
Abstract
Study Design
Retrospective cohort study.
Objective
Although surgical risk factors for developing spine surgical site infections (S-SSI) have been identified, the impact of such knowledge in its prevention has not been demonstrated.
Methods
We evaluated in 500 patients undergoing spine surgery between 2011 and 2019 at Hospital 12 de Octubre the changes in S-SSI rates over time. Surgical variables independently related to S-SSI were analyzed by univariate and multivariate analysis using binary logistic regression models. A case-control sub-analysis (1:4), matched by the surgical variables identified in the overall cohort was also performed.
Results
Twenty cases of S-SSI were identified (4%), with a significant decrease in the incidence rate across consecutive time periods (6.6% [2011-2014] vs .86% [2015-2019]; P-value <.0001)). Multivariate analysis identified arthrodesis involving sacral levels (odds ratio [OR]: 2.57; 95% confidence interval [95%CI]: 1.02-6.47; P-value = .044) and instrumentation over 4-8 vertebrae (OR: 2.82; 95%CI: 1.1-7.1; P-value = .027) as independent risk factors for S-SSI. The reduction in the incidence of S-SSI concurred temporally with a reduction in instrumentations involving 4-8 vertebrae (55% vs 21.8%; P-value <.0001) and sacral vertebrae (46.9% vs 24.6%; P-value <.0001) across both periods. The case-control analysis matched by these surgical variables failed to identify other factors independently related to the occurrence of S-SSI.
Conclusions
Spinal fusion of more than 4 levels and the inclusion of sacral levels were independently related to the risk of S-SSI. Optimization of surgical techniques by reducing these two types of instrumentation could significantly reduce S-SSI rates.
Introduction
Spinal Surgical site infection (S-SSI) occurs in .7% to 12.0% of patients undergoing spinal surgery1,2 and is related with increased morbidity, mortality and a 4-fold increase in health care costs, even if the surgery is ultimately considered successful1.
Several retrospective studies have identified different risk factors for this S-SSI, mostly related with the surgical technique and, to a lesser extent, patient-related characteristics.1,3-8 Nevertheless, the real impact of this increasing knowledge in terms of preventive measures for this complication has not been yet analyzed.
Since we began to prospectively register and follow-up cases of S-SSI in instrumented spine surgeries at our center in 2011, we initially observed a relatively high incidence that has progressively declined in the latest years.
The aim of our study was to analyze the epidemiological and etiological evolution of S-SSI at our institution and to evaluate the factors that could have influenced this reduction.
Materials and Methods
Study Population and Design
This retrospective study was conducted at the University Hospital “12 de Octubre” (Madrid, Spain). The Clinical Research Ethics Committee approved the study protocol (2020/0215) and granted a waiver of informed consent in view of the observational design. The research was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Patients eligible for the study were all those that had undergone spinal instrumentation in our Neurosurgery Department during the study period (January 2011 to December 2019). The design was a retrospective cohort study complemented by a nested case-control study with matching. Beginning in January 2011, affiliation data and main surgical variables of the study cohort had been prospectively collected in a healthcare database maintained by the Neurosurgery Department. Collected variables included preoperative diagnosis, type of procedure (arthrodesis, re-arthrodesis, adjacent segment fusion and others), number of vertebrae and spaces involved in vertebral fixation, whether it was open or minimally invasive surgery (MIS), and the level of the spine operated on; and others, such as the use of a lumbar interbody cage and the need for readmission and re-operation of the patient after wound infection. The main post-surgical complications occurring in the first 3 months after surgery, including S-SSI were also included in the database.
The diagnosis of S-SSI was made applying the criteria for superficial and deep incisional surgical site infection of the Centers for Disease Control and Prevention (CDC) (see definitions below), and confirmed after retrospective evaluation revision of the medical records by two authors (JDF, IP) of the Neurosurgical Department.
For the nested case-matched control study, four controls were randomly selected from the cohort per case, matched by year of intervention and by the surgical variables identified in the overall risk factor analysis of the cohort. A study-specific database was designed to include patient comorbidity variables as well as surgical variables not included in the healthcare protocol. It included patient-dependent data: Charlson comorbidity index: myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic lung disease, connective tissue pathology, ulcer disease, mild liver pathology, moderate or severe liver pathology, diabetes, diabetes with organ damage, hemiplegia, moderate or severe renal pathology, malignancy, leukaemias, lymphomas, solid metastases and AIDS; as well as the use of immunosuppressive medication, body mass index (BMI) > 35, pre-surgical risk attributed by the American Society of Anesthesiologists (ASA) scale, and the existence of urinary or faecal incontinence. In addition, other surgery-dependent factors were included, evaluating if this surgery had been performed on a previous operated area; approach way used (anterior or posterior), level of surgery, and number of vertebral spaces involved; duration of surgery (greater than 3 hours); use of hydroxyapatite chips, bone chips or bone grafts; and finally, type of antibiotic prophylaxis, including intraoperative use of vancomycin powder in the surgical bed.
