
Abstract
Purpose:
The purpose of this study is to evaluate the efficacy of percutaneous endoscopic debridement and drainage (PEDD) in patients with surgical site infection (SSI) following instrumented lumbar fusion.
Methods:
We retrospectively reviewed the medical records of 20 patients (6 women and 14 men; average age, 60.1 years) who underwent PEDD at our institute to treat SSI following instrumented lumbar fusion from January 2010 to December 2015. The terminal event, or failure of PEDD treatment, was defined as a shift in treatment methods to open surgery. Risk factors were analyzed to determine their effect on the therapeutic results of PEDD. Clinical outcomes were assessed by careful physical examination, regular serologic testing, and imaging studies to determine whether continued conservative treatment or open surgery was necessary.
Results:
Causative bacteria was identified in 17 (85%) of the 20 biopsy specimens. Successful infection control through PEDD was identified in 13 patients (65%). Both the visual analog scale and Oswestry disability index significantly improved in these patients. Detection of the causative pathogens was the only risk factor influencing the terminal event in the remaining seven patients (35%).
Conclusion:
In this study, PEDD was an effective treatment approach for obtaining a bacteriological diagnosis, relieving the patient’s symptoms, and assisting in eradication of SSI following instrumented lumbar fusion. The use of species-specific antibiotics for the offending pathogens appears to be the most important factor to determine the success rate. The indications of this procedure could be extended to treat patients with SSI after instrumented lumbar fusion.
Introduction
Instrumented spinal fusion has become one of the most commonly performed surgeries in recent decades, especially in patients with degenerative spondylolisthesis and disc-related diseases. 1,2 However, many studies have also reported complications, including implant failure, neurological injuries, vascular injuries, pseudoarthrosis, infection, and others 3 –5 due to instrumented spinal surgeries. Postoperative deep infection following instrumented spinal fusion is one of the most serious and difficult complications to manage. 6 It is widely agreed that surgical debridement combined with adequate antibiotics is essential for the treatment of these difficult cases. 7,8 Wide debridement with implant removal has proved be an effective method to treat postoperative infection after instrumented spinal fusion. 9 However, major spinal surgery consisting of removal of the implant and associated extensive debridement could result in further spinal instability or pseudoarthrosis. Hence, most surgeons agree that eliminating the infection while retaining the implant is an ideal management for patients with surgical site infection (SSI), especially in the early stage. 10
The diagnostic and therapeutic values of percutaneous endoscopic debridement and drainage (PEDD) for spinal infections has already been proved in recent studies. 11 –13 Yang et al. suggested the indications of this minimally invasive procedure could even be extended to treat patients suffering from spinal infections with paraspinal abscesses and postoperative recurrent infection. 14 However, all these studies focused on the effect of PEDD in spinal infection without implants. To date, no study has evaluated on the feasibility of this valuable technique in the treatment of patients with post-instrumented spinal infection. The purpose of the current investigation was to evaluate the efficacy of PEDD in the treatment of patients with SSI following instrumented lumbar fusion and to find the risk factors associated with the therapeutic results compared between patients with and without conversion of treatment method from PEDD procedures to open revision surgery.
Methods
Between January 2010 and December 2015, 20 patients with SSI following instrumented lumbar fusion were enrolled in this study. All 20 patients initially received decompression and associated reconstruction surgeries for degenerative spondylolisthesis and disc-related disease at our institute or other hospitals. The study was approved by the institutional review board, and informed consent was obtained from each patient. The case series included 6 women and 14 men with an average age of 60.1 years (range 38–72 years) who were treated with PEDD procedures at our institute, a 1200-bed tertiary referral center. SSI was diagnosed based on clinical examinations, including elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels, radiography, and magnetic resonance imaging findings. Patients who had spinal infections resulting in severe structural instability or deformity and who sustained significant neurological deficits were excluded. The medical records of the enrolled patients, including outpatient and emergency room notes, admission notes, inpatient progress and nursing notes, discharge summaries, surgical reports, radiology reports, pathology reports, and microbiology laboratory results, were reviewed. The microbiology reports comprised microscopy and culture findings and any specific pathogens identified by the PEDD procedures. All patients in this study had intractable back pain requiring narcotic pain control and bed rest before PEDD.
