
Abstract
Purpose:
This study aimed to compare functional recovery and change in morbidity status from the preoperative levels among patients who underwent two different surgical treatments for unstable intertrochanteric fracture.
Methods:
This retrospective comparative study enrolled 140 patients (aged >80 years) who were referred to two hospitals. Of these, 64 were treated using proximal femoral nail (PFN) and 76 were treated using hemiarthroplasty (HA). To evaluate functional recovery, primary outcome measures were cumulative illness rating scale (CIRS) score to evaluate changes in morbidity status, activity of daily living (ADL) index, and mobility scores.
Results:
The proportion of patients who experienced increased CIRS scores in the HA group was higher at the 3-month follow-up (p = 0.02) but similar at the 6-month follow-up (p = 0.2) in comparison to the PFN group. Treatment with HA, American Society of Anesthesiologists scores of 3–4, and lower, preoperative ADL indexes were the major predictors of increased postoperative CIRS score. Impaired ambulatory ability and the need for walking aids were significantly higher in the PFN group at the 3-month follow-up (p = 0.01 and p = 0.02, respectively) but similar at the 6-month follow-up with respect to the HA group. PFN treatment and high patient body mass index were the major predictors of decreased ambulatory ability at postoperative 3 months.
Conclusion:
HA has several advantages, including early mobilization and decreased dependency. However, it is associated with greater blood loss, a higher need for blood transfusion, and longer surgical duration than PFN, all of which are predisposing factors for significantly higher risk of reduced CIRS scores.
Keywords
Introduction
Intertrochanteric (IT) hip fracture in the elderly is an important public health issue owing to its increasing incidence and an increase in the life expectancy of the general population. 1 These patients tend to have a poor prognosis and experience deterioration in their overall health postoperatively due to the comorbidities associated with substantial morbidity and mortality. 1 –3 Indeed, approximately 30% of these patients die within 1 year postoperatively, while the majority patients who survive experience reduced mobility. 4 Therefore, the successful management of unstable IT fractures in elderly patients may result in healing, lower mortality rate, early restoration of functional capacity, and low reoperation rate.
Since the 1980s, satisfactory clinical outcomes have been reported for stable IT fractures after treatment with a sliding hip screw or proximal femoral nail (PFN). However, the incidence of treatment failure with internal fixation devices for unstable IT fractures has been reported to be up to 50%. 5 In addition, comminution, osteoporosis, and instability often preclude early resumption of full weight-bearing after the internal fixation of unstable IT fractures in elderly patients. 6 While a majority of IT fractures are amenable to internal fixation, the complexity of the fracture or other patient-related factors may compel the orthopedic surgeon to consider hemiarthroplasty (HA) as the treatment of choice. 7,8 HA, which involves core replacement, is not considered as a primary treatment option but can be an alternative for treating unstable IT fractures. 9 Nevertheless, it offers several benefits over internal fixation, including avoiding complications related to lag screw cutout, the lack of risk of fracture nonunion, and the ability of immediate weight-bearing. 10 Regarding the postoperative mortality rate, inconsistent results related to the type of surgery have been noted. 11,12 Compared with PFN surgery, HA has the disadvantages of greater intraoperative blood loss, a higher need for blood transfusion, longer surgical duration, and cementing. 1,12 Based on these findings, we hypothesized that progressive postoperative morbidity is more prevalent in patients treated with HA. However, HA may be advantageous considering early functional recovery; this is because HA allows patients to have immediate weight-bearing capability.
This study aimed to compare functional recovery and change in morbidity status from preoperative levels among patients who underwent two different surgical treatments for unstable IT fractures.