Preventive Measures Against Surgical Site Infection
Preparation of the patient’s skin in the operating theatre included total body preoperative shower and surgical site antisepsis with chlorhexidine soap. Pre-operative hair removal was performed immediately before the procedure with clippers. Antibiotic prophylaxis protocol included intravenous (IV) cefazolin (2 g) in the induction of anesthesia or IV vancomycin (1g) for allergic patients.
Definitions
Criteria for definition of S-SSI case: Cases fulfilling deep surgical site infection according to CDC criteria 9 occurring up to 90 days after surgery: involving deep planes of tissue (fascia or muscle) and meeting at least one of the following criteria: (a) purulent drainage through the incision; (b) spontaneous wound dehiscence or that is deliberately opened by a surgeon, with identification of microorganisms in wound cultures and patient symptoms consisting of at least one of the following: fever (temperature greater than 38°C), increased tenderness or pain; (c) demonstration of the existence of an abscess or other evidence of deep-plane infection, either by imaging tests, direct vision or histopathological examination.
Controls: Patients from the spine surgery cohort without SSSI data and matched to each case by year of surgery and by independent surgical factors detected in the overall cohort analysis were included.
Statistical Analysis
Quantitative data were shown as the mean ± SD or the median with interquartile range (IQR). Qualitative variables were expressed as absolute and relative frequencies. Categorical variables were compared using the χ2 test. Student’s t-test or Mann-Whitney U test were applied for continuous variables, as appropriate.
Factors associated with the occurrence of S-SSI were investigated either in the global cohort or in the case matched control sample through univariate and multivariate comparative analyses through logistic regression models. Those variables with univariate P-values ≤.1 were entered into a backward stepwise logistic regression model. Multicollinearity among explanatory variables was analyzed using the variance inflation factor (VIF), with VIF values <3 being considered acceptable. The most parsimonious model (i.e. the highest outcome variability explained with the lowest number of variables) was selected. Results were given as odds ratios (ORs) with 95% confidence intervals (CIs).
For the selection of controls within the global cohort, each patient was firstly codified regarding the presence or not of the surgical risk factors obtained in the analysis of the global cohort. For each case, four controls were randomly selected from all the patients without S-SSI from the global cohort with the same codification regarding surgical factors and the same year of surgery.