The terminal event was defined as a shift in the treatment method from PEDD procedures to an open revision surgery, with or without implant removal. We used several clinical parameters to identify the potential risk factors that could influence the terminal event, including age, sex, instrumented level, cage implantation, causative pathogens, pathogen detection, and chronic infection. Clinical outcomes were assessed by careful physical examination, regular serological testing, and imaging studies after PEDD to determine whether continued antibiotic treatment was sufficient or if open revision surgery was required. The visual analog scale (VAS), Oswestry disability index (ODI), and modified Brodsky criteria (MBC) were also used to examine clinical improvements in patients treated with PEDD procedures before surgery, after surgery, and at every follow-up visit.
PEDD technique
The patient was placed prone on a radiolucent frame suitable for fluoroscopy. All procedures were performed under local anesthesia with conscious sedation, similar to that used for standard lumbar discography. Conscious sedation was performed via administration of an intravenous bolus dose of fentanyl 50 μg and propofol 0.5 mg kg−1. Under fluoroscopic guidance, the target site was located and the entry site was marked on the skin at a point 8–12 cm from the midline. Following sterile preparation, draping, and administration of local anesthesia, a spinal needle was inserted directly into the targeted disc. The insertion trajectory was more horizontal than the usual approach to avoid the implant. A guide wire was introduced through the spinal needle into the area surrounding the disc space, and the spinal needle was then withdrawn. After creating a small stab-wound incision (approximately 1 cm), a dilator and a cannulated sleeve were guided over the wire and progressed sequentially into the center of the disc. Fluoroscopy was repeated in two orthogonal planes to verify the correct positioning of the endoscope tip. The tissue dilator was then removed and the cutting tool was inserted. The cutting tool, a cylindrical sleeve with a serrated edge at its distal end, was used to harvest a core of the impacted biopsy specimen. Discectomy forceps were then inserted through the cannulated sleeve to extract additional tissue from the infected disc. Percutaneous debridement was performed piecemeal by manipulating the biopsy forceps, flexible rongeurs, and shaver into different positions to obtain as much tissue as possible under fluoroscopic monitoring. The same procedures were repeated on the other side. These two working sheaths were left on both sides for sufficient extirpation and extensive debridement of the infected intervertebral disc and a portion of the end plate from a different endoscopic direction. Approximately 35 mL of povidone-iodine was diluted with 1000 mL normal saline to achieve a 3.5% betadine solution ready for use intraoperatively. After the biopsy and debridement procedures, at least 10,000 mL of the diluted betadine solution was used for irrigation. One portal was connected to a lavage fluid pump for the inflow and the other portal was connected to a suction bottle for the outflow with continuous infusion. The suction function was usually kept open from the beginning to the end of the procedure for further drainage of the lavage fluid and abscess. Finally, two large-bore drainage catheters were inserted into the debrided disc space and connected to a negative-pressure Hemovac. The biopsy specimen contained disc material and parts of the vertebral end plates of adjacent vertebrae. Each biopsy specimen was examined for microorganisms and evaluated histopathologically.
Statistical analysis
The Mann–Whitney U test or Fisher’s exact test was used to assess risk factors associated with the therapeutic results, compared between patients with versus patients without conversion of treatment method from PEDD procedures to open revision surgery. The clinical improvements in VAS, ODI, and MBC before surgery were compared with those after PEDD and every follow-up visit using the Wilcoxon signed-rank test. Nonparametric statistics were used, as several variables were not normally distributed. The SPSS 13.0 software (SPSS Inc., Chicago, Illinois, USA) was used for data analysis. A value of p < 0.05 was considered statistically significant.
