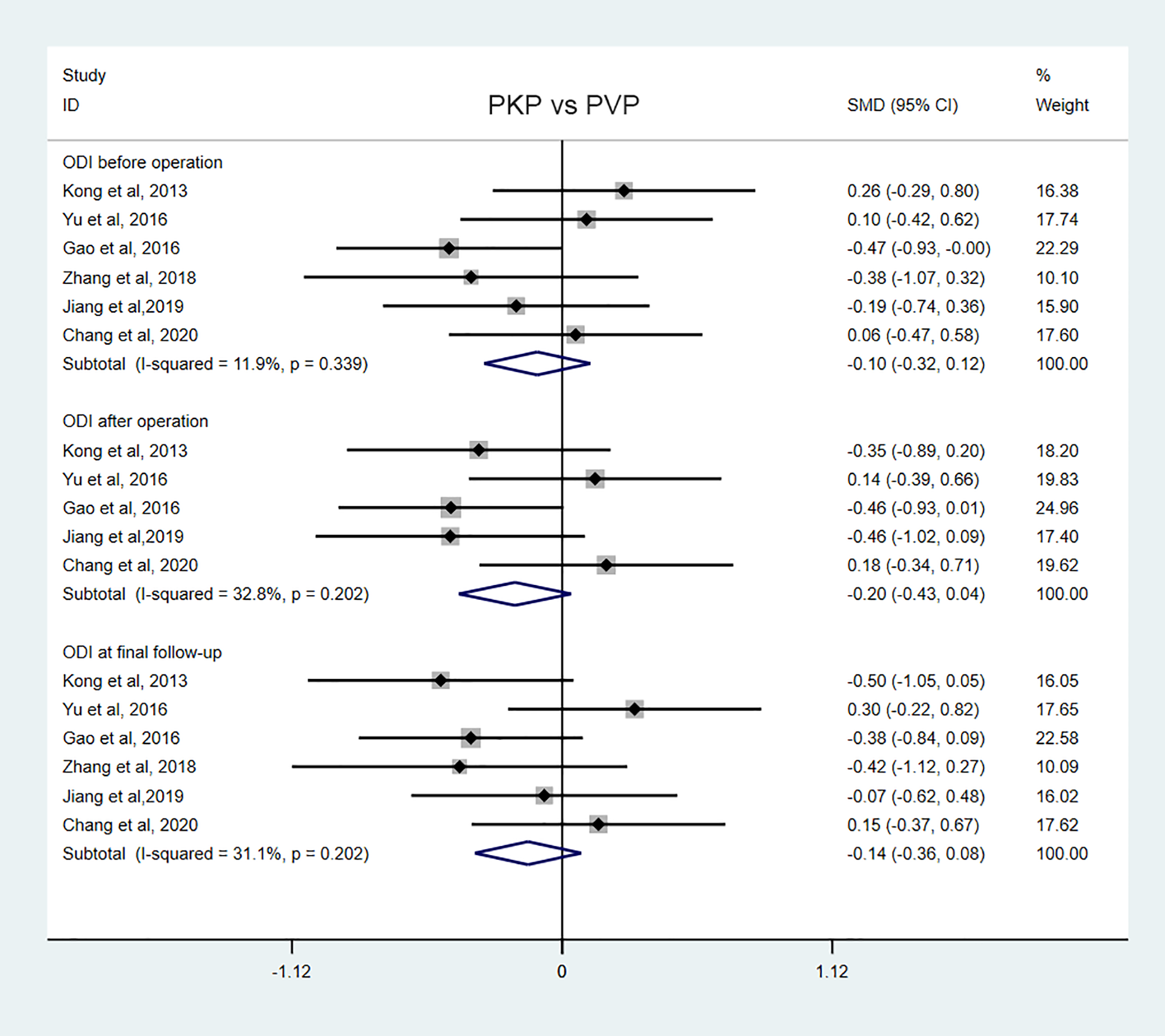
Forest plot of 2 studies estimating the short-term and long-term ODI scores.
Radiographic Outcomes (Cobb Angle and Anterior Vertebral Height)
The radiographic outcomes included the Cobb angle and vertebral body height (anterior vertebral height, Ha and Hm). Five studies with 98 patients undergoing PKP and 140 undergoing PVP reported the Cobb angle. A fixed-effect model was applied due to the low heterogeneity (I 2 < 50%). There were no differences between the 2 groups in the Cobb angle before the operation, but the Cobb angle after the operation [SMD = −0.37, 95% CI (−0.64, −0.10), P = 0.007] and at the final follow-up [SMD = −0.34, 95% CI (−0.61, −0.07), P = 0.012] in the PKP group were significantly lower than those in the PVP group, which demonstrated that PKP corrects kyphosis deformities to a greater extent in the short term and long term (Figure 5).
