
Abstract
We report a case of sacral fracture complicated by an intrasacral meningocele in a 37-year-old male. The patient had a left sacral fracture with bilateral fractures of the superior and inferior pubic rami. The sacrum was fixed with a posterior plate and both superior pubic rami were fixed with an intramedullary screw. However, computed tomography myelogram and magnetic resonance imaging showed the intrasacral meningocele with the leakage of the cerebrospinal fluid into the buttocks and developed delayed union. Reoperation utilizing a strong anterior and posterior internal fixation combined with posterior bone grafting was undertaken and bone union was obtained.
Introduction
An intrasacral meningocele is a rare form of sacral cyst that was first reported in 1932 by Enderle. 1 Since then, intrasacral meningocele was reported by several reports and defined as that the walls are composed of fibrous tissue and the cavity is lined with an arachnoid membrane. This cyst filled with cerebrospinal fluid (CSF), including no neural component within the confines of the sacrum. 2,3 For many of the patients, intrasacral meningocele is asymptomatic, and they are often found by chance in diagnostic imaging. 4 Therefore, in many cases, the patients are not aware that they have the intrasacral meningocele.
There has been only one case reporting an intrasacral meningocele complicated by a fracture treated conservatively. 5 An intrasacral meningocele with a fracture is extremely rare, so the treatment methods or pitfalls are unclear. We report a rare case of unstable pelvic ring fracture complicated by an intrasacral meningocele. We emphasize the importance of knowing the pathology of an intrasacral meningocele and strong fixation is required for sacral fracture accompanied by bone graft to ensure union.
Case presentation
The patient was a 37-year-old male who was hit by a log 60 cm in diameter fell onto his back from 2 m height. The physical findings consisted of pain in the lumbar area, but there were no other clinical manifestations. Radiographs at the time of the injury revealed a sacral fracture through the left sacral foramina and bilateral laminae with bilateral fractures of the superior and inferior pubic rami (Figure 1(a)). The left side of the pelvis was displaced superiorly, and it was an AO classification C1.3 vertical shear-type fracture. Computed tomography (CT) scans showed a sacral zone II comminuted fracture and widening of both the spinal canal and the sacral foramen (Figure 1(b)). On the day of the injury, external fixation was applied. On the third day after the injury, the sacrum was fixed with a posterior plate inserted through the bilateral longitudinal incision to bridge the fracture with minimal invasion and both superior pubic rami were fixed with an intramedullary screw (Figure 2). Perfect reduction could not be obtained, which caused the insufficient length of the superior pubic ramus intramedullary screw. The location of the superior ramus screw within the bone was confirmed by postoperative CT scan. One month postoperatively, subcutaneous fluctuation was observed in the buttocks. CT scan was obtained and percutaneous needle aspiration at the same time confirmed the CSF leakage. We continued observation as there was no migration of the fracture. However, radiology at 3 months revealed cranial displacement of the left hemipelvis and the posterior screws loosening (Figure 3(a)). CT scan revealed the screw of the posterior plate migrated to the right buttock, and no tendency of the bone union was observed in the sacrum (Figure 3(b)) and pubic rami of the left pubis. CT myelogram showed that both gluteal areas were being enhanced. It proved that the CSF had leaked out into the gluteal compartment (Figure 3(c)). Magnetic resonance imaging (MRI) showed an intrasacral meningocele (Figure 3(d)) with fluid collection posterior to the sacrum and gluteal area bilaterally. Reoperation was undertaken. The posterior part of the sacrum formed the fistula and CSF leaked from there to the gluteal compartment. The delayed union at the sacral site was refixed by a posterior plate with a longer screw. A block of the autogenous bone harvested from the iliac crest was grafted between the spinous process and the posterior iliac mass, also the fluid fistula was plugged with the autogenous bone graft (Figure 4(a)). The delayed union of the left pubis was converted to plate fixation (Figure 4(b)). The gluteal fluid collection was no longer observed on the postoperative CT scans, and the sacral lamina, which had thinned posteriorly, was covered with the grafted bone (Figure 4(c)). Since the patient had no symptoms by the intrasacral meningocele before this trauma, surgical treatments of the intrasacral meningocele were not performed. At 1 year postoperatively, bone union was obtained at the delayed union sites in the sacrum (Figure 5) and left pubis. The posterior sacral plate was removed. Although mild pain in the lumbosacral area and numbness of the left lower limb remained at the final follow-up 4 years postoperatively, there was no problem in walking condition and daily life. The patient returned to his original job as a factory worker. The fractures in the sacral area and the superior and inferior rami of the left pubis had united (Figure 6).