All the significance tests were two-tailed. The threshold for significance was set at a P-value <0·05. Statistical analysis was performed with SPSS version 21.0 (IBM Corp, Armonk, NY).
Results
Incidence and Description of Cases of IASI
During the overall study period (2011-2019), 500 surgical spine interventions were performed at the Neurosurgery Department of our center, and 20 of them (4%) met the criteria for S-SSI. As is represented in Figure 1, in the period between 2011-2015, 18 cases of S-SSI were recorded in 270 procedures (6.6%), compared with only 2 cases in 230 procedures (.86%) in the period 2016-2019, with statistically significant differences (P-value: <.0001). Graphical representation of the evolution of annual S-SSI incidence (in black) and the number of spine surgeries (in grey) from 2011 to 2019.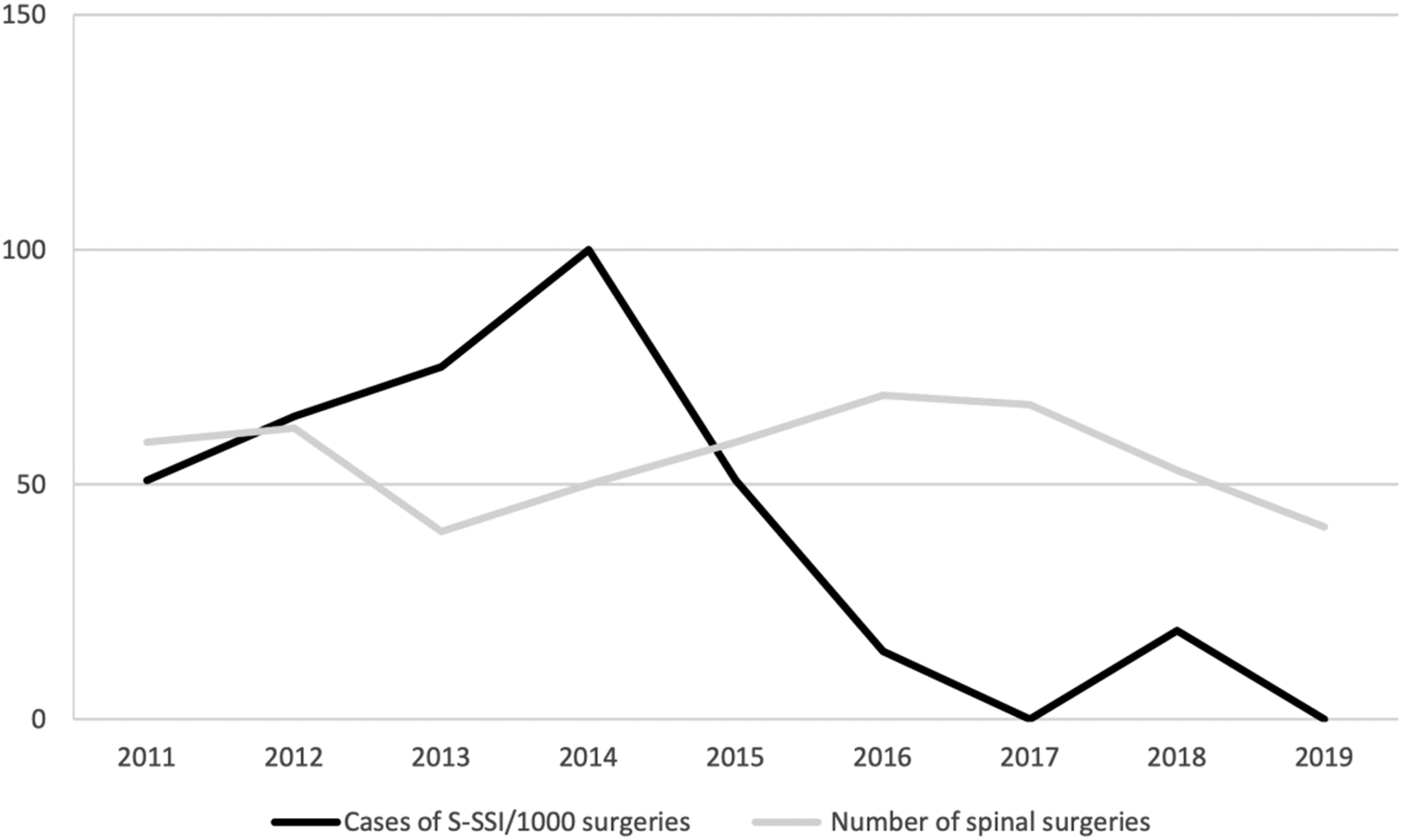
Description of the 20 episodes of S-SSI 2011-2019.
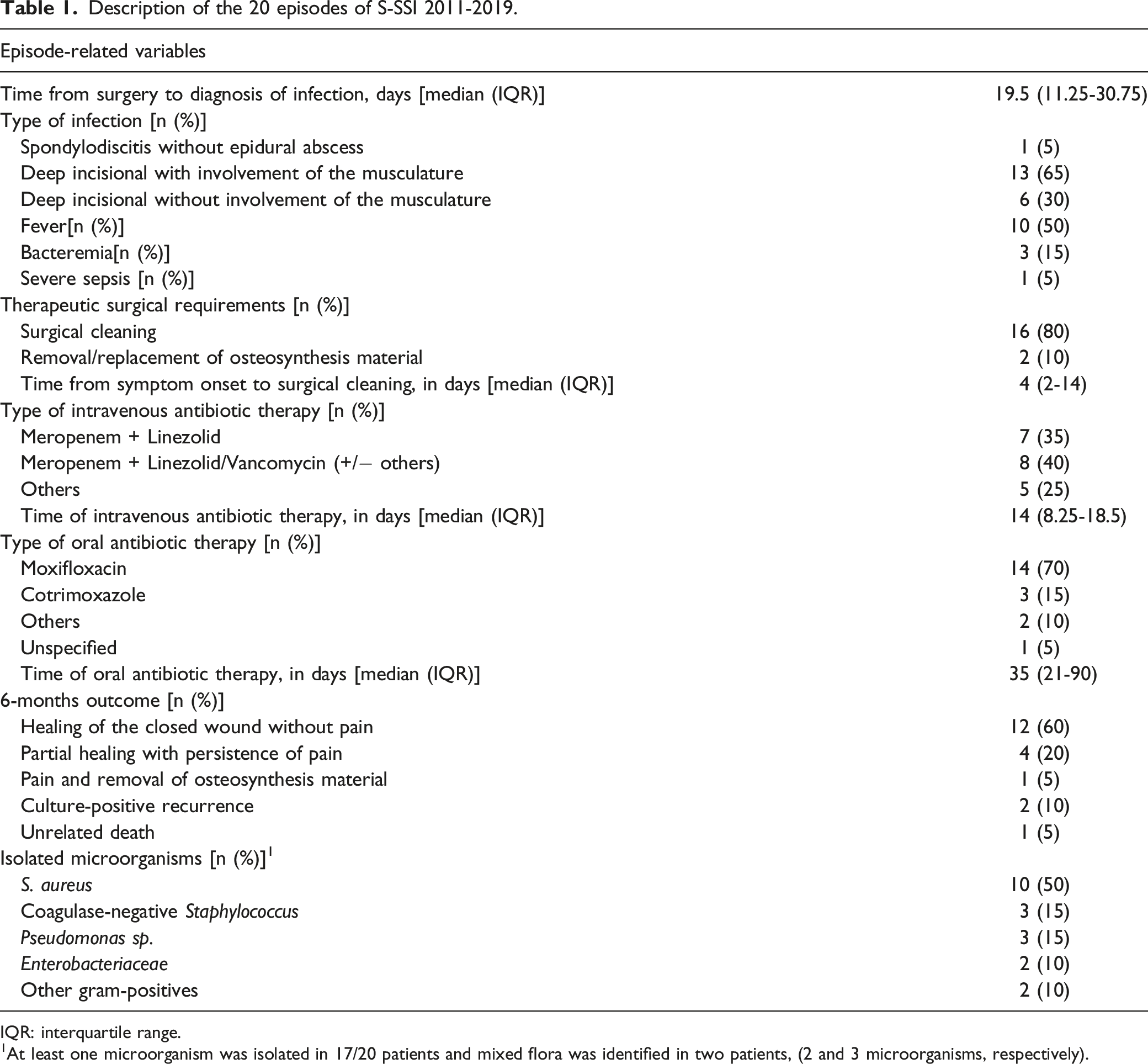
IQR: interquartile range.
1At least one microorganism was isolated in 17/20 patients and mixed flora was identified in two patients, (2 and 3 microorganisms, respectively).
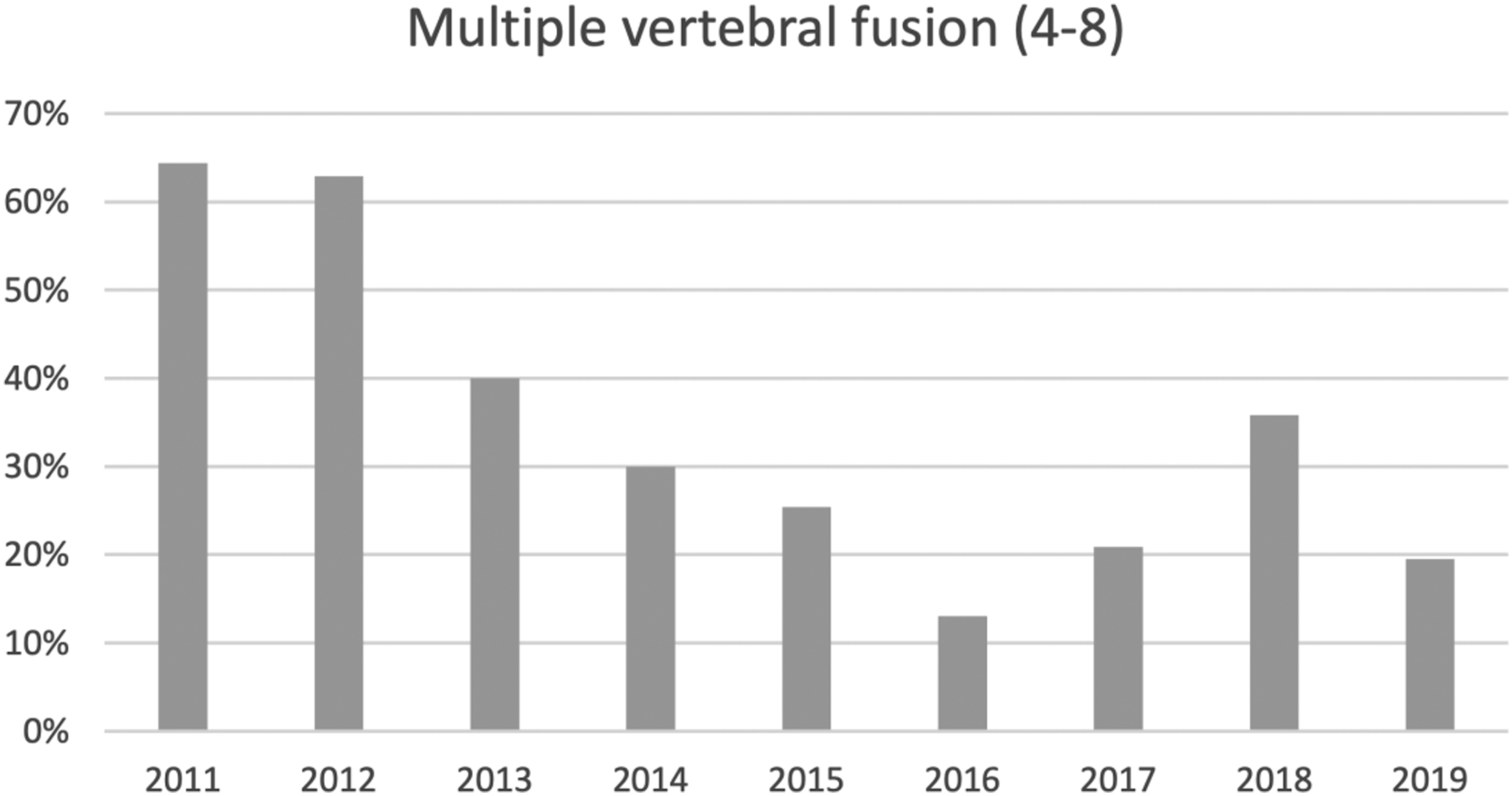
Graphical representation of the annual percentage of spinal surgeries consisting of multiple vertebral fusion (4-8) from 2011 to 2019.
