
Abstract
Introduction
The aim of this study was to evaluate the use of percutaneous curved vertebroplasty procedure (PCVP) and bilateral-pedicle-approach percutaneous vertebroplasty (bPVP) for the treatment of osteoporotic vertebral compression fractures (OVCFs) through a systematic review and meta-analysis of the scientific literature.
Methods
A systematic review of the scientific literature in PubMed, China National Knowledge Infrastructure (CNKI), Wanfang and other databases was conducted in conjunction with different keywords. Nine studies were included; all but 3 were randomised controlled studies and all were prospective or retrospective cohort studies.
Results
We observed statistically significant differences between the PCVP group and the bPCVP group in terms of postoperative visual analogue scale (VAS) scores (mean difference [MD]: −.08; 95% confidence intervals [CI]: −.15 to .00), bone cement leakage rates (OR = .33; 95%CI: .20 to .54), bone cement injection (MD: −1.52; 95%CI: −1.58 to 1.45), operative times (MD: −16.69; 95%CI: −17.40 to −15.99) and intraoperative fluoroscopies (MD: −8.16; 95%CI: −9.56 to −6.67), with the PCVP group being more dominant. There were no statistical differences in postoperative Oswestry Disability Index (ODI) scores (MD: −.72; 95%CI: −2.11 to .67) and overall bone cement distribution rates (MD: 2.14; 95%CI: .99 to 4.65) between the 2 groups.
Conclusions
Meta-analysis showed more favourable outcomes in the PCVP group compared to the bPVP group. PCVP might be effective and safe in the treatment of OVCFs because it relieves postoperative patient pain, reduces operative time and cement injection, and decreases the risk of cement leakage and radiation exposure to the surgeon and patient.
Keywords
Introduction
In osteoporosis, bone density decreases and bone architecture deteriorates, resulting in increased fracture susceptibility and fragility. 1 Osteoporotic vertebral compression fracture (OVCF) is one of the most common fragility fractures, 2 which greatly affects the quality of life of the elderly. OVCF is traditionally treated with bed rest, analgesics, and calcium supplements. Despite the ability to relieve pain, bed rest can worsen osteoporosis and contribute to complications such as deep vein thrombosis, pneumonia, cardiovascular diseases, and cerebrovascular accidents. 3 Surgical intervention can be chosen if the conservative treatment effect is not ideal. 4
PVP is a standard treatment for fractures of the vertebral column, resulting in pain relief and improved stability. 5 Transpedicular puncture can be performed unilaterally or bilaterally during PVP. Although the former has the disadvantage of uneven distribution of bone cement, 6 it is clearly superior to the latter in terms of operation time, trauma, and radiation exposure to the doctors and patients. Bone cement is distributed more uniformly in the latter procedure, but it has many disadvantages, including a large amount of trauma, a lengthy operation time, and a high price tag.7,8
Various clinical reports have described unilateral or bilateral puncture PVP over the last few years, but there have been many studies comparing the 2 puncture methods from a clinical 9 and biomechanical standpoint, with the results tending to favor unilateral puncture. 7 A unilateral PVP approach requires increasing the angle of the puncture unilaterally to create a diffuse and uniform distribution of bone cement between the vertebrae. 10 As a consequence, pedicles may be penetrated, cement can leak, and spinal nerves may be injured.
The PCVP was recently introduced by surgeons. It ensures an even distribution of bone cement within the vertebral body, while also significantly reducing the angle at which the vertebral arch is punctured. 11 With PCVP, bilateral enhancement is achieved through unilateral pedicle puncture to combine the benefits of unilateral and bilateral pedicle punctures. 12
In the current scientific literature, PCVP and bPVP have been compared in the treatment of OVCF in many articles, but systematic and comprehensive meta-analysis is rarely carried out. The purpose of this study was to gather relevant literature and evaluate the differences between PCVP and bPVP in treating OVCF. In order to give surgeons a medical basis for making surgical decisions.