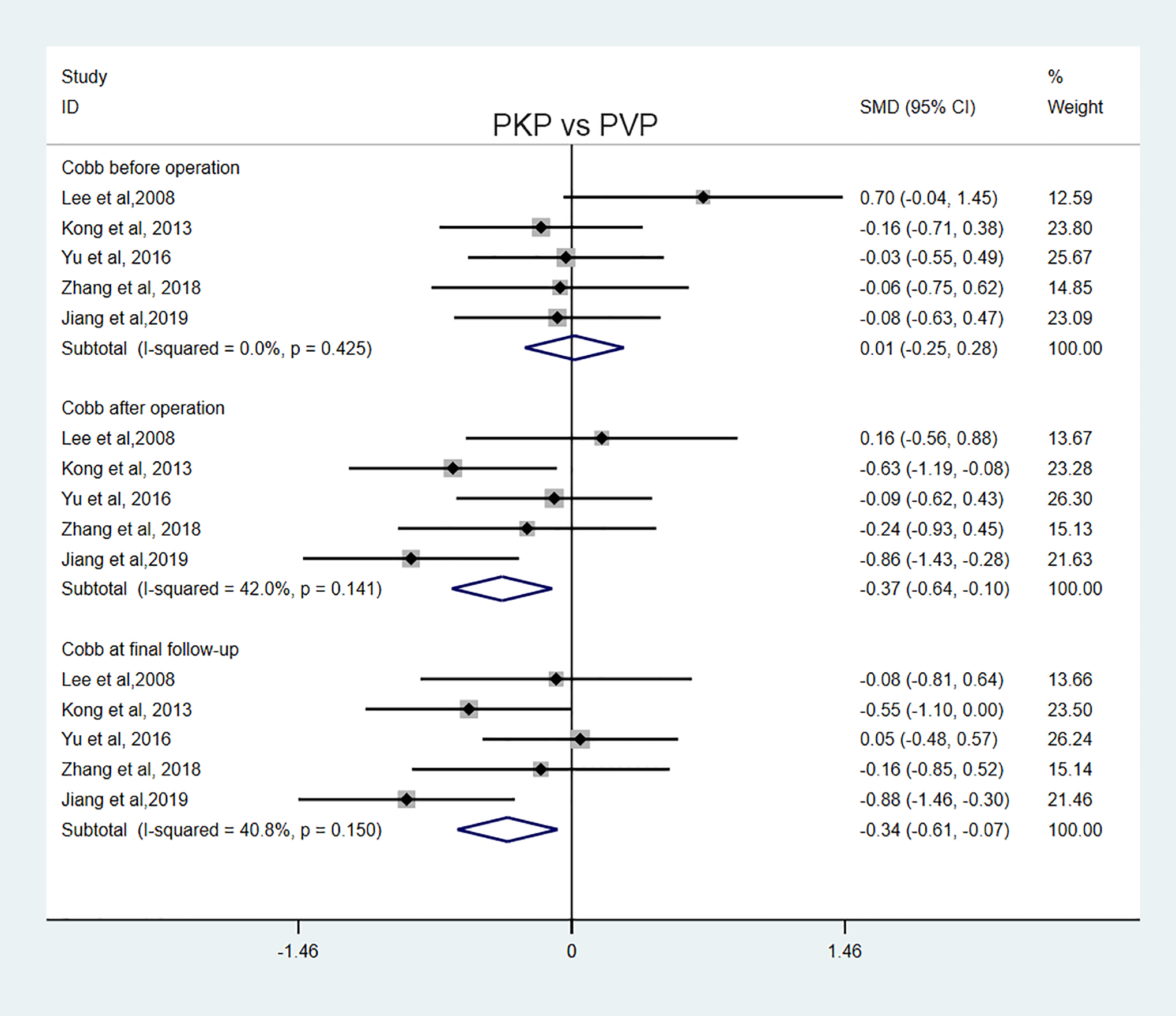
Forest plot of 2 studies estimating the short-term and long-term Cobb angles.
