
Abstract
Purpose:
Treatment for an unstable intertrochanteric fracture in elderly patients is challenging. Bipolar hemiarthroplasty (HA) using microarc oxidation (MAO) coating has been a treatment option alternative to internal fixation. However, the outcome of bipolar HA using MAO-coated stem in these patients is unknown.
Methods:
From July 2007 to April 2016, 234 (older than 65 years) patients (234 hips) who were diagnosed as having unstable intertrochanteric fractures were treated with bipolar HA using a fully MAO-coated standard-length rectangular cementless stem. During the arthroplasty, the greater trochanteric and the medial fracture fragments were attached to the stem and fixed with two to three 16-gauge wires. Forty-eight patients (48 hips) died within postoperative 2 years. The remaining 186 patients (186 hips) were followed up for a mean of 4.3 (range 2–10) years.
Results:
With the exception of 4 patients who died during hospitalization, 176 of 230 ( 76.5%) patients could ambulate independently with or without an assistive device at the time of hospital discharge. Venous thromboembolism occurred in seven patients (3.0%). One hip dislocated due to a fall 1 month after the arthroplasty. Periprosthetic femoral fracture occurred in four patients and periprosthetic acetabular fracture in one patient. One patient had periprosthetic of acute pyelonephritis. There was no focal osteolysis around the femoral stem.
Conclusion:
The result of cementless HA using MAO-coated stem enabled early ambulation in most (76.5%) of elderly patients with unstable intertrochanteric fractures and the results were encouraging.
Introduction
There are multiple modalities of treatment for intertrochanteric fractures. 1 –4 Surgeons determine the surgical method considering patient’s age, underlying comorbidities, quality of bone, type of fracture, and the degree of comminution. Surgical options include plate and screw fixation, intramedullary nailing, and arthroplasty. 1 –3,5,6
However, the treatment for an unstable intertrochanteric fracture with a posteromedial defect (AO/OTA 31-A2) in elderly patients still remains challenging. These patients have poor bone quality, and internal fixation is often associated with complications, such as screw cutout, loss of fixation, or implant failure. 7
In elderly patients with intertrochanteric fracture, early mobilization is mandatory to minimize the risk of complications due to prolonged recumbency, 1 and bipolar hemiarthroplasty (HA) has been an alternative to internal fixation. 8 –10
Although cemented stems were used to obtain stable fixation in osteoporotic femur of these patients, 11 cement-related cardiopulmonary complications appeared as a matter of concern. 11,12
Among cementless femoral stems, rectangular stems can afford sufficient rotational stability even in osteoporotic femur avoiding cement-related complications. 6
Microarc oxidation (MAO) is an electrochemical oxidation forming nanoporous pits and thick oxide layers on the metal surface. This technique has been used to enhance bone ingrowth of femoral stem, 13 and the results of cementless HA using MAO-coated stem in patients with femoral neck fracture were encouraging. 13
However, the outcome of this type of HA in patients with unstable intertrochanteric fracture, which has a large fracture fragment including lesser trochanter, is unknown.
The purpose of this study was to determine clinical and radiological results of cementless bipolar HA performed using an MAO-coated standard-length stem in unstable intertrochanteric fracture in elderly patients.
Materials and methods
From July 2007 to April 2016, 243 patients (243 hips) aged 65 years or older were diagnosed as having an unstable intertrochanteric fracture; three parts or more intertrochanteric fractures with a loss of posteromedial cortical buttress (AO/OTA 31-A2) 14 were treated with bipolar HA with the use of a fully MAO-coated rectangular stem at our hospital.
Six patients, who underwent HA after a failure of internal fixations, and three patients, who underwent HA due to pathologic fractures, were excluded. The left withb234 patients (234 hips) as the study’s subjects. There were 49 men and 185 women, their mean age at the time of surgery was 80.6 years (range 65–96 years), and the mean body mass index was 22.0 kg/m2 (range 13.4–31.6 kg/m2). Their mean American Society of Anesthesiologists score was 2.3 (range 1–4). The ambulatory ability before injury was obtained from patients or their family members at the time of admission and classified according to Koval’s categories. 15 The mean preinjury Koval category before the injury was 2.5 (range 1–5).