Materials and Methods
Study Selection and Search Strategy
A computer search was conducted for published studies on PCVP and bPVP in the treatment of OVCF as of June 2022. The search strategy was to search common databases at home and abroad: PubMed, EMBASE, Cochrane Library, CNKI, Wanfang Data, China Biomedical Literature Database, etc. In accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines for identifying and screening studies, the search strategy was developed. The following Mesh search headings and keywords were used: “Curved Vertebroplasty, PCVP, Vertebroplasty, PVP, Bilateral, Osteoporotic fractures, Osteoporotic vertebral compression Fracture and OVCF.” A wide variety of Boolean combinations were used to find all eligible studies. We analyzed the reference lists of all the studies and reviews that were identified.
Inclusion Criteria
Our systematic review and meta-analysis included studies which compared the PCVP with the bPVP for OVCF. Inclusion criteria included: (1) currently published controlled studies on PCVP and bPVP in the treatment of OVCF; (2) The study subjects were clinically confirmed patients with OVCF; (3) Intervention measures: PCVP and bPVP; (4) Outcome indicators (including at least one of the following): postoperative VAS score, postoperative ODI score, operation time, bone cement injection volume, X-ray exposure times, bone cement leakage rate and total distribution rate of bone cement. Whenever there were dual (or multiple) studies from a single institution, the most recent study was used.
Exclusion Criteria
Exclusion criteria: (1) controlled studies (observational studies) that did not meet the requirements; (2) studies with nonconforming interventions, such as open surgery; (3) Studies with repeated data publication and incomplete data; (4) Reviews, case reports, animal experiments and cadaver studies.
Data Extraction
Data was independently extracted from the study by Yanxing He and Jianjian Yin. The extracted data describe the characteristics of study design, gender, number of enrolled patients, postoperative VAS score, postoperative ODI score, bone cement injection volume, number of X-ray exposures, bone cement leakage rate and total distribution rate, and operation time. Differences are settled by a third judge after the results are extracted.
Risk of Bias Assessment
An assessment of the bias risk of 3 randomized controlled trials (RCTs) was made using Cochrane Collaboration tools, 13 while the Newcastle-Ottawa scale was used to assess bias risk in cohort studies. Independent assessments of bias were performed by 2 review authors (Yanxing He and Jianjian Yin) for each study included in the review. It will be resolved by discussion with a third author if there is any disagreement during the data extraction and quality assessment process.
Data Synthesis and Statistical Analysis
Revman 5.4 (Cochrane Collaboration) was used for statistical analysis. In this meta-analysis, dichotomous data were calculated by odds ratio (OR). An analysis of continuous data was performed using the mean difference (MD) and 95% confidence intervals (CI). Other statistics, such as P-values and CI, provide missing standard deviations. For example, when the P-value is reported as P < .00001, assuming P = .00001. In order to assess heterogeneity among the combined studies, Cochran’s Q test and the degree of inconsistency (I2) were used. If P > .05 and I2 < 50%, then the fixed-effects model is used. Otherwise, the data is merged using random effects. Statistical significance is defined as a P < .05.
Study Characteristics
According to the above strategies, Figure 1 shows the detailed results of the literature search. A total of 9 articles, including 579 patients (279 in PCVP group and 300 in bPVP group) met the Including criteria. Among these 9 studies, 3 were randomized10,14,15 and 6 were retrospective,11,16-20 all of which compared the treatment of OVCF in the PCVP group with bPVP. Among the included studies, the following characteristics were summarized in Table 1. Meta-analysis flow diagram showing the selection of relevant articles. The Baseline Characteristics of the Studies Included in the Meta-Analysis.

Study Quality Assessment
Randomized Controlled Trials Were Evaluated According to the Cochrane Collaboration Tool.

Analyzing the Quality of Studies in Meta-Analyses Using the Newcastle-Ottawa Scale.

Meta-Analysis Results
Bone Cement Leakage Rate
Cement leakage rates were analyzed in 8 studies, including 263 patients in the PCVP group and 312 patients in the bPVP group. The heterogeneity between studies was low (P = .85; I2 = 0%), using a fixed-effects model. Compared with the bPVP group, the leakage rate of bone cement in the PCVP group was significantly lower (OR = .33; 95%CI: .20 to .54; Figure 2). Meta-analysis and forest plot data for the variable “bone cement leakage rate”.