Vertebral height was measured using anterior vertebral height by 3 studies with 94 patients undergoing PKP and 103 undergoing PVP; Ha (%) and Hm (%) were measured by 2 studies with 41 patients undergoing PKP and 43 undergoing PVP. There were no differences between 2 groups in anterior vertebral height before the operation [SMD = −0.27, 95% CI (−0.55, 0.01), P = 0.063] or at the final follow-up [SMD = 0.22, 95% CI (−0.27, 0.71), P = 0.376]; in Ha (%) before the operation [SMD = −0.08, 95% CI (−0.51, 0.36), P = 0.729], after the operation [SMD = 0.28, 95% CI (−0.27, 0.84), P = 0.320] or at the final follow-up [SMD = 0.25, 95% CI (−0.47, 0.97), P = 0.498]; or in Hm(%) before the operation [SMD = −0.10, 95% CI (−0.33, 0.53), P = 0.648] or after the operation [SMD = 0.47, 95% CI (−0.12, 1.05), P = 0.120]. However, the short-term anterior vertebral height and long-term middle vertebral height of the PKP group were slightly larger than those of the PVP group, with a statistically significant difference [SMD = 0.43, 95% CI (0.14, 0.71), P = 0.003; SMD = 0.57, 95% CI (0.12, 1.01), P = 0.012] (Figure 6).
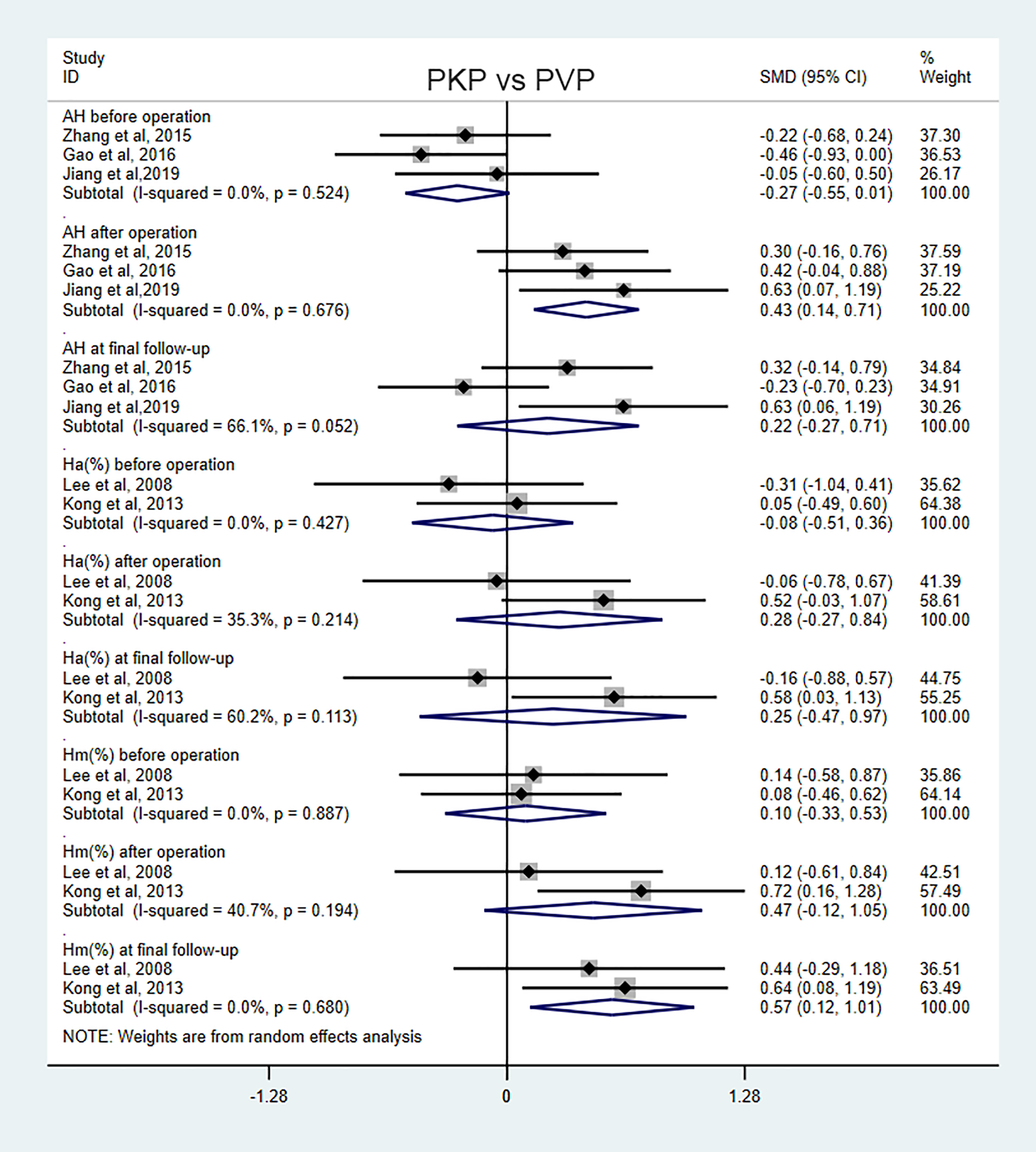
Forest plot of 2 studies estimating the short-term and long-term vertebral heights.
