
Abstract
We present a 70-year-old woman with severe diabetes mellitus, who experienced low back pain and left lower leg paralysis. Computed tomography showed air in the spinal canal from C4 to S5, and magnetic resonance imaging revealed an epidural abscess from Th11 to L1. Laboratory findings showed increases in inflammatory indicators and blood culture indicated the presence of Escherichia coli. The patient was treated conservatively with antibiotics. Neurological deficits and inflammatory data improved during the course. Follow-up imaging studies showed the disappearance of gas and epidural abscess. The existence of air in the spinal canal is a rare condition known as pneumorachis. To the best of our knowledge, such a long pneumorachis ranging from the cervical to the sacral spinal canal with epidural abscess caused by gas gangrene has not yet been described. We should therefore realize the possibility of epidural abscess produced by gas gangrene and treat it appropriately.
Introduction
Pneumorachis is a rare clinical condition characterized by the entry of air into the spinal canal. It was first described by Gordon and Hardman in 1977. 1 It is caused mainly by traumatic injury or iatrogenic etiologies, such as pneumothorax or spinal surgery. 2 However, the involvement and production of gas by gas gangrene within the spinal canal are extremely rare. To the best of our knowledge, only 10 reports of pneumorachis with epidural abscess have been identified, and in most of these cases, the gas is observed in a limited region in the spinal canal. 3 –12
Epidural abscess is a rare and potentially serious pyogenic infection. 13 Urgent surgical intervention is one of the management methods of epidural abscess, but with earlier diagnosis based on computed tomography (CT) and magnetic resonance imaging (MRI), some studies indicate successful outcomes with nonoperative medical treatment alone. 14,15
Herein, we present a rare case of pneumorachis from the cervical to the sacral spinal canal with epidural abscess produced by gas gangrene and treated with antibiotics conservatively.
Case report
A 70-year-old woman with severe diabetes mellitus (DM) presented with low back pain and paralysis of the left lower leg for 1 week, which worsened on the next day she fell on her back while walking. The paralysis did not progress a few days before she came to the hospital. She had no medical or surgical history other than DM. On admission, she presented normal general physical condition and normal body temperature (36.6°C). Physical examination revealed low back pain and grade 2/5 weakness in her left tibialis anterior (TA) and left extensor hallucis longus (EHL) on manual muscle test (MMT). Her muscle tone and reflexes were normal. The patient reported no hypesthesia and no urinary or bowel dysfunction.
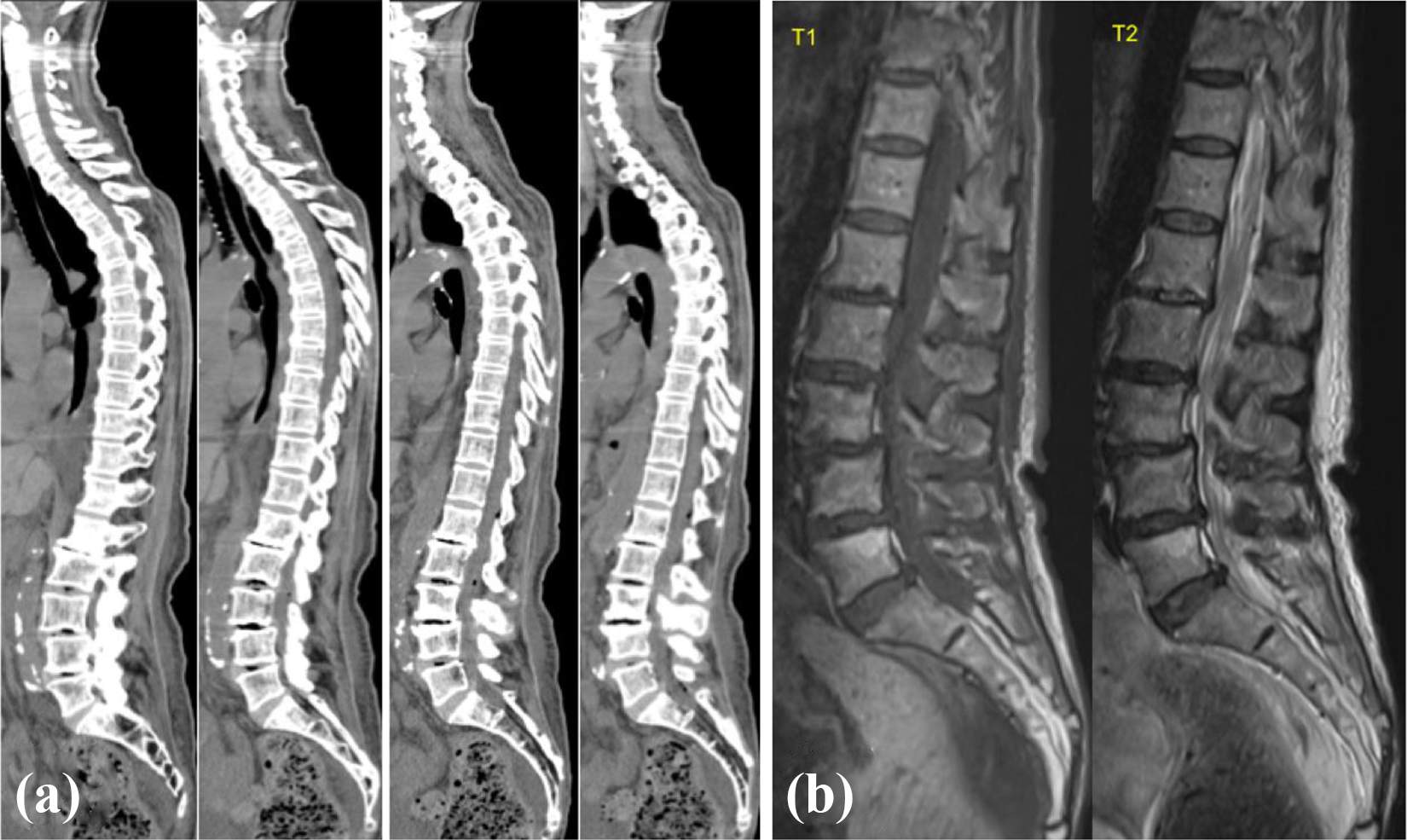
Laboratory examination revealed a white blood cell (WBC) count of 20,100 cells/mm3 (normal: 3300–8600 cells/mm3) and C-reactive protein (CRP) level of 31.86 mg/dL (normal: 0–0.14 mg/dL). Hemoglobin A1c (HbA1c) level (value based on the Japan Diabetes Society (JDS)) was 11.7% (normal: 4.3–5.7%). Urine test was negative. CT pan-scan was performed to detect the cause of inflammatory reaction. It presented intraspinal air in the spinal canal from C4 to S5 and showed no pneumocephalus (Figure 1(a)). A chest and abdomen CT revealed no significant abnormalities, including tumor, abscess, pneumothorax, pneumomediastinum, or fractures. Urgent MRI showed an intraspinal epidural mass from the Th11 to L1 level with decreased signal intensity on T1-weighted images and increased signal intensity on T2-weighted images (Figure 1(b)).