We used a fully MAO-coated titanium alloy stem (Bencox stem; CORENTEC, Cheonan, South Korea) (Figure 1). This is a double-tapered, rectangular-shaped, standard-length titanium stem.

The Bencox stem is a double-tapered, rectangular titanium stem and extensive MAO coating on the surface without collar. MAO: microarc oxidation.
In 2008, the manufacturer removed shoulder edge of the stem to avoid varus insertion of the stem design. The mean roughness of the stem surface is 5.5 µm. The stem length ranges from 131 mm to179 mm and the stem width at middle ranges from 8 mm to 20 mm in 1-mm increment.
The rectangular geometry of Bencox stem affords sufficient rotational stability even in the weak osteoporotic femur. In our previous study, the results of bipolar HA with the use of Bencox stem were satisfactory without loosening of the stem in elderly patients with displaced femoral neck fractures. 13
The acetabular component was a cobalt–chromium cup (IC Bipolar Head, Implantcast GmbH, Buxtehude, Germany), which has a ultrahigh-molecular-weight polyethylene liner inside. A 28-mm alumina head was used in 210 hips, 28-mm metal head in 2 hips, and 22-mm metal head in 22 hips.
All operations were performed through a posterolateral approach by four senior hip surgeons. A total of 209 patients were operated under spinal anesthesia, and 25 under general anesthesia.
After rasping the endosteal cavity of the proximal femur, we used a stem trial to check the stem size, stability, and leg length. During the operation, in our patients, the greater and lesser trochanters were fractured off from the main fragment of the distal femur. Thus, it was difficult to restore and adjust the leg length. To adjust the leg length, we used the method described by Lee et al. 16 With the use of the trial components, the optimal stem size and head length were determined. If the size, stability, and leg length were satisfactory, the stem was inserted into the femoral canal with a firm impaction from a gentle tapping to a press fit.
Then, the greater trochanteric and the medial fracture fragments were attached and fixed with two to three 16-gauge wires with the technique, which was described elsewhere. 16 Usually, the greater trochanter was fixed with one vertical wire, which was inserted through a hole drilled in the lateral femoral cortex below the abductor tubercle and a hole in the upper portion of the fractured greater trochanter. The medial fragment was fixed with one to two circumferential wires. The wires were tightened and tied with Kirschner wire bows. 16
Patients were instructed to stand with assistance, with unrestricted weight-bearing and use of an assistive device, as tolerated, on the second or third postoperative day. As the walking ability improved, the assistive device (walker, crutches, or cane) was changed as determined appropriate by a physical therapist. After hip surgery, patients are not allowed to squat for 1 month.
No prophylactic regimen for thromboembolism was used until 2009. Since 2010, mechanical prophylaxis using intermittent pneumatic compression device was used.
Follow-up evaluations were performed at 6 weeks; at 3, 6, 9, and 12 months; and every year thereafter.
Our patients were older than 65 years with a mean age of 80.6 years and had a life expectancy of 7.14 years for men and 9.02 years for women according to a life chart. 17 Thus, we extended this portion of the review to include the hips that had been followed up for more than 2 years for a complete analysis of this age-group.
The clinical evaluation was performed using the Koval’s categories for walking ability. 15
The radiographical evaluation was done by two independent observers who did not participate in the operation. The 6-week anteroposterior and cross-table lateral radiographs were considered to be the baseline studies for radiographical comparison. The serial radiographical evaluation included an assessment of the stability, 18 osteolysis around the femoral component, 19 subsidence of the femoral components, 20 the presence or absence of acetabular erosion and cortical porosis around the femoral component, 21,22 heterotopic ossification, 23 and leg length discrepancy. Osteolytic lesions, spot welds, pedestal formation, and reactive lines, if present, were located according to the seven zones described by Gruen et al. 24 To evaluate the leg length discrepancy, we measured the distance between the interteardrop line and the lower margin of the lesser trochanter. The distances of the operated limb and the contralateral limb were compared, and the difference of more than 2 cm was defined as the failure of leg length equalization. 25
The design and protocol of this retrospective study were approved by the institutional review board in our hospital, which waived informed consents.