Perioperative Complications (Overall Complications, Bone Cement Leakage and New Vertebral Fracture)
The complication outcomes, including bone cement leakage, new vertebral fracture and overall complications, in different studies were compared. All studies reported information about cement leakage for the PVP and PKP procedures. The combined results showed that PKP was associated with a lower cement leakage rate than was PVP [SMD = 0.50, 95% CI (0.31, 0.81), P = 0.003]. Seven studies with 184 patients undergoing PKP and 225 undergoing PVP reported the rate of new vertebral fractures. The meta-analysis indicated that the rate of new vertebral fractures was similar between the 2 groups [SMD = 0.79, 95% CI (0.36, 1.73), P = 0.560]. In addition, the total complication rate was compared by 7 studies, and no significant differences were observed between the 2 groups [SMD = 0.63, 95% CI (0.39, 1.00), P = 0.051]. Fixed-effect models were used in all above analyses because there was no heterogeneity (I 2 = 0). All the results are shown in Figure 7.
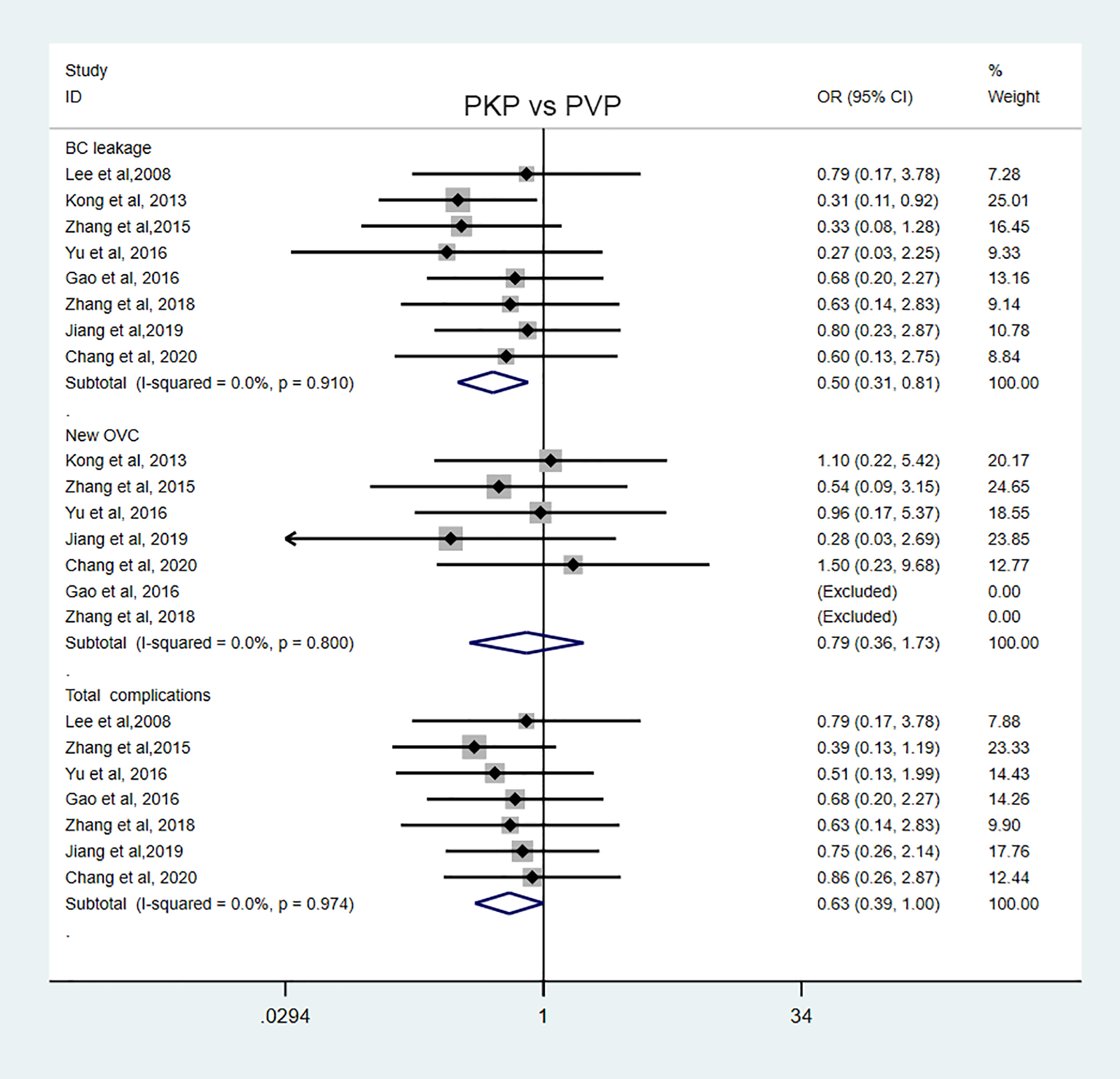
Forest plot of 2 studies estimating bone cement leakage, new vertebral fractures and overall complications.