Patients and methods
The current study was approved by the Ethical Research Institutional Review Board (document number: 33216249-604.01.02-E.24145). Informed consent was obtained from all patients, including for the use of clinical data for scientific purposes. This retrospective comparative observational study included 154 patients aged >80 years who were diagnosed with unstable IT fracture between March 2015 and February 2018. Patients with unstable fractures according to the AO classification (31A2.2–A2.3) and those with a history of low-energy trauma were included in the study. We excluded 14 patients with subtrochanteric fractures as well as those with polytrauma, those with fractures associated with a primary or secondary bone tumor, those who were wheelchair-bound or permanently bedridden before the fracture, those who died before the operation, and those who were lost to follow-up. Patients were categorized into two groups according to the treatment center. At one center, three senior surgeons routinely performed HA for the treatment of unstable IT fractures (AO/OTA 31A2.2–A2.3), whereas at the other center, three senior surgeons routinely performed PFN for the treatment of unstable IT fractures (Figures 1 and 2). A total of 64 patients were treated using PFN at an orthopedic referral center, whereas the other 76 patients were treated using HA at another orthopedic referral center. Preoperative and postoperative 3- and 6-month follow-up data were collected.

(a) Anteroposterior radiograph showing an unstable intertrochanteric fracture of the left hip in a 92-year-old woman who fell at the ground level at home. The radiograph was taken 11 months after undergoing treatment using hemiarthroplasty. (b) The design of the proximal part of the femoral stem allows the surgeon to suture or fix the greater trochanter to the femoral stem using cerclage wire or reinforcement sutures.
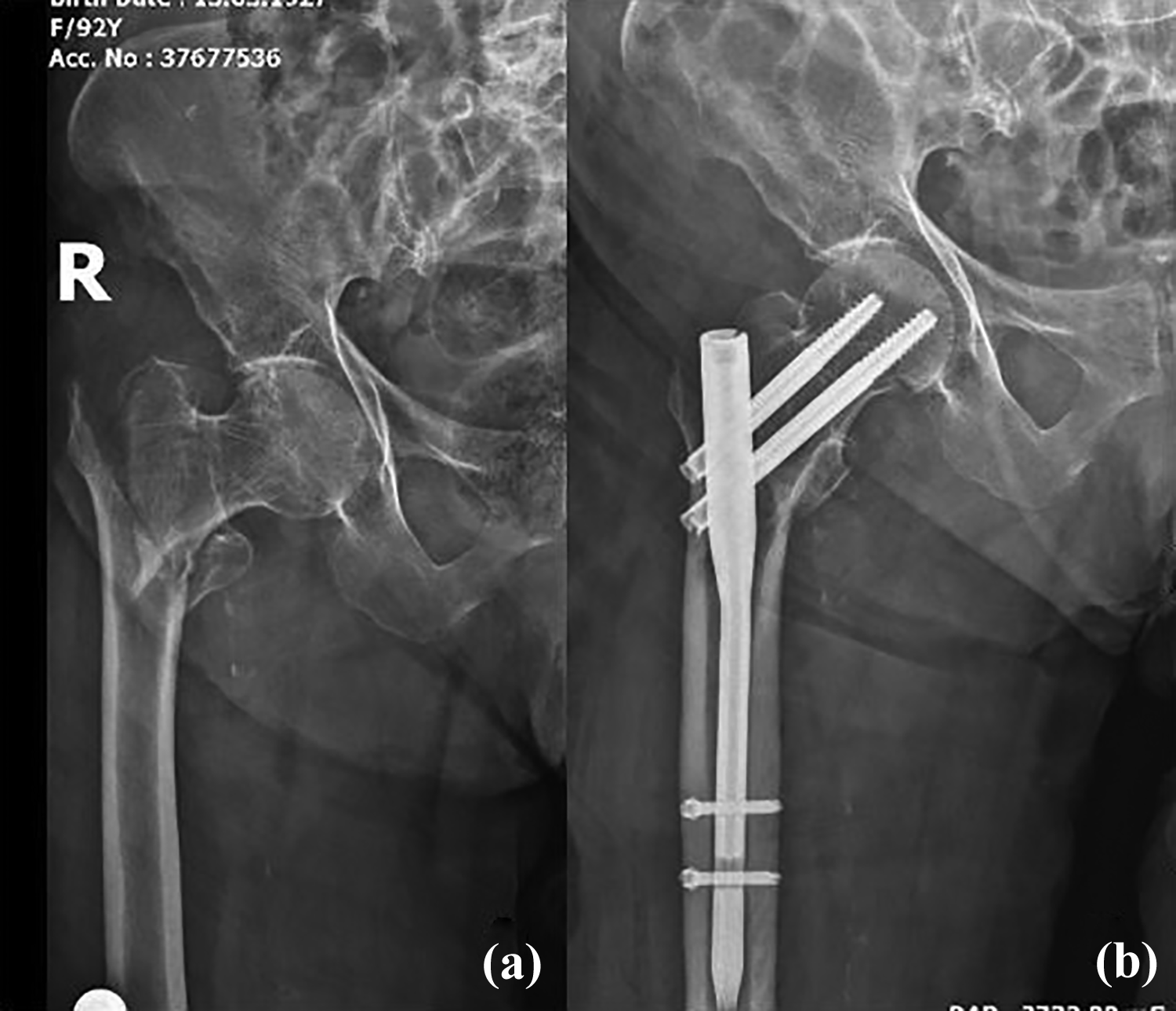
(a) Anteroposterior radiograph showing an unstable intertrochanteric fracture of the right hip in an 81-year-old woman who fell at the ground level at home. (b) The radiograph was taken 4 months after fixation using a proximal femoral nail and shows a united fracture.