Six months after S-SSI diagnosis, 60% of the patients presented clinical cure with absence of pain and healed wound. In contrast, 20% of patients showed only partial healing, with persistent pain during follow-up. Only one patient (5%) required removal of the osteosynthesis material. In two cases (10%), recurrence of infection was detected with newly positive cultures, requiring readmission for intravenous antibiotic therapy. In one single patient death non-attributable to S-SSI was reported Figure 3.
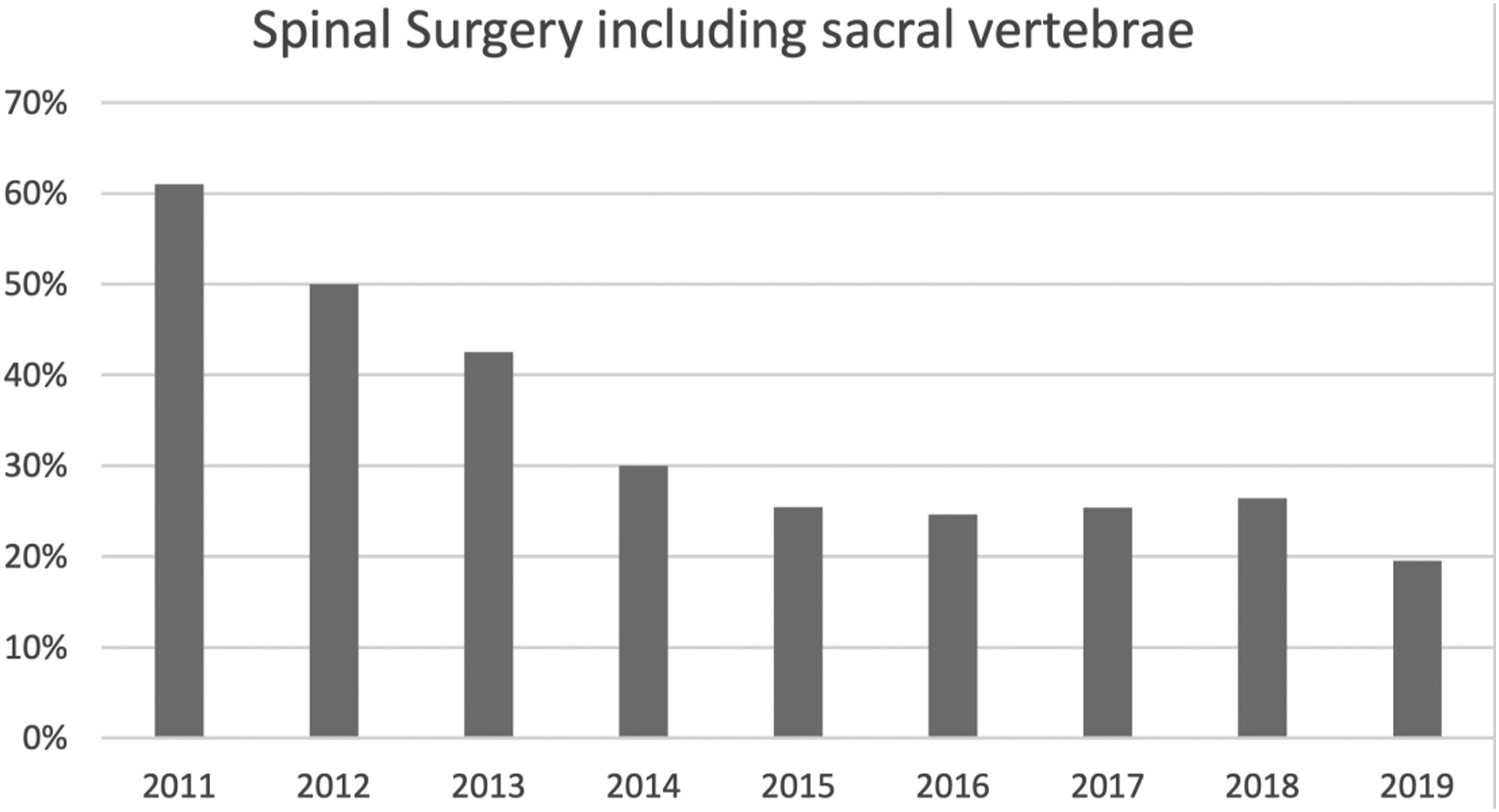
Graphical representation of the annual percentage of spinal surgeries including sacral vertebrae from 2011 to 2019.