Bone Cement Injection Volume
Bone cement injection volume was analyzed in 7 studies, including 217 in the PCVP group and 203 in the bPVP group. The heterogeneity between studies was low (P = .52; I2 = 0%) and fixed-effects models were used. In the PCVP group, the volume of bone cement injected was significantly lower than in the bPVP group (MD: −1.52; 95%CI: −1.58 to 1.45; Figure 3). Meta-analysis and forest plot data for the variable “bone cement injection volume”, measured by milliliter.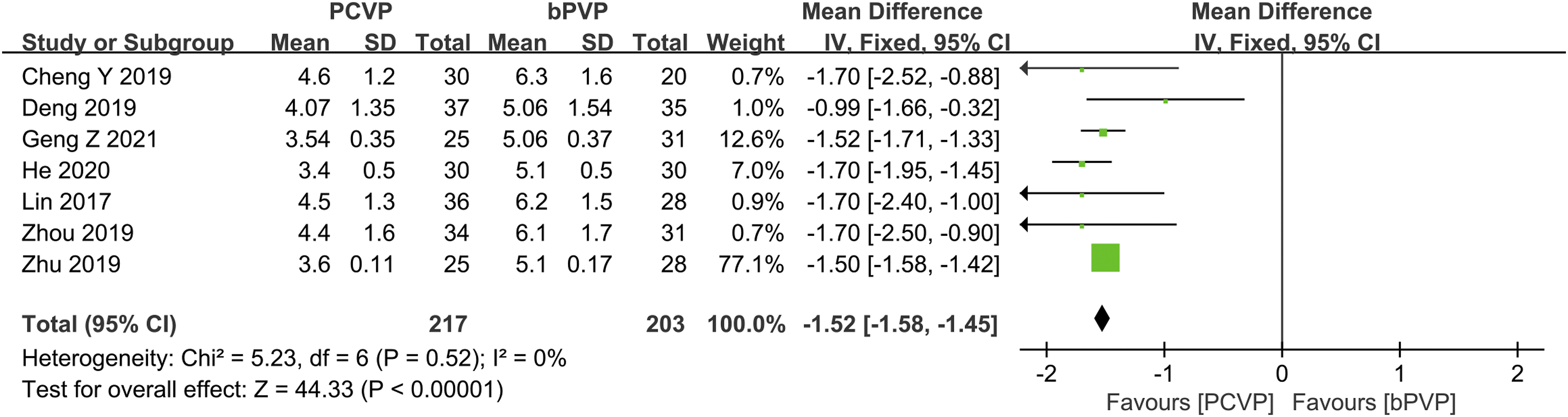
Total Distribution Rate of Bone Bement
Four studies have been conducted, including 126 PCVP patients and 127 bPVP patients, to determine the total bone cement rate. We found that there was low heterogeneity among the 4 studies related to the total distribution rate of bone cement (P = .26; I2 = 25%) and using a fixed-effects model. There was no significant difference between PCVP group and bPVP group (MD: 2.14; 95%CI: .99 to 4.65; Figure 4). Meta-analysis and forest plot data for the variable “total distribution rate of bone cement”.
Postsurgery VAS
An analysis of postoperative VAS was carried out in 9 studies including 279 PCVP patients and 300 bPVP patients. The 9 studies using a fixed-effects model and assessing postoperative VAS (P = .30; I2 = 15%) showed low heterogeneity. As compared with bPVP, PCVP had a lower VAS (MD: −.08; 95%CI: −.15 to .00; Figure 5). Meta-analysis and forest plot data for the variable “postoperative VAS”.
Postsurgery ODI
Four studies with 266 patients analyzed postoperative ODI showed low heterogeneity among studies (P = .93; I2 = 0%) and fixed-effects models were applied. There was no significant difference between PCVP group and bPVP group (MD: −.72; 95%CI: −2.11 to .67; Figure 6). Meta-analysis and forest plot data for the variable “postoperative ODI”.
