
Abstract
Purpose:
To analyze the incidence, pattern, and contributing factors of pelvic obliquity among Adolescent Idiopathic Scoliosis (AIS) patients who will undergo surgery.
Methods:
In total, 311 patients underwent erect whole spine anteroposterior, lateral and lower limb axis films. Radiographic measurements included Transilium Pelvic Height Difference (TPHD; mm), Hip Abduction-Adduction angle (H/Abd-Add; °), Lower limb Length Discrepancy (LLD; mm), and Pelvic Hypoplasia (PH angle; °). The incidence and severity of pelvic obliquity were stratified to Lenke curve subtypes in 311 patients. The causes of pelvic obliquity were analyzed in 57 patients with TPHD ≥10 mm.
Results:
The mean Cobb angle was 64.0 ± 17.2°. Sixty-nine patients had a TPHD of 0 mm (22.2%). The TPHD was <5 mm in 134 (43.0%) patients, 5–9 mm in 104 (33.4%) patients, 10–14 mm in 52 (16.7%) patients, 15–19 mm in 19 (6.1%) patients, and ≥20 mm in only 2 (0.6%) patients. There was a significant difference between the Lenke curve types in terms of TPHD (p = 0.002). L6 curve types had the highest TPHD of 9.0 ± 6.3 mm followed by L5 curves, which had a TPHD of 7.1 ± 4.8 mm. In all, 44.2% of L1 curves and 50.0% of L2 curves had positive TPHD compared to 66.7% of L5 curves and 74.1% of L6 curves which had negative TPHD. 33.3% and 24.6% of pelvic obliquity were attributed to PH and LLD, respectively, whereas 10.5% of cases were attributed to H/Abd-Add positioning.
Conclusions:
76.4% of AIS cases had pelvic obliquity <10 mm; 44.2% of L1 curves and 50.0% of L2 curves had a lower right hemipelvis compared to 66.7% of L5 curves and 74.1% of L6 curves, which had a higher right hemipelvis. Among patients with pelvic obliquity ≥10 mm, 33.3% were attributed to PH, whereas 24.6% were attributed to LLD.
Keywords
Introduction
Pelvic obliquity (PO) in scoliosis had been recognized in patients with spastic scoliosis or neuromuscular scoliosis. 1 –4 Pelvic obliquity can be assessed by its anatomical origin, whether it is caused by a suprapelvic, intrapelvic, or infrapelvic problem or any combination of these problems. 1,4 Suprapelvic cause is secondary to the spinal deformity in which scoliosis may drive the pelvis into an asymmetrical position. The intrapelvic cause is secondary to morphological changes of the pelvis that leads to either hypoplasia of the ilium, the ischium or the whole hemipelvis. The infrapelvic cause is secondary to hip contractures (e.g. hip flexion contracture) or lower limb length inequality. Cummings et al. had noted that pelvic asymmetry was proportional to leg length inequality difference. 5 Winter and Pinto had described that pelvic obliquity can be caused by leg length inequality, hip contractures, structural scoliosis, or any combination of these. 2 However, there was no previous literature that reported the incidence and causes of pelvic obliquity for patients with Adolescent Idiopathic Scoliosis (AIS). This study assessed the lower limb axis films in 311 AIS patients to determine the incidence of pelvic obliquity in AIS patients and to formulate an etiological classification of pelvic obliquity.
Materials and methods
This was a retrospective study carried out in a single academic institution from January 2013 to December 2015. This study received institutional review board approval (MECID no: 2017525-5268). The inclusion criteria for this study were patients with a diagnosis of AIS who were planned for Posterior Spinal Fusion (PSF) and patients with complete preoperative radiological investigations that included a good quality lower limb axis film. Patients with previous surgery to the lower limb or the spine or who had other developmental abnormalities of the lower limb were excluded. The surgical indication for AIS was major Cobb angle >45° on the erect whole spine radiograph.
The objective of the study was to analyze the incidence, pattern, and contributing factors of pelvic obliquity among AIS patients who will be undergoing surgery. During this period, a total of 335 patients fulfilled the study’s inclusion criteria. Twenty-four patients were excluded as the clarity or completeness of the lower limb radiographs were inadequate. A total of 311 patients were included in the analysis of the incidence and pattern of pelvic obliquity among AIS patients. From this group of patients, 73 patients had pelvic obliquity of ≥10 mm but among these patients, 16 patients had significant pelvic rotation (PR) in their lower limb axis radiographs and were excluded. This subgroup of 57 patients was analyzed for the contributing factors of pelvic obliquity.
All patients underwent an additional standing lower limb axis films for this study as well as the routine preoperative radiographs for surgical planning. The lower limb axis films were full-weight bearing films with the patient instructed to stand in their most natural position. From the lower limb axis film, the following radiographic parameters were obtained (Figures 1 and 2):
Transilium Pelvic Height Difference (TPHD) (mm): Difference in height between the right and left hemipelvis (positive value denotes left hemipelvis higher). Hip Abduction-Adduction (H/Abd-Add) angle: Angle formed between a line connecting the center of the symphysis pubis and the midpoint between both medial malleoli and a vertical axis (positive value denotes Hip Abd-Add led to right hemipelvis lower). Lower Limb Length (mm): Measurement from the center of the femoral head to the center of the ankle joint. Lower limb Length Discrepancy (LLD, mm): Difference between the length of right and the left lower limb (positive value denoted right lower limb longer). Pelvic Hypoplasia (PH, °): Angle formed by transilium and transischium line (positive value denotes left hemipelvis higher). Pelvic Rotation (PR): Presence of PR was determined, as described by Gum et al.,
6
by measuring the width of each hemipelvis from the anterior superior iliac spine to the inferior ilium at the sacroiliac joint. The ratio of the width of both hemipelvis was then derived. Physiological PR was defined as L/R ratio within the range of 1 ± 0.1.
7
PR more than this range was considered PR +ve.
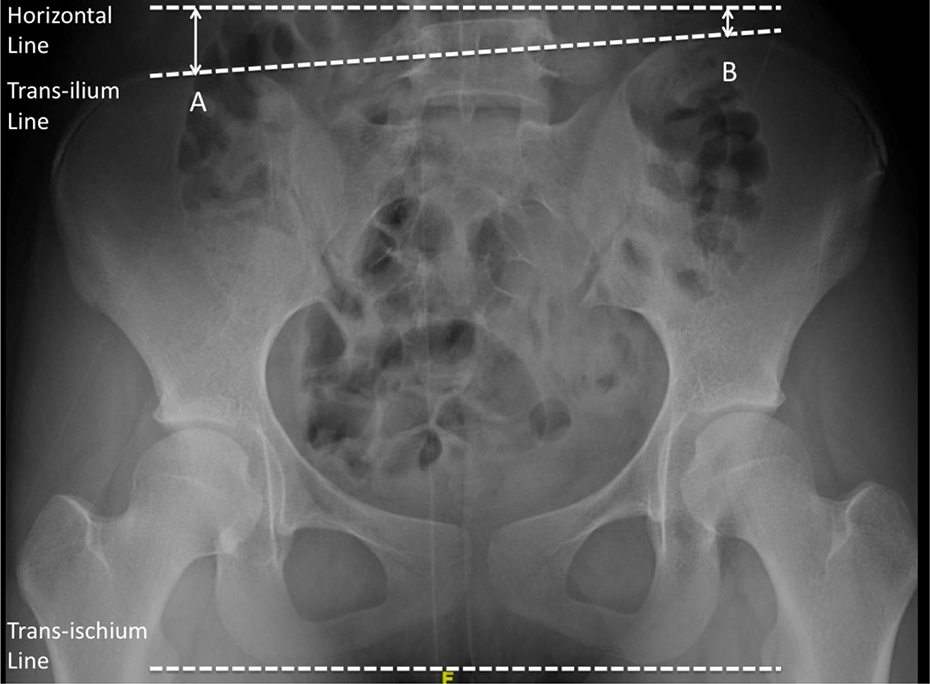
Measurement of TPHD (difference between measurement A and B in millimeter) and PH angle (angle formed by the transilium and transischium line). PH: pelvic hypoplasia; TPHD: transilium pelvic height difference.