Intraoperative Resource Consumption (Cement Injection Volume, Operation Time, Fluoroscopy Times, Operation Cost and Blood Loss)
Six studies compared the volume of cement injected, 5 studies reported the operation time, 2 studies reported the number of fluoroscopy times, and 2 studies reported the operation costs. Separate meta-analyses demonstrated PVP was associated with a smaller volume of cement injected [SMD = 0.50, 95% CI (0.27, 0.73), P < 0.001], a shorter operation time [SMD = 1.80, 95% CI (1.40, 1.94), P < 0.001], fewer fluoroscopy times [SMD = 1.02, 95% CI (0.62, 1.43), P < 0.001] and lower operation costs [SMD = 18.20, 95% CI (15.52, 20.87), P = 0.040] than was PKP, with significant differences. Although only one study reported intraoperative blood loss, we found that the volume of blood loss in the PVP group was also significantly smaller than that in the PKP group [SMD = 0.96, 95% CI (0.41, 1.51), P = 0.001]. A random-effect model was employed in the analysis of cement injection volume, operation time and operation cost (I 2 > 50%) but not for fluoroscopy times. All the above results are shown in Figure 8.
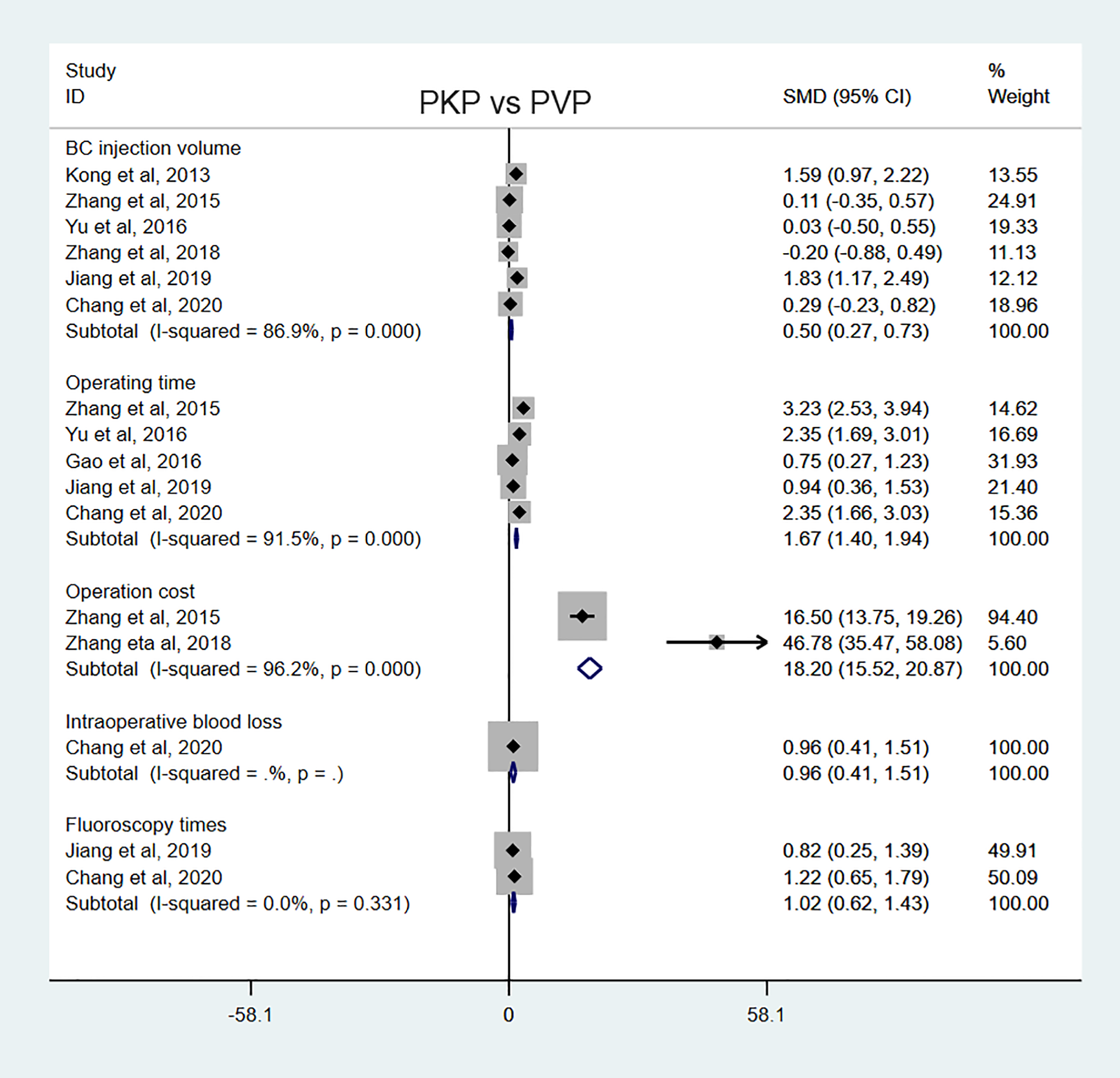
Forest plot of 2 studies estimating the cement injection volume, operative time, fluoroscopy times, intraoperative blood loss and operation cost.
Publication Bias
To detect possible publication bias, a funnel plot for the most commonly reported outcome (cement leakage rate) was generated. The plot showed an adequate symmetrical distribution of points close to the no-effect line. Moreover, none of the studies were located outside of the acceptability range, thus demonstrating satisfactory results. Therefore, the risk of publication bias for this study was low (Figure 9).
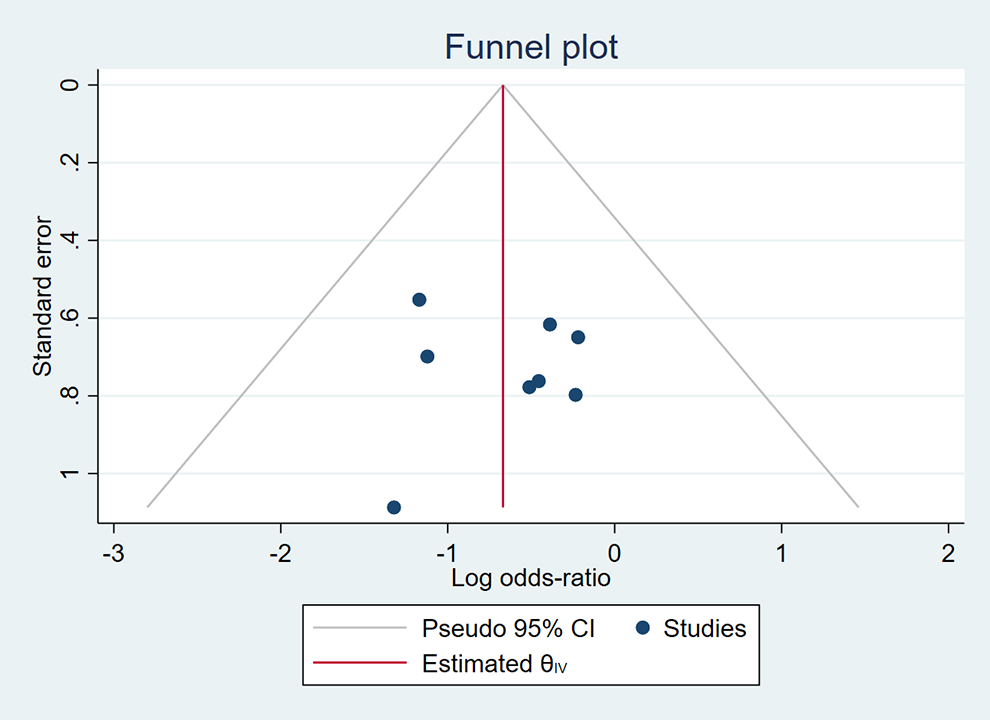
A funnel plot of the cement leakage rate.