(a) CT demonstrating intraspinal air from the cervical to the sacral spinal canal. (b) MRI demonstrating an intraspinal epidural mass from Th11 to L1 level with decreased signal intensity on T1-weighted images and increased signal intensity on T2-weighted images. CT: computed tomography; MRI: magnetic resonance imaging.
These results suggested spinal epidural abscess produced by gas gangrene. After obtaining blood culture, intravenous meropenem (1 g × 3/day) was administered, and symptoms and laboratory data were carefully followed conservatively with the treatment of DM. After admission, inflammatory data and blood sugar level improved gradually, and neurological deficits showed no deteriorations during the course. Two sets of blood cultures were positive for Escherichia coli. On the fifth day after admission, meropenem was converted to cefmetazole (1 g × 3/day), to which E. coli was susceptible. On the 15th day, the pneumorachis almost disappeared on CT, and MRI showed no spinal epidural abscess (Figure 2). Blood culture on the 16th day was negative. On the 27th day, her WBC count was 7300 cells/mm3, CRP was 0.65 mg/dL, and HbA1c (JDS) was 8.0%. Regarding her neurological impairment, the MMT of TA and EHL gradually improved to 4/5, respectively. As a result, the patient was able to walk with a cane at the last follow-up.
(a) Computed tomography images showing the disappearance of intraspinal air. (b) Magnetic resonance image confirming the disappearance of epidural abscess.
Discussion
Pneumorachis is a rare condition where air invades the spinal canal, and it is mainly caused by trauma. According to the literature, 16 the cause in 53% of pneumorachis cases was injury to the respiratory system (pneumothorax, pneumomediastinum, etc.). The next most common cause of pneumorachis was intracranial injury, and other causes of pneumorachis associated with degenerative disc disease or intra-abdominal viscera have been reported. An epidural abscess with gas-producing organisms is a rare cause of pneumorachis. In the present case, an inflammatory reaction was noted in a blood test, E. coli was identified on blood culture, intraspinal gas was noted on CT, a spinal abscess was noted on MRI, and the gas and abscess disappeared after treatment. These findings suggested that this pneumorachis was caused by a spinal epidural abscess with gas gangrene. Moreover, the air in the posterior space of the spinal canal indicated that the pneumorachis was caused by an epidural abscess and not by a degenerative disc disease, which mostly shows air in the anterior space of the spinal canal. Only 10 reports have presented cases of pneumorachis with an epidural abscess (Table 1), and to the best of our knowledge, our report presents the longest pneumorachis from the cervical to the sacral spinal canal. The incidence of an epidural abscess is increasing, and the current incidence has been estimated to be 2–12.5 per 10,000 admissions, which can be attributed to the aging population, increasing use of spinal instrumentation, vascular access, and so on. 14
Summary of all cases of pneumorachis with epidural abscess.