Patient demographic data and the presence of preoperative comorbidities assessed using the cumulative illness rating scale (CIRS) and American Society of Anesthesiologists (ASA) scores were recorded as well as the time from injury to surgery and preoperative mobility level with dependence status (Table 1). Comorbidities at admission were identified from the patient’s history, medications, and past medical records. CIRS comprises 13 items for different organ systems, with each system being graded at five levels based on the level of impairment. 13 Organ systems are rated between 0 (no problem affecting that system) and 4 (severe functional impairment). Mobility levels were defined as follows: level I, independent community ambulator; II, community ambulator with aids; III, independent household ambulator; IV, household ambulator with aids; and V, nonfunctional ambulatory. 14 The need for walking aids was investigated using a five-item scale (grade 1, unable to walk; 2, requires accompaniment; 3, two aids/walker, unaccompanied; 4, one aid, unaccompanied; and 5, no need for walking aids). The basic activity of daily living (ADL) index was used for assessing dependency, wherein a score of 6 indicated full function and 1 indicated the most severe functional impairment. 15 The CIRS score, activity level, and ADL index were also assessed at the 3- and 6-month follow-ups to determine whether patients preserved their preoperative status. Logistic regression analysis was performed when a difference was noted between the study groups using univariate analysis. Cognitive status was assessed using the Mini-Mental State Examination (MMSE), which has a maximum score of 30, and scores ≥27 indicated normal cognition. 16 For patients who showed cognitive impairment, information was obtained either from a partner or from a close relative. Furthermore, functionality at each time point was assessed only for those who survived to the end of the study. In addition, intra- and postoperative outcome measures were compared between the two groups.
Main demographic and clinical data by treatment group.

BMI: body mass index; ASA: American Society of Anesthesiologists; CIRS: cumulative illness rating scale; MMSE: Mini-Mental State Examination; ADL: activities of daily living; χ 2: chi-squared test; t: Student’s t-test; SD: standard deviation; DM: diabetes mellitus.
aGrades 6–4 as within the normal range and Grades 3–1 as associated with significant osteoporosis.
Postoperative mortality rates were calculated before discharge (in-hospital mortality) and at 3- and 6-month follow-ups. Follow-up data were collected by telephone from patients or caregivers when required. These interviews were conducted to evaluate the vital and functional status of patients. Data regarding hip status, general complications, and previous reoperations were collected.