Results
Among the 20 enrolled patients, 13 (65%) were successfully treated by PEDD and appropriate antibiotic therapy (Figures 1 to 4). The terminal event included seven patients whose spinal infection was not under control and underwent open revision surgeries, five patients with implant removal, and two patients with retainment of implant following extensive debridement procedures. Causative bacteria was identified in the biopsy specimens of 17 (85%) patients. The spinal infections of nine patients were caused by Staphylococcus aureus, including five infections due to the oxacillin-sensitive strain and four due to the oxacillin-resistant strain. Four patients had infections caused by Mycobacterium tuberculosis, two had infections caused by Pseudomonas aeruginosa, and two had infections caused by Streptococcus viridans and Escherichia coli (Table 1). Pathogen detection was the only risk factor (p < 0.05) that influenced the terminal event (Table 2). The most prominent clinical sign of spinal infection was back pain, which occurred in all 20 patients before PEDD. One week after PEDD, most patients reported satisfactory relief of their back pain. Seven patients with persistent infection and severe back pain underwent extensive debridement procedures with or without implant removal within 3 months after PEDD. An at least 6-week course of systemic parenteral antibiotics or full-course antimicrobial chemotherapy were administered, based on the sensitivity studies for the identified pathogens. Overall, the 13 patients successfully treated with PEDD and appropriate antibiotic therapy were satisfied with the clinical results. Both VAS and ODI significantly improved after PEDD treatment in these patients (Table 3). The elevated CRP levels normalized within a mean of 5 weeks, while the ESR levels decreased irregularly to half of the original pretreatment values within a mean of 3 weeks (Figure 5). No recurrent infection was found among these patients during at least 24 months’ follow-up (average 38.9 months; range 28–72 months). No patient experienced PEDD-related complications such as neural injury.

A 54-year-old female underwent L4-S1 instrumented fusion several years prior and complained of severe low back pain and intermittent high fever. Radiograph showed L4 and S1 pedicle screw loosening and L4–S1 end plate erosion.

Sagittal and axial T2-weighted magnetic resonance imaging demonstrated L4–S1 infection with paraspinal abscess accumulation.

After percutaneous endoscopic debridement and drainage, a negative pressure Hemovac with two drainage tubes was inserted into the L4–S1 disc space for further continuous drainage of the causative pathogens.
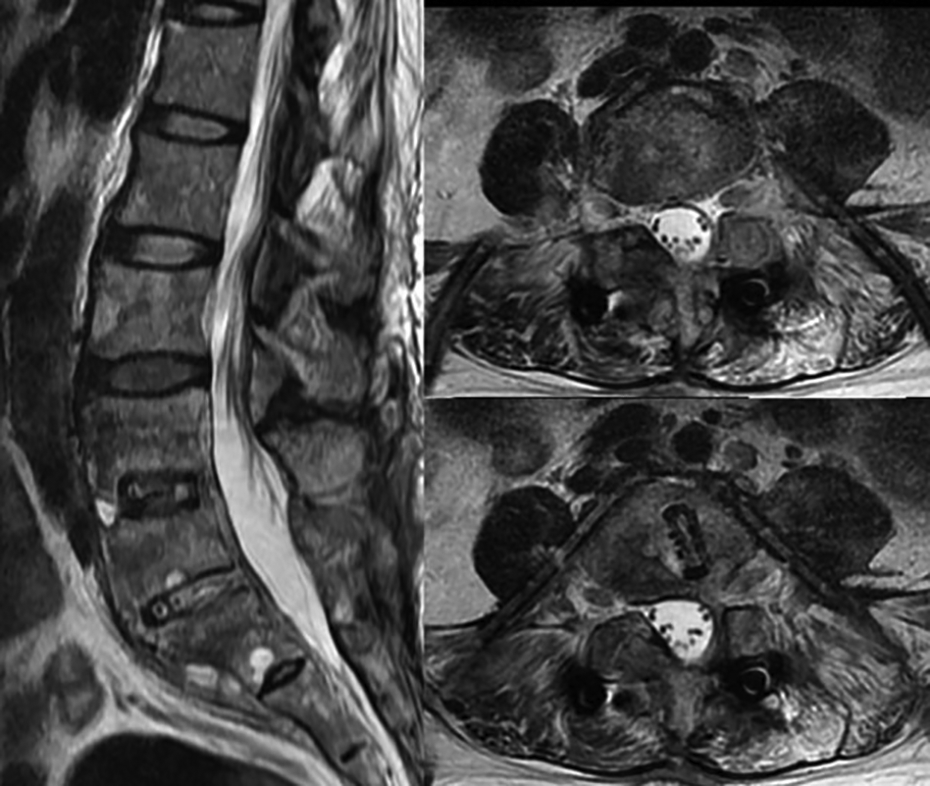
Postoperative magnetic resonance imaging revealed decreased paraspinal abscesses and two inserted drainage tubes for continuous drainage.
Patient demographic data.