Surgery Duration
In 9 studies, operation time was analyzed for 279 patients with PCVP and 300 patients with bPVP. We found low heterogeneity among the 9 studies related to operation time (P = .06; I2 = 46%) and using a fixed-effects model. The operation time of PCVP group was significantly shorter than that of bPVP group (MD: −16.69; 95%CI: −17.40 to −15.99; Figure 7). Meta-analysis and forest plot data for the variable “surgical time”, measured by minutes.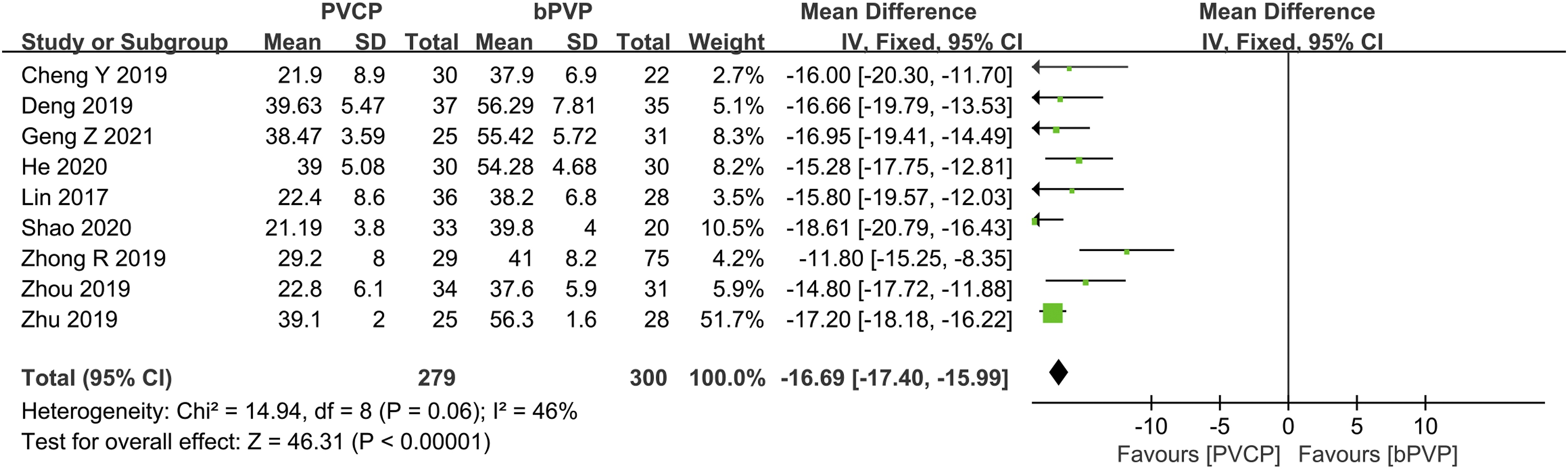
X-Ray Frequency
In 6 studies, including 199 patients in the PCVP group and 211 patients in the bPVP group, the frequency of surgical radiography was analyzed. We found high heterogeneity among the 6 studies related to the frequency of surgical radiography (P = .0002; I2 = 79%) while using the random effects model. Compared to the bPVP group, the PCVP group endured significantly fewer surgical X-rays (MD: −8.16; 95%CI: −9.56 to −6.67; Figure 8). Meta-analysis and forest plot data for the variable “surgical X-rays”, measured by count.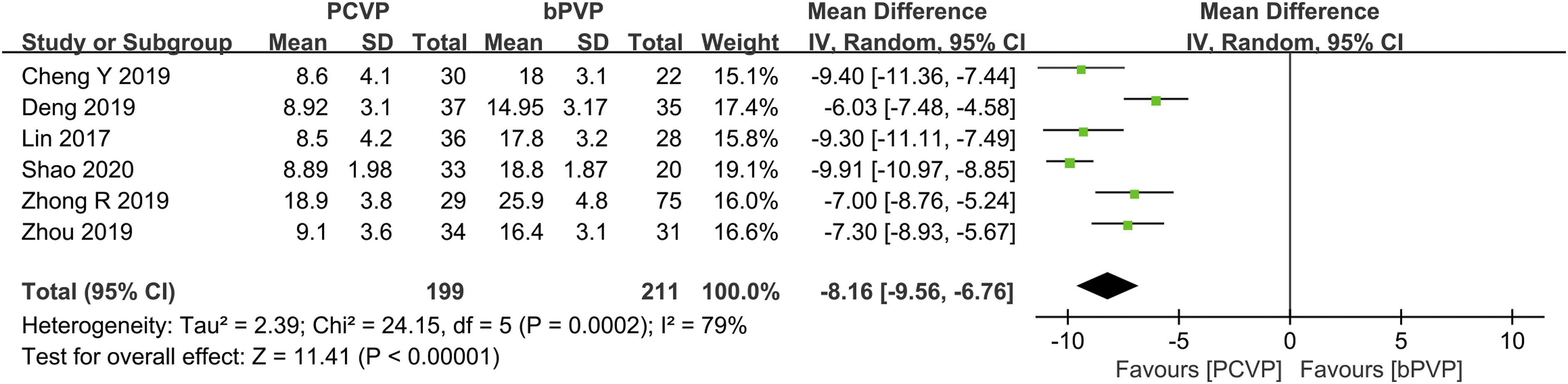
Discussion
Osteoporotic fractures of the spine and thorax are severe complications of osteoporosis that have a high mortality and morbidity rate. The standard treatment for OVCF remains surgical intervention. 21 PVP is a surgical procedure that is conventional, which can quickly alleviate pain and reduce complications after surgery.22,23
Through PCVP (Figure 9B), an angled bending angle vertebroplasty device can be used during unilateral PVP to solve the problems associated with unilateral and bilateral PVP (Figure 9A).