Surgical risk factors for surgical site infection in the global cohort
Comparison of demographic and surgical variables in patients developing or not developing S-SSI in the overall cohort (2010-2019).
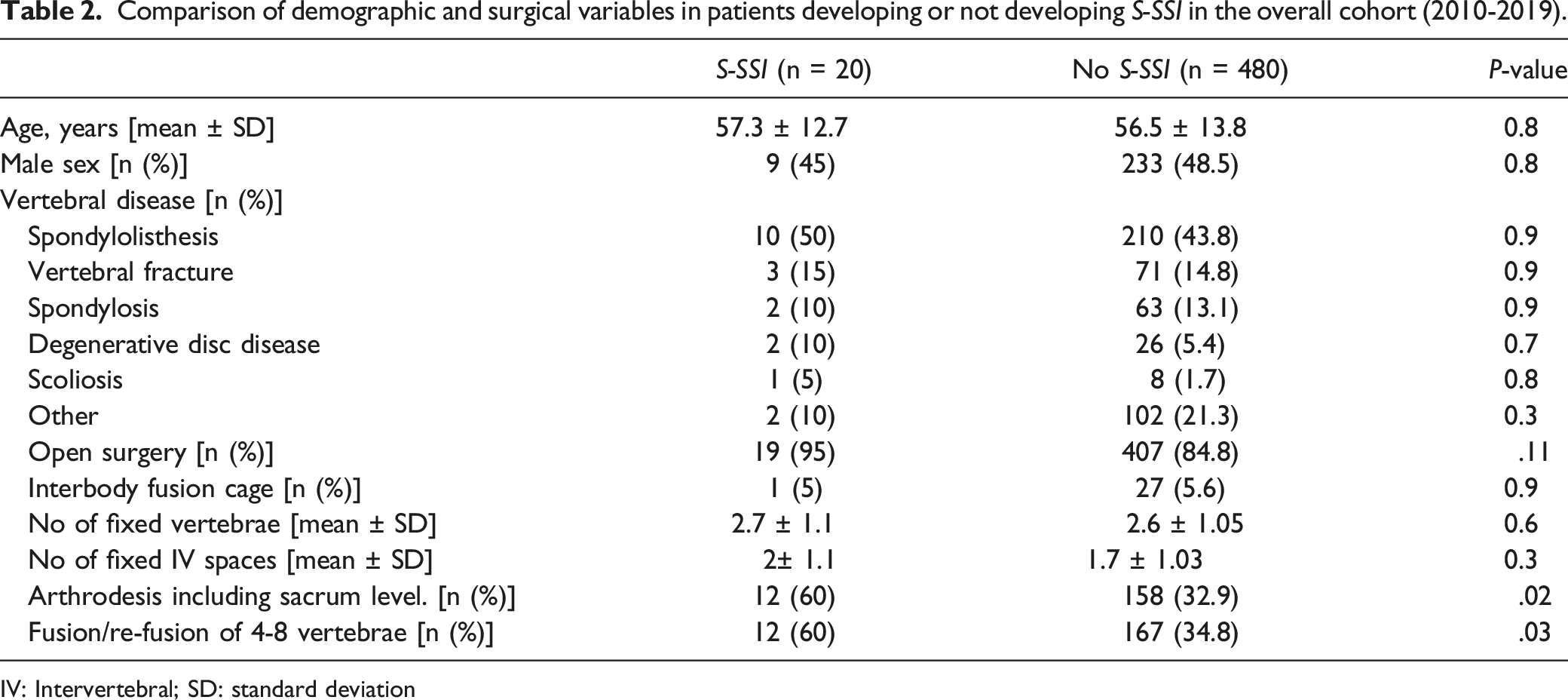
IV: Intervertebral; SD: standard deviation
Univariate and multivariate analysis of surgical risk factors for S-SSI in the overall cohort (2011-2019).

CI: confidence Interval; OR: odds ratio
Comparison of the number of interventions on sacral levels and refusions of 4 to 8 vertebrae between the periods 2011-2014 and 2015-2019.