M: male; F, female; T: thoracic spine; L: lumbar spine; S: sacral spine; OSSA: oxacillin-sensitive Staphylococcus aureus; ORSA: oxacillin-resistant Staphylococcus aureus; MT: Mycobacterium tuberculosis; AIDS: acquired immune deficiency syndrome.
a Chronic infection.
b AIDS.
Comparison of clinical findings between the patients with or without shifting to open surgery.
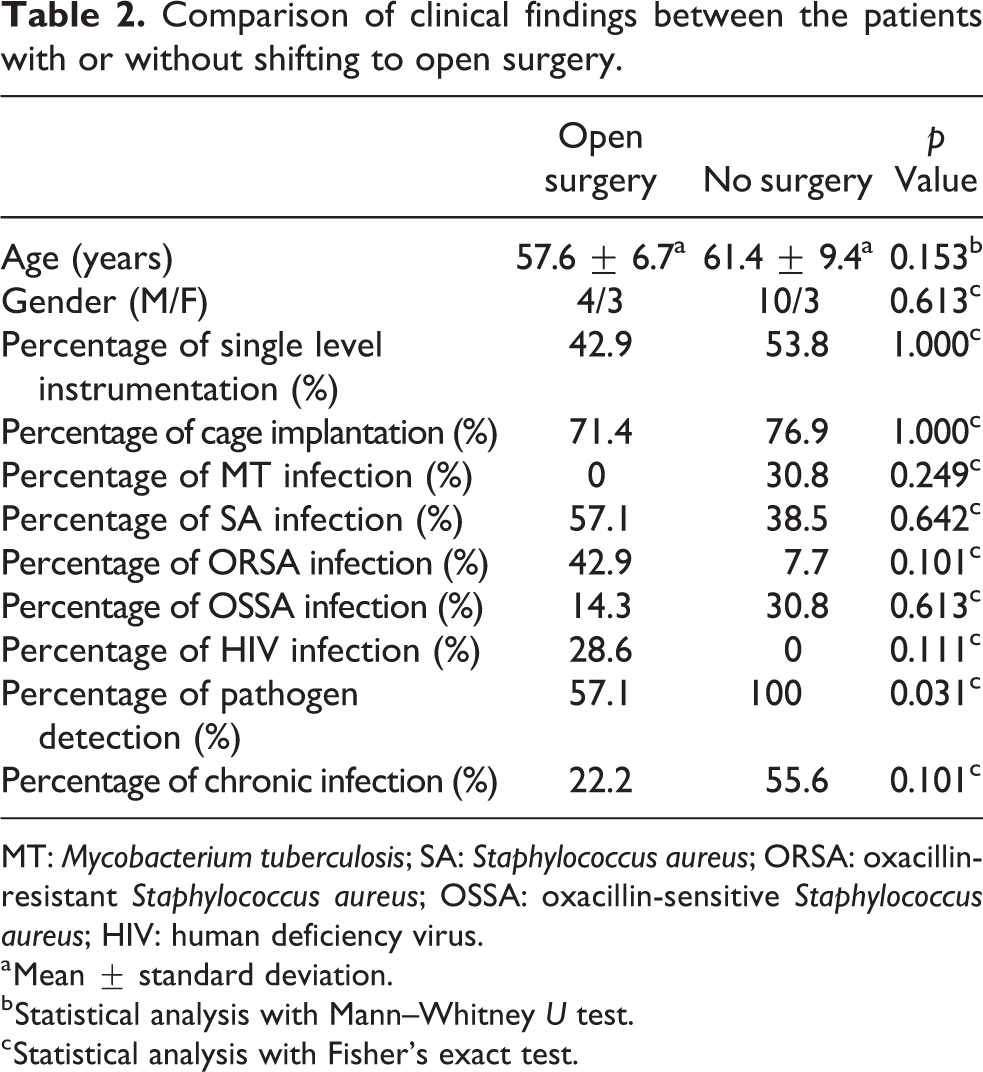
MT: Mycobacterium tuberculosis; SA: Staphylococcus aureus; ORSA: oxacillin-resistant Staphylococcus aureus; OSSA: oxacillin-sensitive Staphylococcus aureus; HIV: human deficiency virus.
a Mean ± standard deviation.
b Statistical analysis with Mann–Whitney U test.
c Statistical analysis with Fisher’s exact test.
Comparison of clinical outcomes before surgery and after surgery.