11
During the operation, the bending Angle puncture needle does not need to excessively increase the inclination Angle of the puncture and can reach more locations, resulting in a more uniform distribution of bone cement among the vertebrae affected. Additionally, intraoperative punctures of the medial pedicle wall are reduced, reducing the risk of nerve damage.12,24 (A) Bilateral-pedicleapproach percutaneous vertebroplasty; (B) Percutaneous curved vertebroplasty.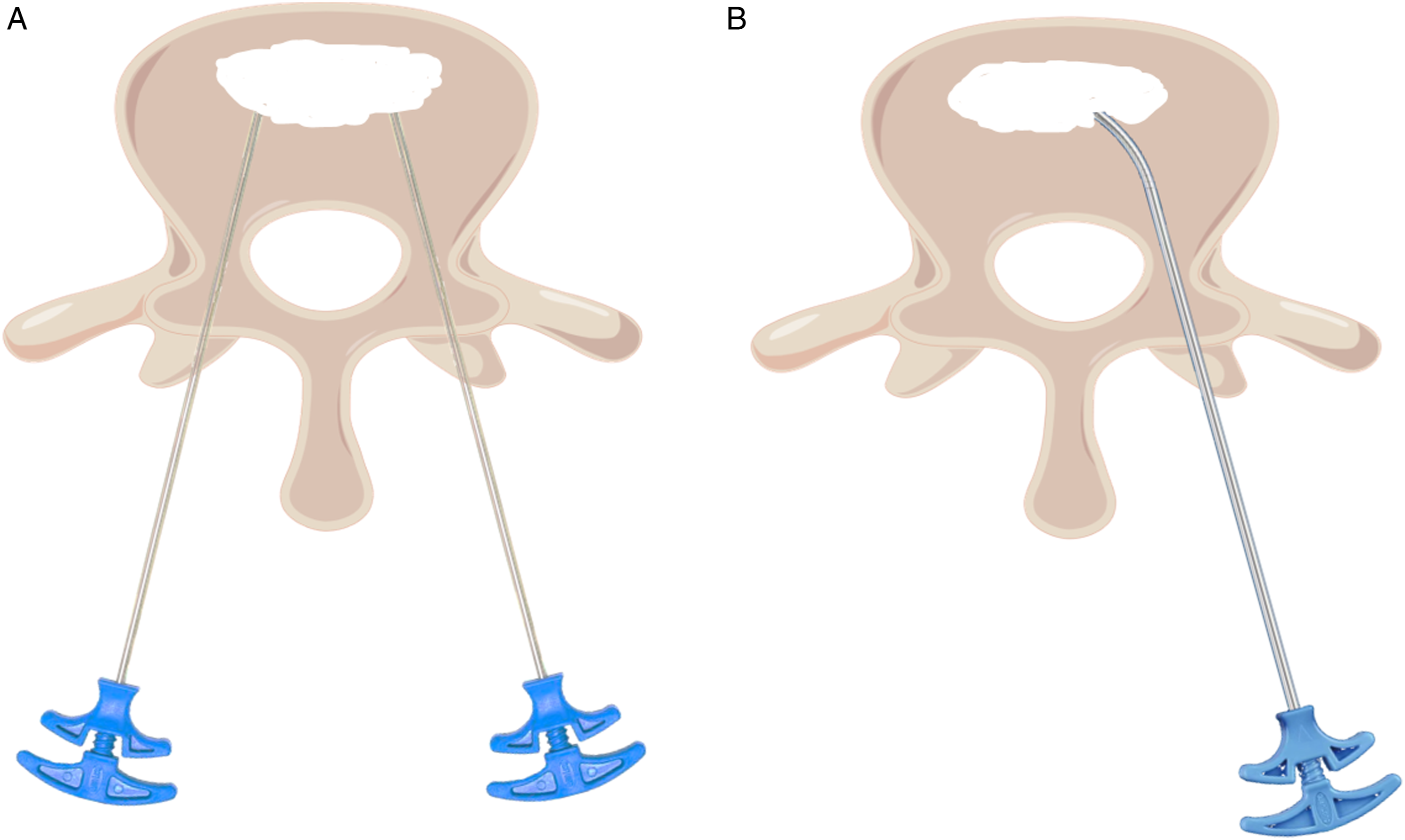
It has been reported 11 that the VAS score of PCVP group and bPVP group decreased significantly after surgery, which indicates that the clinical symptoms of patients were effectively relieved. The results obtained in this analysis suggested that the postoperative VAS score was lower in the PCVP group, which may be related to less surgical trauma and shorter operation time. At the same time, there was no statistically significant difference in postoperative ODI score between the 2 groups, indicating that both surgeries have good clinical effects.
Some articles25,26 have reported the placement of balloons through percutaneous curved vertebroplasty to complete percutaneous curved kyphoplasty, illustrating the feasibility of being able to apply a balloon to percutaneous arcuate vertebroplasty.
Bone Cement Leakage Rate
In PVP, the most common complication is bone cement leakage, which occurs in between 3% and 75% of patients. 27 One study 28 found that the cement leakage rate was highest in the unilateral PVP group due to the increased inclination of puncture. A large amount of bone cement was injected, and pressure was raised on the diseased vertebrae, resulting in bone cement leakage. The bilateral PVP injection pressure and volume were lower, resulting in a lower cement leakage rate. 28
In the PCVP group, the curved injector was used to expand an arc channel in the vertebral body until the contralateral side of the vertebral body, and the bone cement was injected at multiple points while exiting the curved Angle injector. The bone cement was in a low-pressure diffusion state, so the bone cement diffusion and leakage could be observed and controlled at any time, and the bone cement leakage rate was reduced. 29
Bone Cement Injection Volume