Spinal epidural abscess may occur by direct extension from a local infection or by hematogenous or lymphatic spread. 3 For those with risk factors, including DM, obesity, or long-term steroid intake, hematogenous spread is the main cause of spinal epidural abscess. 17 In the present case, the patient had uncontrolled DM and was susceptible to infection. Moreover, despite no evidence of pyuria, CT showed low-density area in the right kidney, which suggested pyelonephritis. This might indicate that the epidural abscess was caused by a pathogen (later detected as E. coli) via the urinary tract hematogenously.
The main causative organisms of epidural abscess are Staphylococcus aureus (about 50% of cases), and other gram-positive cocci (such as Staphylococcus epidermidis, Enterococcus faecalis, etc.) and gram-negatives (such as Acinetobacter, Citrobacter koseri, Enterobacter, E. coli, Serratia marcescens, etc.). 18 In this case, E. coli was identified in two sets of blood cultures and was suspected as the pathogen of epidural abscess. Table 1 shows various pathogens causing epidural abscess with pneumorachis. While the most reported pathogen is S. aureus, E. coli has been identified in only one paper, and the route of infection is not evident. 10
Patients with epidural abscess have varied symptoms. According to a report of 101 cases of spinal epidural abscess, 18 about 84% of patients had back pain, 42% had neurologic signs (9% had paralysis), 24% had fever above 38°C, and only 8% had the classic triad of spinal pain, fever, and neurologic deficit. Patients with epidural abscess and pneumorachis also have varied symptoms such as pain, fever, or paralysis (Table 1).
Regarding the diagnosis, MRI is the gold standard for epidural abscess. X-ray imaging sometimes shows a vertebral osteomyelitis, and CT may show a loss of epidural fat, abnormal enhancement between bone and the dural sac, and a soft tissue mass in a spinal canal. 19 However, MRI shows the exact location of an abscess and identifies spinal or paraspinal infection. 20 Epidural abscesses with pneumorachis are all diagnosed with MRI, except for one case reported by Kirzner et al., where CT revealed an ill-defined soft tissue density with gas in the spinal canal. 3 As we have mentioned, epidural abscess with gas-producing organisms are very causes of pneumorachis. However, we have to take into account the possibility of epidural abscess with gas gangrene when we encounter patients with pneumorachis based on CT. In our case, the spinal gas location ranged from C4 to S5 spinal canal on CT. This long pneumorachis is very rare, and the reason is unknown, but the patient’s uncontrolled DM and delay of diagnosis for a week without treatment might have affected the progression of air produced by gas gangrene.
Urgent surgical intervention with systemic antibiotics has been the standard treatment of spinal epidural abscess, especially for patients presenting with evolving neurological deterioration, spinal instability, or persistence of infection despite antibiotic treatment. 21,22 However, by earlier diagnosis with MRI, nonoperative management is a valid treatment option for spinal epidural abscess. 17,23 Some papers consider the algorithm for the treatment or risk factors for failure of medical therapy, but it is still controversial. 15,16 The present patient had weakness in her left TA and left EHL, but no deterioration was identified a few days before coming to the hospital. She was first treated with antibiotics and her clinical course was followed carefully. As a result, the patient improved dramatically without surgical management. According to Table 1, all cases have been treated using combination of antibiotics and surgical intervention so far. We do not and cannot make any conclusion about the efficacy of the medical treatment or surgical management, and further discussion about the treatment is needed.
Conclusion
We presented a rare case of the longest pneumorachis ranging from the cervical to the sacral spinal canal with an epidural abscess by gas gangrene due to E. coli among the reported cases of pneumorachis with an epidural abscess in the literature. In most cases, intraspinal gas with infection was noted in a limited region, but the finding in this case suggests that pneumorachis with an epidural abscess could extend throughout the spinal canal. The present case suggests that a spinal epidural abscess by gas gangrene should be considered in the differential diagnosis of pneumorachis and that gas extension from the cervical to the sacral spinal canal could be detected with a spinal epidural abscess. We should therefore realize the possibility of an epidural abscess produced by gas gangrene and provide appropriate treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.