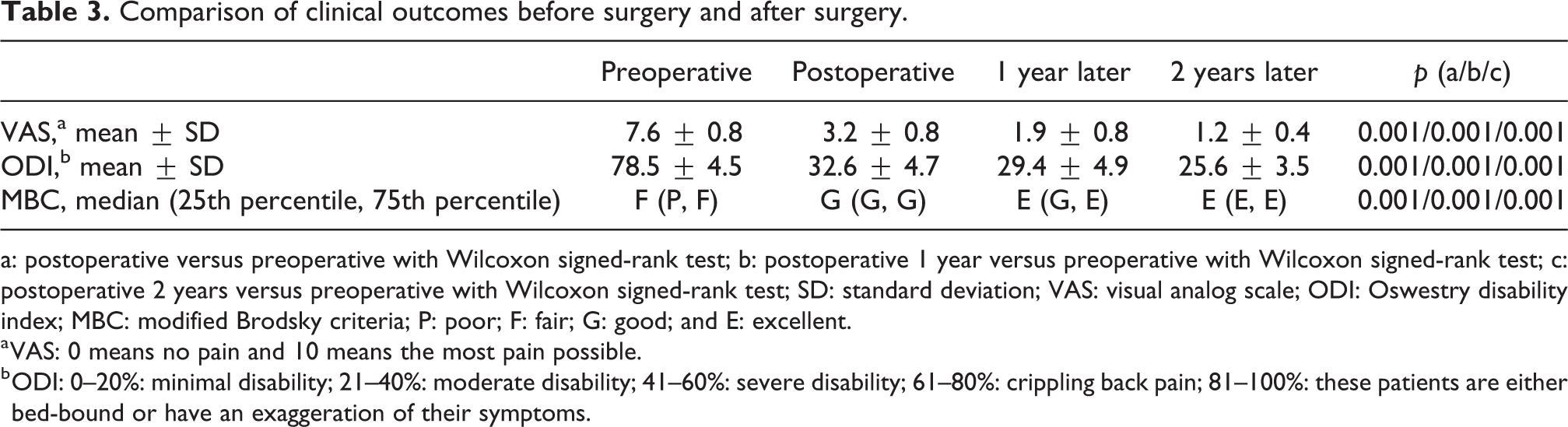
a: postoperative versus preoperative with Wilcoxon signed-rank test; b: postoperative 1 year versus preoperative with Wilcoxon signed-rank test; c: postoperative 2 years versus preoperative with Wilcoxon signed-rank test; SD: standard deviation; VAS: visual analog scale; ODI: Oswestry disability index; MBC: modified Brodsky criteria; P: poor; F: fair; G: good; and E: excellent.
a VAS: 0 means no pain and 10 means the most pain possible.
b ODI: 0–20%: minimal disability; 21–40%: moderate disability; 41–60%: severe disability; 61–80%: crippling back pain; 81–100%: these patients are either bed-bound or have an exaggeration of their symptoms.

Percentage change in serological values ((a) ESR and (b) CRP), before and after percutaneous endoscopic debridement and drainage, in successfully treated patients.
Discussion
Deep SSI after spinal surgery is a serious complication, with a reported incidence rate of 1.9–20%. 15,16 There is still no consensus concerning the treatment strategy for these difficult cases. Although surgical debridement is crucial, controversy remains with regard to which procedure should be selected and whether the previously implanted instrument should be removed or retained. Removal of implants could increase the chance of infection eradication as it eliminates biofilm-related microorganisms. Kim et al. performed implant removal and wide debridement for 21 patients with postoperative deep wound infection, resulting in good clinical outcome. 9 However, subsequent spinal instability and pseudoarthrosis may be a major concern after this procedure. Many surgeons recommend that most post-instrumented spinal infection could be controlled by aggressive debridement, appropriate antibiotic therapy, and retention of implants. 17,18 Although major spinal surgery can successfully treat deep infection, it is associated with postoperative complications in this fragile population. 19,20
In our case series, 20 patients with SSI following instrumented lumbar fusion were enrolled. Thirteen patients were treated successfully with PEDD and antibiotic therapy. The remaining seven patients required open surgery with or without implant removal to cure the spinal infection. The success rate was only 65%, which was lower compared with open surgery. Maruo and Berven treated 126 postoperative SSI cases with aggressive debridement and implant retention 21 ; 43 (22%) cases developed treatment failure, with 5 cases resulting in death. It is difficult to achieve extensive debridement through PEDD. However, there were no PEDD-related complications in our case series. In consideration of the low complication rate, simplicity, minimal invasiveness, and acceptable successful rate, PEDD could be regarded as an effective alternative treatment for these patients.