(a) Radiograph at the time of the injury shows left sacral fracture through sacral foramen and bilateral fractures of the superior and inferior pubic rami. (b) CT scan at the time of the injury shows left sacral fracture and widening of the both the spinal canal and the sacral foramen. CT: computed tomography.

Radiograph after the first operation. The sacrum is fixed with the posterior plate and both superior pubic rami are fixed with an intramedullary screw.
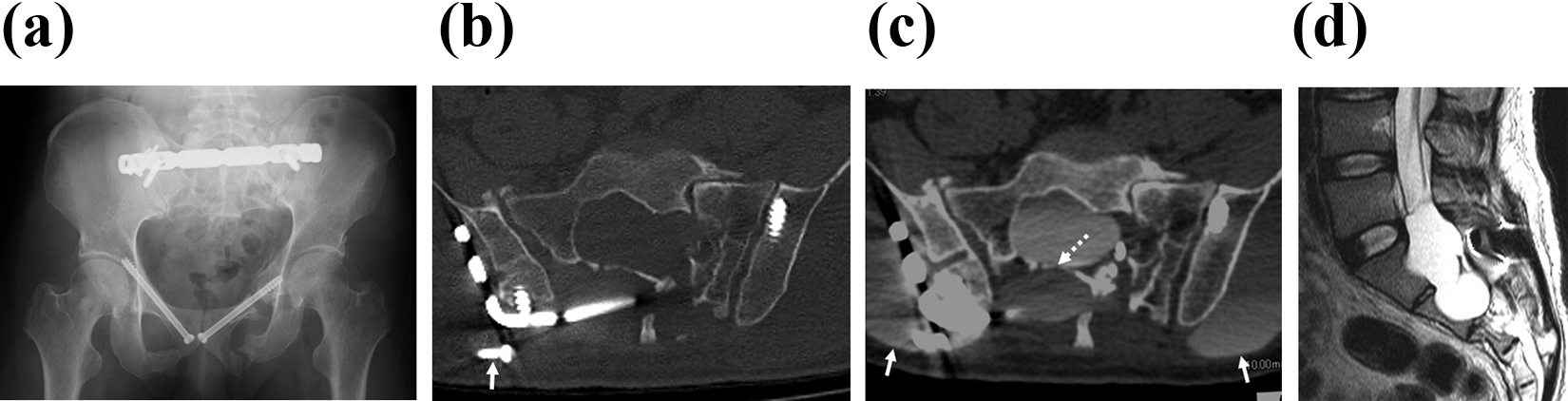
(a) Radiograph, 3 months after the first operation, shows the migration of the left hemipelvis cranially and loosening of the posterior screw. (b) CT scan, 3 months after the first operation, shows the posterior screw migrated into the right buttock (white arrow) and no tendency for bone union is observed. Thinning of the sacral lamina is clear. (c) CT myelogram, 3 months after the first operation, shows there is a leakage of the spinal fluid through the fracture of the lamina (white dotted arrow). Spinal fluid has leaked out into the gluteal compartment (white arrow). (d) MRI, 3 months after the first operation, shows an intrasacral meningocele. CT: computed tomography; MRI: magnetic resonance imaging.

(a) The illustration of the sacrum. Dotted lines indicate the fracture line. After plugging the fistula by an autogenous bone peg (dotted circle), a block bone graft harvested from the iliac crest is fixed between the spinous process and the posterior iliac mass (square). (b) Radiograph after the reoperation shows the posterior plate is fixed with longer screws and the left pubis is fixed with a longer plate. (c) CT scan after reoperation shows the sacral lamina is covered with the grafted block bone (white arrow). CT: computed tomography.