Surgical technique
Patients were grouped according to the routine surgical management preferred by the two orthopedic centers. Surgeons at one center routinely performed HA, while those at the other center performed PFN. Thus, patients in the PFN group were treated with titanium PFN, while those in the HA group were treated with calcar-replacement cemented bipolar HA. For PFN surgery, a nail with two proximal 8.5-mm locking screws (TST Profin) or a nail with an 11-mm lag screw and a 7-mm integrated interlocking screw was used (TRIGEN™ Intertan™). The choice of PFN type was dependent on the availability of these devices at the center during interventions. Orthopedic implants are provided to state hospitals according to the national rules of tender that are regulated by law; thus, when patients included in this study presented to these treatment centers, the available PFN types were used. Therefore, the decision regarding the choice of the PFN type was not based on patient or fracture characteristics. Moreover, long femoral nail was not used, and the length of the nails ranged from 18 cm to 22 cm. Two different designs of calcar-replacement cemented bipolar HA were implanted. The femoral component with calcar replacement was cemented using an anterolateral approach in all cases (Figure 1). No revision or long stem was used for patients. The total number of patients with greater trochanter fixated was 18 (23.6%). Fixation was accomplished using cerclage wire or nonabsorbable sutures. A postoperative rehabilitation program was standardized for all patients. Postoperatively, full weight-bearing on the operated limb was allowed at 24 h, except when there were medical contraindications while assuming the standing position or concerns regarding the stability of the fracture fixation. Full weight-bearing was allowed immediately after HA. Postoperatively, antiembolic treatment with enoxaparin sodium for 1 month and analgesics when needed were prescribed. Postoperative follow-up visits, which included a detailed physical examination and radiographic evaluation, were conducted at 6 weeks, 3 months, and 6 months postoperatively, and annually thereafter.
Ethics approval
This study has been approved by the Ethical Review Committee of Erzincan University.
Statistical analysis
Categorical data are presented as frequencies and percentages; continuous variables are presented as mean (±standard deviation) and range. Associations between categorical variables were determined using the χ 2 test. The two-sample t-test was used to compare independent continuous variables. Age- and sex-adjusted univariate and multiple logistic regression analyses were used to identify the determinants of functional capacity and perioperative comorbidity (CIRS score). The following confounding or explanatory variables were tested as the predictors of all outcomes: age, sex, body mass index (BMI), need for walking aids before the fracture (five-step scale), ASA class, MMSE, type of surgical implant, preoperative hemoglobin (Hb) level, time to surgery, length of hospital stay, and early full weight-bearing on the operated limb. The odds ratios for the independent contribution of single explanatory variables were calculated. Statistical post hoc power analyses were conducted for the end points of treatment using the following variables: immediate weight-bearing on the operated limb, the number of patients with an increased need for walking aids, and the number of patients with a decreased ambulatory score. These analyses revealed that a sample of this size was sufficient to detect a clinically significant difference with 100%, 89%, and 95% power. SPSS version 21.0 (SPSS, Chicago, Illinois, USA) was used for data processing and statistical analysis. The level of significance was set at p = 0.05.
Results
A total of 64 and 76 patients in the PFN and HA groups, respectively, participated in this retrospective study. Demographic characteristics, including preoperative functional scores, mental scores, and comorbidities of the two groups, are presented in Table 1. No significant differences were observed between the two groups regarding demographics, Singh classification as a measure of osteoporosis, fracture type, time to surgery, preoperative functional scores, and preoperative ASA and CIRS scores. Perioperative variables of the patients are summarized in Table 2. Significant differences were observed between the two groups regarding perioperative characteristics (blood loss and transfusion rate), postoperative Hb levels, time to partial or full weight-bearing, surgical duration, and hospital stay. Moreover, unacceptable reduction was not detected on postoperative radiographs. The quality of reduction was classified as follows: anatomical, acceptable, or poor reduction (>10 and varus, valgus, and/or ante-retroversion, respectively). Seven of the 64 patients who underwent PFN surgery had poor reduction, 31 had anatomical reduction, and 26 had acceptable reduction.
Perioperative complications and comorbidities from operation to discharge.

PFN: proximal femoral nail; ICU: intensive care unit; HA: hemiarthroplasty; n: number; SD: standard deviation; TIA: transient ischemic attack; DVT: deep vein thrombosis; NS: not studied; χ 2: chi-squared test; t: Student’s t-test.
Mortality
Perioperative (from admission to discharge) mortality rate did not significantly differ between the groups (3 of 64 in the PFN group and 7 of 76 in the HA group; p = 0.3). After adjustment for age, sex, and ASA classification, the difference in the mortality rates between the groups was not significant at the 3-month (p = 0.4) and 6-month (p = 0.6) follow-ups. At the 6-month follow-up, 13 patients (20%) in the PFN group and 17 patients (22%) in the HA group had died.