Increasing the cement volume excessively isn’t the best way to distribute bone cement widely. Laboratory-based biomechanical studies have found that if bone cement is applied to 15% of the vertebral body, the stiffness can be restored. 30 The vertebral body may be excessively rigid if the volume of bone cement injected exceeds this value.30,31
A critical step in PVP is the injection of bone cement into the fractured vertebrae. Therefore, A major factor in the success of the surgery would be the characteristics of the bone cement itself. There is considerable evidence that cement viscosity and cement volume are 2 of the most important risk factors associated with cement leakage.32,33 When injection volumes of bone cement increase, cement leakage occurs more frequently. The cement should be injected when it is at a “toothpaste-like” consistency following mixing in most previous studies to reduce bone cement leakage. 34 Despite PVP bilaterally puncturing the vertebral body more likely to distribute bone cement symmetrically, it also increases the amount of bone cement injected, increasing the risk of Bone cement leakage.15,35
Studies have also reported that bone cement at both low and high volumes is effective in relieving pain and promoting early recovery of function. 36 The amount of bone cement injected at the same site is related to the degree of osteoporosis, with the higher the degree of osteoporosis the greater the amount of bone cement used. 37 We believe that low level of bone cement may bring better clinical effects, but this needs to be further analyzed according to the specific conditions of patients, so we believe that the conclusion that low level of bone cement may bring better clinical effects is limited.
Surgery Duration
As a result of unilateral PVP, patients suffer less trauma, undergo fewer intraoperative X-rays, and recover from surgical procedures in less time. 38 An even distribution of bone cement within diseased vertebrae is promoted by bilateral PVP, which correlates with pain reduction. 39 It prolongs the surgical procedure, however, and elderly patients are less likely to tolerate bilateral PVP. With the introduction of PCVP, this issue may be resolved by using the specialised bending-angle vertebroplasty device.