Results
The mean operating time was 92.2 min (range 55–170 min). The mean estimated blood loss was 576.8 mL (range 135–1340 mL). Of the 234 patients, 154 (65.8%) received transfusion (mean 582.6 mL; range 100–1600 mL) perioperatively.
No patient had cardiopulmonary complications during the operation.
Distal extension of the original fracture occurred intraoperatively in 10 hips (4.3%, 10 of 234). All of the intraoperative cracks were treated with cerclage wires, and these patients ambulated with a walker for 4 weeks after the arthroplasty.
Mean length of hospital stay was 26.1 days (range 6–167 days). Four patients died during the hospitalization. Three patients died of pneumonia and one died due to acute renal failure. With the exception of these 4 patients, 176 of 230 (76.5%) patients could ambulate independently with or without an assistive device at the time of hospital discharge after the operation.
Forty four patients (44 hips) died due to problems unrelated with the arthroplasty after discharge within postoperative 2 years. The remaining 186 patients (186 hips) were followed up for more than 2 years (mean 52.4 months; range 24–122 months).
Orthopedic complications developed in 10 patients postoperatively (Table 1).
Orthopedic complications postoperatively.

One hip dislocated 1 month after the arthroplasty. During the manual reduction, the bipolar cup was dissociated from the head. Thus, this patient was treated with open reduction and change of the femoral head.
Periprosthetic femoral fracture (PFF) occurred in four patients: two Vancouver type B1, one Vancouver type B2, and one Vancouver type C. Of the two Vancouver type B1 PFFs, one fracture was treated with open reduction and plate fixation, and the other was conservatively treated with teriparatide. The patient who had Vancouver type B2 PFF at postoperative 7 years was treated with stem revision using a modular long stem. The patient who had Vancouver type C PFF at postoperative 7 months was treated with open reduction and plate fixation.
One patient had periprosthetic acetabular fracture at postoperative 8 years and was treated with conversion total hip arthroplasty.
One patient sustained pubic ramus fracture at postoperative 2 years and was treated conservatively.
Otherwise, there was no reoperation or revision.
Trochanteric nonunions occurred in three patients and did not disable the patients (Figure 2).

(a) An 84-year-old woman sustained an unstable intertrochanteric fracture. (b) An anteroposterior radiograph obtained immediately postoperatively shows well-fixed greater trochanteric fragment with wires. (c) An anteroposterior radiograph obtained 6 months postoperatively shows broken wires and gap between the proximal femur and the greater trochanter fragment. (d) An anteroposterior radiograph obtained 2 years postoperatively still shows gap without migration proximally. However, the stem is well-fixed with a stable bone ingrowth and she walks independently without any symptom.
One patient had periprosthetic infection at 3 years during treatment of acute pyelonephritis. This patient was treated with implant removal, debridement, and antibiotics-loaded cement spacer. She could ambulate with crutches and refused second-stage reimplantation.
Medical complications developed in 14 patients postoperatively (Table 2).
Medical complications postoperatively.
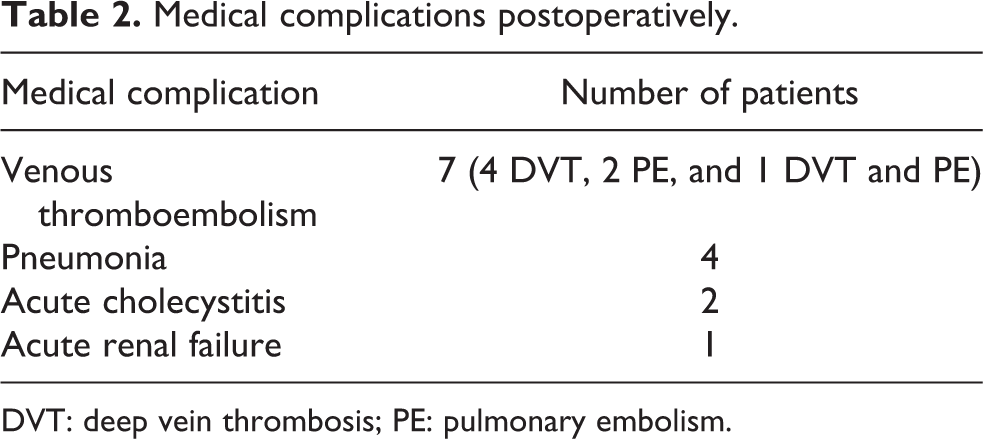
DVT: deep vein thrombosis; PE: pulmonary embolism.