Discussion
To the best of our knowledge, this was the first comprehensive meta-analysis aimed at comparing the clinical safety and efficacy of PVP with those of PKP for the treatment of neurologically intact osteoporotic KD. The meta-analysis results revealed that PKP led to better kyphotic deformity correction and a lower cement leakage rate in the treatment of neurologically intact KD, while PVP produced less resource consumption (cement injection volume, operative time, fluoroscopy times, etc.). However, there were no differences between the 2 procedures in clinical outcomes (VAS and ODI), the rate of new vertebral fractures, total complications or most of the vertebral height measurements, with the exception of short-term anterior vertebral height and long-term middle vertebral height.
Clinically, KD is an uncommon and complicated spinal condition associated with progressive and aggravated symptoms with delayed onset, and KD is mainly caused by osteoporosis but is different from typical osteoporotic vertebral fractures.4,42 The pathomechanism, clinical characteristics, imaging manifestations and therapeutic strategies of KD remain inconclusive despite the recent increase in medical awareness and advancements in imaging technology. Currently, avascular osteonecrosis of the vertebral body is widely accepted as a hypothetical pathophysiology, and the intravertebral vacuum cleft, an imaging sign of avascular osteonecrosis, has been highly suggestive of KD.7,42 The treatment of KD is individualized according to the severity of symptoms and the stage of the disease. KD can be divided into 3 phases on the basis of its severity: a less than 20% reduction in vertebral body height without adjacent disc degeneration (stage I), a more than 20% reduction in vertebral body height with adjacent disc degeneration (stage II) and a rupture of the vertebral posterior wall with spinal cord compression (stage III). 43 Generally, patients with symptomatic KD are refractory to conservative treatment because vertebral lesions fail to heal spontaneously. 11 Surgical intervention is the only effective option to alleviate severe pain and prevent further collapse. Admittedly, minimally invasive surgery (PVP or PKP) is often used for patients with neurologically intact KD in stages I and II, while open surgery is recommended as routine management for those in stage III.15,16
To date, increasing clinical studies and meta-analyses have been conducted, and the studies have demonstrated that PKP and PVP are safe and effective methods for pathological vertebral compression fractures and can alleviate pain and improve most patients’ functional status and quality of life.18,27,29,44,45 Furthermore, a recent meta-analysis of more than 2 million patients indicated that the mortality of OVCF patients undergoing vertebral augmentation (PKP or PVP) was 22% less than that of patients undergoing nonsurgical management within 10 years after treatment. 46 In view of these advantages, PVP or PKP has been used to treat neurologically intact KD increasingly more often, and several single-arm studies have shown that both procedures can effectively relieve intractable pain and maintain sagittal balance.1,19,21,22 Subsequently, few comparative studies have directly compared the safety and effectiveness of PVP with those of PKP in treating KD. A retrospective study by Zhang 37 reported that PVP provided comparable pain relief and vertebral height restoration, while PKP was associated with fewer cement leakages. Chang et al 31 prospectively investigated 56 KD patients treated with either PVP or PKP and found that both techniques could achieve similar effects in the treatment of KD, but PVP required less resources, such as less money, a shorter operation time, less blood loss and less radiation exposure. In addition, Yu et al 47 considered that surgical decision-making for PVP or PKP should rely on the clinical stages and status of postural correction of KD patients. Thus, whether one technique is superior in treating KD remains inconclusive, and the current findings are unconvincing due to the limited sample size. Therefore, we conducted a meta-analysis to comprehensively compare the advantages and disadvantages of PVP and PKP for neurologically intact osteoporotic KD.
Regarding clinical outcomes, there were no statistically significant differences in the short-term and long-term VAS and ODI scores between the 2 groups, which was consistent with previous results.31,37,39-41 From a radiological perspective, we found that PKP provided better short-term and long-term kyphosis correction than did PVP. In addition, there were no differences in most of the vertebral height measurements, with the exception of greater restoration of short-term anterior vertebral height and long-term middle vertebral height for the PKP group. As reported by Kong et al, although both PVP and PKP could restore the vertebral body height, reduce the kyphotic angle and could reduce vertebral fractures with clefts with lasting effects, PKP showed a better result in the magnitude of local correction than did PVP. However, another study by Kim et al 48 measured the vertebral HL and segmental kyphotic angle at preoperative, postoperative, and 1-, 3-, 6-, and 12-month postoperative time points and found that PKP yields less HL (PKP 20.5% ± 5.6% vs. PVP 29.8% ± 4.6%, P < 0.001) in the earlier stage. However, no significant differences in vertebral height were observed at the 1-year follow-up (PKP 29.8% ± 6.3% vs. PVP 33.0% ± 5.2%, P = 0.075), which revealed that the PKP group had greater progressive vertebral HL. It was likely that the bone-cement interface induced by a balloon tamponade in PKP contributed to the differences. Regrettably, this meta-analysis actually included 5 studies with nonrandomized data on vertebral height, and only 2 studies reported Ha (%) and Hm (%); thus, the conclusion regarding vertebral height needs to be interpreted with caution and further confirmed by more reliable data from RCTs. Moreover, previous studies30,49,50 have indicated that the magnitude of deformity correction and vertebral height restoration might not affect the clinical outcomes after PKP or PVP, so the radiological findings included in the current study can be regarded as secondary outcomes of this study.