The diagnosis and treatment of spinal infection remains a challenge to clinicians due to its early, subtle clinical course. A high degree of suspicion is crucial to achieve a timely and accurate diagnosis and avoid severe complications due to inadequate or delayed management. Prescribing specific antibiotics targeted against the causative pathogen plays an important role. Hence, identifying the causative pathogens is one of the key factors required to achieve cure in these patients. Computed tomography-guided biopsy has been recommended to determine the causative pathogen, with variable success rates. However, the aspirate is often inadequate due to insufficient specimen harvesting. Fouquet et al. retrospectively reviewed 25 cases of postoperative discitis and obtained bacteriological diagnosis in only nine (36%) patients. 22 Rankine et al. analyzed 20 patients who underwent spinal biopsy and found that a causative organism could be isolated in only 6 of the 12 patients not receiving antibiotics and 2 of the 8 patients receiving antibiotics. 23 Through the PEDD technique, we harvested sufficient specimens from various infected disc regions for microorganism examination, which could provide a better diagnostic rate. In our previous study, which retrospectively reviewed 20 patients who underwent percutaneous endoscopic discectomy and drainage, we could identify the causative bacteria in 18 (90%) of 20 patients. 24 Appropriate antibiotics for the pathogen were prescribed, and good clinical outcomes were reported. In the current study, the causative bacteria were identified in the biopsy specimens of 17 (85%) of 20 patients. Among these 17 patients, only four (23.5%) required additional open surgery due to PEDD treatment failure. We also found that pathogen detection is the only risk factor (p < 0.05) that influenced the terminal event. Therefore, PEDD-assisted treatment and appropriate antibiotic therapy based on the causative pathogen is crucial and can lead to good clinical results.
An epidural abscess is a rare but potentially devastating infection of the central nervous system. 25 Abscesses that are enclosed within the bony confines of the spinal column can compress the spinal cord and cause severe neurological symptoms. The treatment usually requires a combination of surgical decompression and appropriate antibiotics. Yang et al. retrospectively reviewed the medical records of 10 patients with paraspinal abscess which included subdural abscess, presacral abscess, and perivertebral psoas muscle abscess. All the patients underwent percutaneous endoscopic lavage and drainage treatment, and all of them were successfully treated. 14 Hence, this minimally invasive technique could be a valuable alternative choice for these difficult cases.
The current study has several limitations. First, the retrospective nature of the study design lacked randomization of patients. Therefore, it was not possible for enrolled patients to undergo different treatment methods for subsequent comparison of clinical outcomes. Due to the absence of a control group, it is difficult to validate that the treatment effect is not due to antibiotic therapy. The feasibility and benefits of PEDD for the treatment of SSI after lumbar instrumented fusion should thus be rigorously evaluated in a large patient population with prospectively controlled comparison groups. Second, the authors only examined 20 patients with similar clinical conditions, and several clinical-related parameters were used to identify potential risk factors. Pathogen detection was found to be the only risk factor that influenced the terminal event in this small patient population. More patients with different potential parameters should be included to increase the statistical power. Third, most patients with spine infection are fragile, with comorbidities that include hypertension, diabetes mellitus, coronary artery disease, rheumatic disease, late stage renal disease, or other degenerative disorders. We did not take these comorbidities into consideration because they have no direct correlation with spine infection. However, all these comorbidities may influence the immune system and treatment results. Finally, several of the enrolled patients with SSI had received different types of antibiotic treatment before being transferred to our institute owing to previous treatment failure and/or progressive infection at their original hospital. The use of antibiotics prior to PEDD surgery may have interfered with the detection of offending pathogens.
Conclusions
Based on the current analytical findings, PEDD is an effective minimally invasive method for obtaining a bacteriological diagnosis, relieving patients’ symptoms, and assisting in eradication of SSI following instrumented lumbar fusion. Antibiotics targeted toward the causative pathogen appears to be the most important factor to determine the success rate of treatment. The indications of this minimally invasive procedure could be extended and used as an alternative before major open surgery for the treatment of patients with SSI after instrumented lumbar fusion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.