At the latest follow-up, mean Koval score was 4.2 (range 1–7). Based on the levels according to Koval’s categories, 15 29 (15.6%) patients did not drop the level of ambulatory ability, 77 (41.4%) patients dropped one level of ambulatory ability, 35 (18.8%) patients dropped two levels, 21 (11.3%) patients dropped three levels, and 24 (12.9%) patients dropped four or more levels, comparing between ambulatory ability before fracture and at the final follow-up. Twenty (10.8%) patients became nonfunctional ambulatory at the final follow-up; one of these patients was a community ambulator before sustaining fracture and 19 were household ambulators.
Radioreactive line was found in Gruen zone 1 in one hip, but the lucent line did not progress downward. Otherwise, there was no focal osteolysis around the femoral stem (Figure 3).
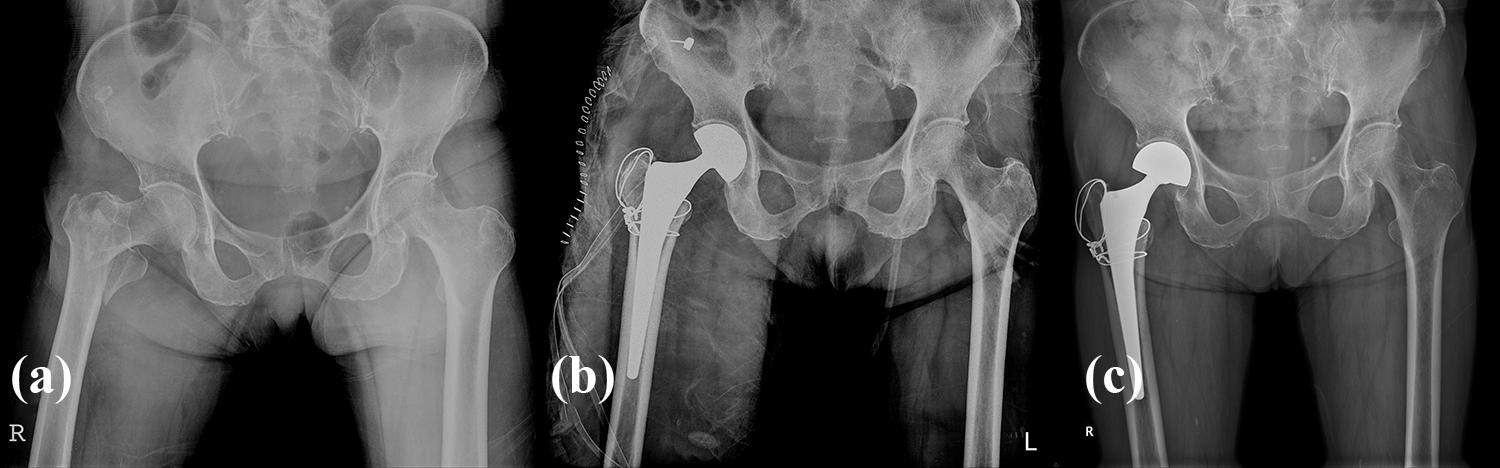
(a) A 79-year-old woman had an unstable intertrochanteric fracture with a posteromedial defect. (b) She was treated with bipolar hemiarthroplasty using MAO-coated stem and circumferential wires. (c) At 5 years after the arthroplasty, she had no pain and could ambulate without any assistive device. The stem was well-fixed as shown in the radiograph. MAO: microarc oxidation.
There was no subsidence of stem. Heterotopic ossification was observed in four hips (1.7%); Brooker grade II in two hips, and grade III in two hips. Heterotopic ossification did not affect clinical outcome. No patient had leg length discrepancy >1 cm.
There was minimal acetabular erosion in 10 hips (5.4%).
After all, during the follow-up period, only six reoperations were performed due to one dislocation, one periprosthetic acetabular fracture, one periprosthetic infection, and three PFFs.