Risk factors for surgical site infection: Nested case-control study matched by surgical variables
Comparison of demographic and surgical variables in cases of IAIV and matched controls* (1:4).
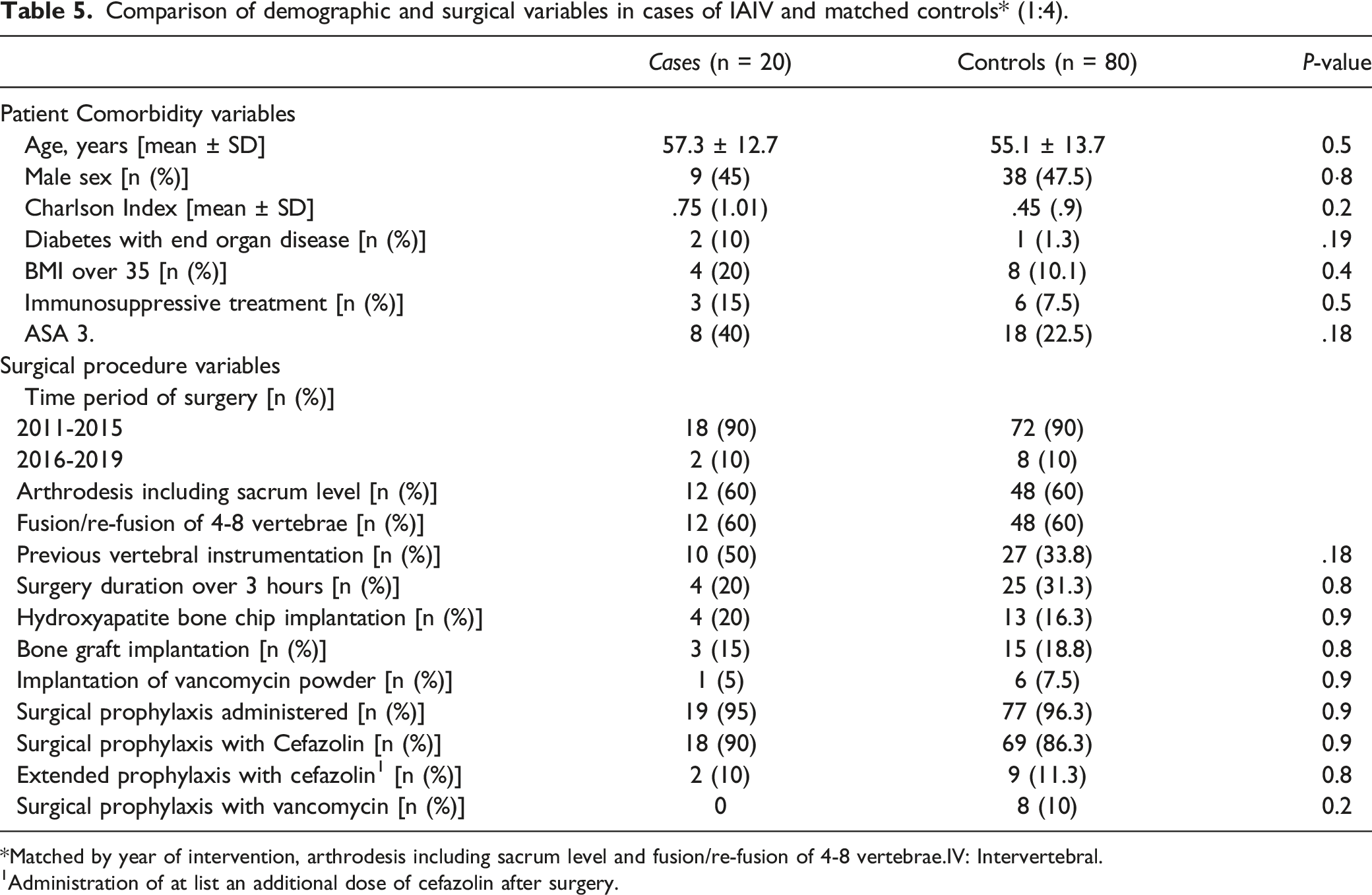
*Matched by year of intervention, arthrodesis including sacrum level and fusion/re-fusion of 4-8 vertebrae.IV: Intervertebral.
1Administration of at list an additional dose of cefazolin after surgery.