The PCVP combines the advantages of both unilateral and bilateral arch access PVP and compensates for the shortcomings of both. The high elasticity of the nickel-titanium alloy allows the needle to reach areas that cannot be reached by a straight-angle metal trocar without emphasising the inward angle of the puncture, which allows greater clinical mobility and helps to achieve uniform bilateral and central cement infusion into the target vertebrae, resulting in bilateral strengthening of the fractured vertebrae. It requires only one puncture, which is a brief procedure that helps improve patient tolerance. 40
Bilateral puncture through bilateral pedicles of ordinary PVP requires 2 puncture operations. During the operation, the bone cement on one side should be filled and then the contralateral bone cement should be injected, which lengthens the operation time accordingly. 15 As compared with bPVP, the PCVP group had fewer G-arm radiographs and shorter surgery durations. 11
In particular, CVP is more suitable for elderly patients who have difficulty enduring long periods of lying in the prone position. Curved nickel-titanium alloy cores maintain a deformation resistance of 35 to 45 N, allowing smooth entry and withdrawal from straight introducers without an excessive effort. However, due to the relatively rigid range of deformation, the curved core may be unable to thread into the vertebral body once the bone becomes too hard, making CVP suitable only for the treatment of the OVCFs. 19
X-Ray Frequency
It is possible to prevent pulmonary embolisms, spinal canal stenosis, spinal cord compression and nerve injuries and other serious complications with intraoperative real-time X-ray fluoroscopy monitoring. 25 The repeated confirmation of the position of the puncture needle and bone cement in the vertebral body also causes the patient and the surgeon to receive more X-ray radiation than the unilateral puncture of curved Angle puncture PVP and ordinary PVP, which has adverse effects on the health of the patient and the surgeon. 15 By using the PCVP bending Angle device, the contralateral vertebral body can be reached, which is similar to bilateral PVP injection of bone cement, reducing the frequency of X-rays and punctures. 41 As compared to bPVP, PCVP had fewer G-arm X-rays and shorter surgical durations. 11
Total Distribution Rate of Bone Cement
Some studies have reported an increased probability of fracture in the diseased vertebrae and adjacent vertebrae after PVP. Analysis of this may be due to the uneven dispersion of bone cement and the inability to increase the stiffness of both sides of the vertebrae in a balanced manner; the stiffness and strength of the vertebrae increase significantly after the injection of bone cement into the diseased vertebrae, while the stiffness and strength of the adjacent vertebrae are relatively weakened due to osteoporosis; the weakened buffering capacity of the discs, resulting in uneven pressure on the endplates of the adjacent vertebrae. 42 Finite element model analysis 43 concluded that the distribution of bone cement in a circular pattern around the vertebral body minimizes the risk of fracture of adjacent vertebrae, and therefore uniform dispersion of the bone cement within the vertebral body and reduction of leakage to the intervertebral disc are of paramount importance. The PCVP provides an ideal biomechanical support by filling the vertebral body with bone cement in a curved pattern through multiple injections with a curved angle injector, effectively reducing the risk of fracture vertebrae. 10
PCVP solves the problem of unilateral cement distribution in the unilateral PVP technique by means of a special bent-angle injector, which can be used to achieve bilateral cement distribution through multiple injections in the injured spine without increasing the angle of inward puncture, 20 and postoperative pain was significantly reduced compared with bPVP group. 11
Our study has several limitations: firstly, heterogeneity is inevitable and should be noted. Secondly, we included only 2 RCTs, which may have led to possible bias between the 2 study groups influencing the results. Secondly, our search strategy was limited to articles published in both English and Chinese languages. Therefore, the conclusions drawn from this study remain to be validated by subsequent larger randomised controlled clinical studies and long-term follow-up.
Conclusion
Compared to bPVP, the PCVP technique had a lower rate of cement leakage and postoperative VAS scores, less frequent cement injection and x-ray exposure and a shorter operative time. Postoperative ODI scores were not statistically significant between the 2 groups and there was no significant difference in the total bone cement distribution rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Project of GUKEXUE (grant no. XK201603).
Ethical Approval
The authors did not conduct any studies involving human participants or animals for this article.
Informed Consent
The study included informed consent from all participants.