Discussion
Our study shows that a cementless HA with the use of a MAO-coated stem relieves pain, restores ambulatory function, provides long-term stability of the implant, and is associated with few complications in unstable intertrochanteric fractures of elderly patients. The result is compatible or better compared with previous results of internal fixation or HA using cemented stems. 11,21,26,27
Osteosynthesis of unstable intertrochanteric fractures in osteoporotic patients is sometimes associated with complications including cutout of the femoral screw, breakage of the nail, and fracture of the femoral shaft. 3,4,28 –33 Moreover, conversion hip arthroplasty of failed internal fixation is technically difficult and is associated with a high complication rate. 34 For these reasons, some authors recommended cemented HA as an alternative to internal fixation for unstable fractures in elderly patients. However, cardiopulmonary complications are serious risks of the cementation in elderly osteoporotic patients. 35
Cementless HA with the fixation of the trochanteric fragments appeared as a good option for unstable intertrochanteric fractures in the elderly. 16,21 Göçer et al. compared cemented and cementless HAs for unstable intertrochanteric fractures. In their study, no stem was loose in the cementless group, while three stems were loose in the cemented group. 26 Other authors also favored the use of cementless stems in that type of fracture because of reduced operating time, intraoperative blood loss, stem loosening, and risk of cardiopulmonary complications. 12,26,36,37 In our study, the mean operative time was 92.2 min (55–170 min), average intraoperative blood loss was 576.8 mL (135–1340 mL), and no patient had cardiopulmonary complications. Bipolar HA for unstable intertrochanteric fracture might be associated with more blood loss and longer operating time than internal fixation. However, we could not compare the two groups because of lack of control subjects.
Postoperative mortality is high after hip fracture surgery in elderly people. 38,39 In a prospective study by Elmorsy et al. on 36 HAs due to unstable intertrochanteric fractures, there was no mortality within the first 60 days from the surgery, and five patients (12.19%) died within the first 1 year due to cardiac complications. 27 In our study, there were 7 deaths (7 of 234, 2.9%) within 30 days, 18 (18 of 234, 7.7%) mortalities within 90 days, and 30 (30 of 234, 12.82%) mortalities within 1 year.
We have previously reported a technique of trochanteric fixation in cementless HA for unstable intertrochanteric fractures. 16 The same technique was used in our patients and only 1 of 62 patients had nonunion of the trochanteric fragment.
There are several advantages in the use of the stem design, which was used in our study. It is a tapered rectangular stem with MAO coating, which fits into the metadiaphyseal junction of the femur below the lesser trochanter. With this kind of stem, initial stability and long-term biologic fixation can be obtained even in the osteoporotic proximal femur. 13 Cardiopulmonary complications, the amount of blood loss, and operative time can be reduced in cementless stems compared with cemented stems. 12 After the insertion of a cementless stem, fracture fragments can be easily attached and fixed to the proximal portion of the stem with cerclage wires. 16 On the other hand, surgeons should be cautious about iatrogenic femoral crack during insertion of cementless stem into the osteoporotic femur of elderly patients.
There were several limitations in our study. First, our study was a retrospective one performed in a cohort of serially observed patients, and the follow-up period was short. However, a long-term follow-up study is barely possible and has little clinical relevance in elderly patients, who have a short life expectancy and limited activity during their life. Second, our study did not include a comparison between internal fixation and arthroplasty, although cementless bipolar HA for unstable intertrochanteric fracture might be associated with iatrogenic femoral crack, more blood loss, and longer operating time. Another limitation of our study is the lack of a comparison with cemented bipolar HA. Because we were very concerned about cement-related adverse effect, we did not use any cemented stem during the study period. Hence, such a comparison group could not be recruited.
Despite these limitations, our study demonstrated that a bipolar HA using a rectangular cementless stem with full MAO coating is a satisfactory option to treat unstable intertrochanteric fracture of elderly patients.
Conclusion
The result of cementless HA using MAO-coated stem enabled early ambulation in most (76.5%) of elderly patients with unstable intertrochanteric fractures, and the results were encouraging with a low incidence of venous thromboembolism and stem loosening.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.