Discussion
After observing an apparent reduction in the number of patients with S-SSI in recent years in patients undergoing spinal surgery in our hospital in the period 2011-2019, we decided to analyze what factors could be positively influencing this trend. We first confirmed in our cohort a significant decrease in the incidence of infection S-SSI from rates above 6% in 2011 to current rates below 1%, even lower than the incidence (around 5%) described in other series.1,2 The analysis of surgical risk factors for S-SSI demonstrated that some specific spinal surgeries posed an increased risk for this complication. We observed that the yearly reduction on such high-risk interventions was coincidental with a progressive waning in the incidence of S-SSI over time. A greater number of vertebrae involved in the fusion technique3,5,10 and extension of the fusion to the sacrum or pelvis3,6 have been considered procedures of high risk for infection, independently to the duration of the surgery. 5 After adjustment for these main surgical variables, we investigated in a matched nested case-control study other intra-surgical variables potentially related to infection that could have varied over time, such as the use of intersomatic cages, bone graft, or bone substitute chips for spinal fusions and arthrodesis, or the use of vancomycin powder in the surgical bed. The type of material used for arthrodesis was not found to influence the risk of infection, in line with the data found in other studies. 11 The use of local vancomycin complementary to antibiotic systemic prophylaxis is a strategy that has been progressively implemented in spinal surgery, although there are conflicting data about its efficacy in preventing S-SSI.12-16 Local vancomycin was used in 7% of the spinal surgeries. We could not find any preventive effect of S-SSI in our series. Its limited use preclude us from extracting definitive results on the efficacy of local vancomycin in the prevention of S-SSI.. Probably also due to the relatively small number of cases included we could only detect statistically non-significant trends in the risk effect of some patient-dependent preoperative variables previously recognized as risk factors for SSI as diabetes mellitus1,4,8,10 high BMI values5,8,17,18 or pre-anesthetic ASA III classification.8,10,15
The characteristics of the patients in our series are similar to those described in other series. Infection by S. aureus was the most common causative agent.18,19 Most of patients evolved favorably with a strategy that included surgical cleaning and intravenous antibiotic therapy, followed by prolonged oral therapy. Sixty per cent of patients were cured at six months and only 10% required removal of implant. There is scarce reported information regarding success of treatments, including retention of implant, in S-SSI. Healing rates with conservation of the osteosynthesis material in osteoarticular infections are variable and range from 50-100%. 20 Early cleansing surgery at a median of 4 days from the onset of symptoms, which has been associated with a better outcome, 21 was probably one of the keys to the success of the treatment in our series On the other hand, antibiotic therapy consisted on relatively short IV regimens, with a median of 2 weeks compared to the long regimens of 4-6 weeks used in other series.19,21,22 Oral antibiotic therapy was prolonged a median of 2 months and included primarily anti-staphylococcal quinolones, such as moxifloxacin, without requiring concomitant rifampicin. Although this regimen has shown to be safe and effective in staphylococcal infections associated with orthopedic implants, 23 the evidence in S-SSI is more limited and our data would support its use in this indication.
We have to recognize several limitations in this study. Despite the adjustment through matching by surgical variables and 1:4 case-control design, the limited number of S-SSI episodes prevented us from performing a more powerful study. Therefore, only trends could be detected for some variables potentially related with a higher risk of S-SSI. On the other hand, the follow-up of 3 months could underestimate some late-onset infections, although it is assumed that late S-SSI represents a minority of cases. Although late-onset infections could have been more probably reported in the first period in which patients had a longer follow-up we believe that it is improbable that differences between both periods on S-SSI analyzed in the present study could be attributable to different follow-up.
The reasons for restricting long constructs and complex fusion procedures were not specifically documented in the present study. Concerns over the damage to the soft tissues and uncertainty on the surgical results of long fixations from our experience and others 24 have probably driven the neurosurgeon’s trend towards shorter arthrodesis over time. That goes hand by hand with involvement of the sacral vertebrae, since long fusions are linked to biomechanical issues that favor the extension of the hardware to the sacrum. Finally, as readjustment of surgical techniques were not performed through the implementation of an optimization protocol we could not design a more specific study as interrupted time-series for evaluating the real impact of such preventive intervention in the observed reduction of S-SSI over time in our institution.
In conclusion, a greater number of vertebral levels operated and instrumentations including sacral levels were associated in our study with a higher risk of postoperative infection. Optimization of the surgical techniques in spinal surgeries could have contributed to the reduction of S-SSI over time in our series. In view of the results of the present study, although biomechanical stability should be the main criteria, potential risk of infection could be an additional factor to be considered previously to decide the extension of fusion procedures.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Conceptualization: Rafael San-Juan, Igor Paredes; Methodology: Rafael San-Juan, Igor Paredes; Data collection: Esther Ramírez-Nava, Juan Delgado-Fernández, Irene Panero, Paula Hernández-Ortiz, Elia Ramírez-Vicente; Formal analysis and investigation: Rafael San-Juan, Igor Paredes. The first draft of the manuscript was written by Rafael San-Juan and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.F.R. holds a research contract “Miguel Servet” (CP18/00073) from the Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation.
Ethical Approval
Ethical approval was waived by the local Ethics Committee of University A in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.