CT scan, 1 year after the reoperation, shows the bone union of the sacral body (white arrow). CT: computed tomography.

Radiograph, 4 years after the operation, shows the sacrum and superior and inferior rami of the left pubis had united.
Discussion
Sacral cysts are usually classified into three groups: anterior sacral meningoceles, perineurial cysts, and intrasacral meningoceles. 3,4 There have been reports of several cases of intrasacral meningoceles since the first case was reported in 1932 by Enderle. 1 The pathogenesis of intrasacral meningoceles is unclear, and there have been several explanations. The most widely known explanation is that they are due to a congenital factor, that is, a developmental anomaly of the dura mater, with intrasacral meningoceles forming as a result of the arachnoid herniating through a defect in the dura, 6 –9 and sacral osteolysis can be explained by increasing pressure within the cyst. As a feature of imaging findings of intrasacral meningoceles, radiographs and CT scans reveal an enlarged sacral canal with thin lamina. 6 Myelography or CT myelography demonstrates that cysts have small fistulae or a narrow communication connected to the end of the dural sac. 6,7 Further, using MRI can easily confirm the diagnosis of intrasacral meningoceles. 7,8,10
In many cases, the course of intrasacral meningoceles is asymptomatic, and they are discovered by chance. 4 They sometimes present with dull lumbosacral pain, paresthesia, and dysuria as symptoms. 7,8 Especially lumbosacral pain occurs as a result of sacral osteolysis. 10 As treatments for intrasacral meningoceles, in asymptomatic cases, follow-up is suggested. While in symptomatic or growing cases, surgical treatments by intrasacral meningoceles excision or ligation of the fistula permitting the flow of CSF is recommended. 7,10
The only report of an intrasacral meningocele complicated by a fracture is the report by Fardon. 5 The patient was injured transverse sacral fracture resulted from a hyperflexion injury. Lumbar myelography performed for the examination of the spine revealed an intrasacral meningocele. He was treated conservatively because the injury was the result of major trauma to a bone that previously has been functionally competent, and the bone union was obtained in 3 months with no pain or neural deficit. As far as we can search in the literature, our case was the only one case of the intrasacral meningocele complicated with unstable sacral fracture treated operatively. Standard treatment of unstable pelvic ring fracture with a sacral fracture is the combination of posterior fixation with anterior fixation. Usually, iliosacral screw or transsacral fixation is used for posterior fixation and plate; intramedullary screw or external fixation is used for anterior fixation. 11 –13 In this case, iliosacral screw did not provide sufficient stability because of the fracture location and there was no place to insert the transsacral bar because of the intrasacral meningocele. Because of this, combined fixation of the posterior plate and anterior intramedullary screw was employed but not stable enough because there was a little contact of the fracture especially in the posterior part of the sacrum due to the intrasacral meningocele. In addition to this, CSF leak can be cited as one of the factors responsible for the delayed union in this case. We thought that dural injury occurred with trauma because we did not touch the dura in the initial surgery. Therefore, bone union was inhibited due to the invasion of fluid between the fractures. To deal with these problems, we revised the posterior plate fixation with massive bone graft, switched intramedullary pubic screws to the plate fixation, and plugged the CSF leak with an autogenous grafted bone. This case of intrasacral meningocele with unstable pelvic fracture suggests that stronger internal fixation, that is, longer screw to fix the posterior plate and plate fixation of the superior pubic ramus in combination with bone grafting, is recommended at the initial operation.
Conclusion
An intrasacral meningocele complicated by a sacral fracture, a particularly unstable pelvic ring fracture, requires stronger internal fixation combined with bone grafting because risk of nonunion is high due to a little bone contact and CSF leak. It is necessary to evaluate the CT carefully in the planning of sacral fracture surgery to rule out the pathological lesion of the sacrum similar to this case of intrasacral meningocele with fracture.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.