Reoperation
Six patients (10%) in the PFN group and seven patients (9%) in the HA group had at least one reoperation during the follow-up period, which included lag screw exchange (n = 2), fracture displacement (n = 2), debridement (n = 2 in the PFN group and n = 5 in the HA group), and exchange of prosthesis (recurrent dislocation, n = 1 and deep infection, n = 1). There was no significant difference between the two groups regarding the reoperation rate at the 6-month follow-up (p = 0.9).
Functional recovery
Changes in ambulatory ability, need for walking aids, and ADL index scores are presented in Table 3. The numbers of patients in the PFN and HA groups who showed a decrease in ambulatory ability, an increase in the need for walking aids, and a decrease in the ADL index scores compared with preoperative levels were evaluated to identify relevant predictors. Significant between-group differences were observed at the 3-month follow-up; however, differences at the 6-month follow-up were not significant. Therefore, we performed a logistic regression analysis of only the 3-month follow-up data to identify the determinants of these scores (Table 3). Treatment with PFN and high BMI were identified as significant predictors for decreased ambulatory ability at postoperative 3 months. Additionally, treatment with PFN, low preoperative Hb levels, and female sex were significant predictors for the need for walking aids at postoperative 3 months. The proportion of patients (excluding those who died) who were community or household ambulators before the fracture but were unable to walk or were categorized as nonfunctional ambulators was 9% (n = 5) in the PFN group and 10% (n = 6) in the HA group (p = 0.8) at the 3-month follow-up and 8% (n = 4) in the PFN group and 7% (n = 4) in the HA group (p = 0.9) at the 6-month follow-up.
Predictors of decreased functional and increased morbidity scores during the follow-up at 3-month follow-up.

CIRS: cumulative illness rating scale; ADL: activity of daily living; PFN: proximal femoral nail; BMI: body mass index; Hb: hemoglobin; χ2: chi-squared test; CI: confidence interval.
aPredictors of decreased functional score and increased morbidity scores analyzed by logistic regression analysis. Morbidity and mobility outcomes in this table exclude patients who died within 120 days. Regression analyses were not done for decreased ADL index, because there was no difference in the groups.
Morbidity
The mean preoperative CIRS score in the PFN and HA groups was 4.2 (standard deviation (SD): 2.5 and confidence interval (CI): 3.6–4.9) and 5.1 (SD: 4.3 and CI: 4.0–6.2), respectively (p = 0.48). Deterioration in postoperative CIRS scores at the 3- and 6-month follow-ups was compared between the two groups. The proportion of patients with deteriorated CIRS scores in the HA group was significantly higher than that in the PFN group at the 3-month follow-up (40% vs. 20%, respectively; p = 0.02); however, it was similar at the 6-month follow-up (35% vs. 25%, respectively; p = 0.2). Perioperative factors associated with higher CIRS scores were determined using logistic regression analysis (Table 3). Treatment with HA, an ASA score of 3 or 4, and lower ADL indexes were determined as significant predictors for increased postoperative CIRS scores in patients with unstable IT fractures. Delirium and renal function deterioration were the most common complications in the HA group (Table 2).
Discussion
The treatment of senile IT fractures, particularly unstable fractures, in cases of severe osteoporosis is a clinical challenge. Several studies have evaluated the mortality rate in elderly patients with hip fractures. Consistent with a previous study, 17 mortality rates in the HA and PFN groups were comparable during follow-up. From the first admission to discharge, three and seven patients died in the PFN and HA groups, respectively. The relatively high perioperative mortality in the HA group may be attributed to the higher incidence of transfusion and longer surgical duration, resulting in relatively greater surgical trauma. 18 –20 Additionally, cementing may increase short-term mortality. 7,19 Reoperation in such patients with a high frequency of morbidity may be a devastating complication. Treatment using cephalomedullary nailing of unstable IT fractures occurring in bones with poor quality shows high failure rates. 21 However, we did not observe a difference in reoperation rates between the two groups.