Regarding the safety of the 2 procedures for KD, a consensus has not been reached in previous studies, especially regarding the risk of cement leakage. On the one hand, Zhang et al 37 found that the rate of cement leakage in the PKP group (8.6%) was significantly lower than that in the PVP group (26.3%), and Kong et al 30 reached a similar conclusion (PKP group 20.7% vs. PVP group 66.7%). On the other hand, Jiang 41 and Chang et al 31 showed no differences in the rate of cement leakage between the 2 groups (P > 0.05). This divergence in the cement leakage rate might be the result of a limited number of KD patients being included. This pooled analysis of sufficient data revealed that PVP was associated with a higher risk of cement leakage than was PKP without heterogeneity, which could explain the inconsistency in the arguments in previous studies. In addition, we further demonstrated that there were no significant differences in the rate of new vertebral fractures between the 2 procedures, and homologous results were found in previous studies.30,31,37,38,41 Recently, a meta-analysis revealed that clinical or radiological subsequent fractures on unoperated levels were not associated with PKP or PVP, which might explain our results. 51 As expected, more resource consumption was observed in the PKP group for factors including bone cement injection volume, fluoroscopy times, intraoperative blood loss and operation cost. In view of no striking differences in long-term efficacy between PKP and PVP, these indicators should also be considered indispensable in evaluations, especially for the majority of patients.
Undeniably, statistical heterogeneity could have partly influenced the consistency of the results in this meta-analysis since several confounding factors (e.g., study design, population source, operative skills and follow-up period) varied among studies. Significant heterogeneity occurred in AH and Ha (%) at the final follow-up, bone cement injection volume, operative time and cost. Although fixed- or random-effects models were utilized to reduce heterogeneity, sensitivity analysis and subgroup analysis could not be conducted to identify the origin of heterogeneity because of the limited number of studies or insufficient data. In addition, only one study by Chang reported information about intraoperative blood loss for the 2 procedures.
The limitations of this meta-analysis were as follows. First, all included studies were observational cohort studies, whose qualities were hampered by the lack of randomization, blinding and other relevant methodological procedures, resulting in selection bias, reporting bias, and performance bias. Second, the evaluation criteria for the height of the injured vertebra and other consumption indicators varied among studies, thereby impeding the combination of more homologous data and increasing the risk of heterogeneity. Third, some uncontrollable factors might influence the consistency of the conclusions, such as inter-individual variation in the population and differences in the surgical technologies used, doctors’ operative proficiency, and location of the responsible vertebra. Finally, it is possible that some relevant studies may not have been identified. However, we conducted a comprehensive literature search in available electronic databases and manually retrieved lists of references from the eligible studies; therefore, we tried our best to minimize the risk of studies being missed.
Conclusions
This meta-analysis demonstrated that percutaneous kyphoplasty and vertebroplasty showed similar clinical outcomes, including short-term and long-term VAS and ODI scores, the rate of new vertebral fractures and overall complications, in the treatment of neurologically intact osteoporotic Kümmell’s disease. PKP contributed to relatively greater radiographic improvement and a lower risk of cement leakage but greater resource consumption than did PVP. Based on the available evidence, good clinical judgment should be exercised in the selection of patients for these procedures. Of course, these conclusions should be confirmed by more high-quality and large-sample RCTs in the future.
Footnotes
Authors’ Note
Zhongqiang Chen and Baolaing Zhang conceived and designed the study. Tianqi Fan and Guanghui Chen collected the data. Baoliang Zhang, Guanghui Chen, and Xiaoxi Yang analyzed and interpreted the patient data. Baoliang Zhang and Zhongqiang Chen wrote and reviewed the paper. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.