The most important finding of the present study was that patients treated with HA showed superior functional outcomes, whereas those treated with PFN showed better health status scores at the 3-month follow-up. The major advantages of HA included a lower reoperation rate, immediate full weight-bearing, rapid rehabilitation, and decreased duration of hospital stay, all of which served to reduce the risk of clinical problems associated with prolonged inactivity (e.g. pneumonia, venous thrombosis, and decubitus ulcers). 21,22 As indicated in Table 2, approximately 35% and 88% of the patients who underwent PFN surgery and HA, respectively, immediately demonstrated weight-bearing on the operated limb. Thus, HA seems to be a more efficacious treatment. In physical rehabilitation, both physiotherapists and patients may be more conservative toward protecting the fracture area in the PFN group. However, this attitude is similar in the HA group as well. We encountered prosthetic dislocation in only one patient owing to the use of the bipolar HA procedure, which is a safe alternative considering prosthetic dislocation. Nevertheless, surgeons’ warnings about prosthetic dislocation and the patient adaptation process may encourage both the patient and the rehabilitation team to be more protective to prevent such dislocations. Reportedly, restricted weight-bearing after surgery for hip fracture is more frequently allowed for patients who undergo osteosynthesis than for those who undergo arthroplasty. 6,23 Additionally, nonweight-bearing status is associated with poor 1-year functional outcomes because of the accelerated loss of muscle mass in elderly patients. 6 Early walking with full weight-bearing following bipolar HA is believed to be a major contributing factor underlying these results. 17,24 The determinants of postoperative functional levels in patients with hip fracture include preoperative time to surgery, nutritional status, cognitive impairment, preoperative autonomy and dependency, ASA score, and nonweight-bearing status. 1,6,25 Functional levels before fracture may be the most consistent predictor for rehabilitation. 12,26 In our study, the major determinants of decreased ambulatory capacity were implant type (PFN) and high BMI. Furthermore, implant type (PFN), sex (female), and low preoperative Hb levels were also major determinants for the need for walking aids at the 3-month follow-up.
The number of patients who showed increased CIRS scores was significantly higher in the HA group than that in the PFN group. Reportedly, morbidity is a key determinant for mortality and physical disability.27 Factors such as anemia, blood transfusion need, delirium, longer hospital stay,18 reoperation, postoperative infection, and cemented implant type are associated with mortality and physical disability. However, few studies have investigated the differences in patient ASA or CIRS between postoperative levels and postoperative follow-up. In a study by Kim et al., the mean preoperative ASA score of elderly patients with hip fractures was 1.9, whereas the postoperative ASA score at the 3-year follow-up was 2.3. However, the authors did not identify predictors for increased ASA scores. 20 In the present study, treatment with HA, a preoperative ASA grade of 3 or 4, and low ADL indexes were the major predictors for increased CIRS scores. Therefore, orthopedic surgeons should consider that hip fractures may not only induce a progressive deterioration in the patient’s general health status, with significant increases in the risk of morbidity over time, but can also result in immediate death of the patient. 27
There are some limitations to this study. The potential long-term complications of prosthetic replacement such as loosening, acetabular erosion, stem failure, late infection, and late dislocation were not identified. Moreover, patients could not be randomized due to the retrospective design of the study; however, the retrospective, cross-sectional design of the study also provided the advantage of avoiding potential patient selection bias. Another strength of the study includes comparative analyses of the clinical and radiographic outcomes in specific patient populations. Furthermore, we performed univariate and multivariate analyses of many different parameters to achieve a better understanding of the role of surgery type over future functional recovery and morbidity status.
In conclusion, HA has several advantages over PFN surgery for the treatment of unstable IT fractures, including rapid functional recovery due to early postoperative mobilization and decreased dependency. However, HA is associated with greater blood loss, a higher need for blood transfusion, and longer surgery time, resulting in a significantly higher risk of deterioration in morbidity status compared with PFN surgery.
Footnotes
Author contributions
Authors HU, YC, and HS contributed to the study design, analysis of literature, analysis and interpretation of data, and manuscript writing and AC, MK, and HD were involved in data collection, analysis of literature, manuscript editing, and performing measurements.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.