Measurement of Lower Limb Discrepancy (difference between right and left lower limb) and Hip Abduction-Adduction (H/Abd-Add) angle (angle formed by vertical axis and line connecting center of the pubic symphysis and the midpoint of both medial malleoli).
Two observers measured the TPHD, limb-length for both the right and the left lower limb, and H-Abd/Add angle for 20 patients. An intraclass correlation coefficient (ICC) value of less than 0.4 indicated poor reliability, 0.4–0.7 indicated fair to good reliability, and 0.75–1.0 indicated excellent reliability. We classified the possible contributing factors of pelvic obliquity to seven types, as shown in Table 1. To determine the contributing factors of pelvic obliquity, only LLD ≥ 5 mm, PH ≥ 1°, H/Abd-Add ≥ 1° were considered significant. Figures 3 to 5 illustrate pelvic obliquity caused by LLD, H/Abd-Add and PH.
Contributing factors for pelvic obliquity.

LLD: Limb Length Discrepancy; PH: Pelvic Hypoplasia; H-Abd-Add: Hip Abduction-Adduction.

Lenke 1A curve with TPHD of +18 mm, LLD of −17 mm, preoperative Cobb angle of 54° and postoperative radiograph at 24 months follow-up with Cobb angle of 21°.

Lenke 6C curve with TPHD of −13 mm, PH −4°. Preoperative lumbar Cobb angle of 63° corrected to 23°. Coronal balance was −18 mm at 27 months follow-up.

Lenke 1B curve with TPHD of −14 mm, H/Abd-Add angle −4°. Preoperative Cobb angle was 55°, which was corrected to 20°. Coronal balance was −9 mm at 25 months after the surgery. H/Abd-Add: Hip Abduction-Adduction.
Postoperative outcome
Following PSF, the whole spine erect radiographs at the final follow-up were analyzed for a change in the pelvic obliquity. This was to detect changes in the pelvic obliquity when the underlying cause was due to H/Abd-Add positioning (assumed to be postural in nature). This was in contrast to lower LLD or PH whereby the pelvic obliquity would still persist postoperatively.
Results
Measurement reliability of the radiological parameters
Limb-length (left side) recorded the highest ICC value, which was 0.97 with a mean difference of 3.0 ± 11.5 mm. The remaining variables showed excellent reliability with ICC values of 0.94, 0.96, and 0.89, respectively. As for intraobserver reliability, the ICC values were highest for limb-length for both right and left with a value of 0.99 and a mean difference of 1.0 ± 3.1 and 0.1 ± 3.5, respectively. The remaining variables showed excellent intraobserver reliability with ICC values of 0.95 and 0.82. Table 2 shows ICC values for each variable and its respective mean differences.
ICC and mean difference of each variable.
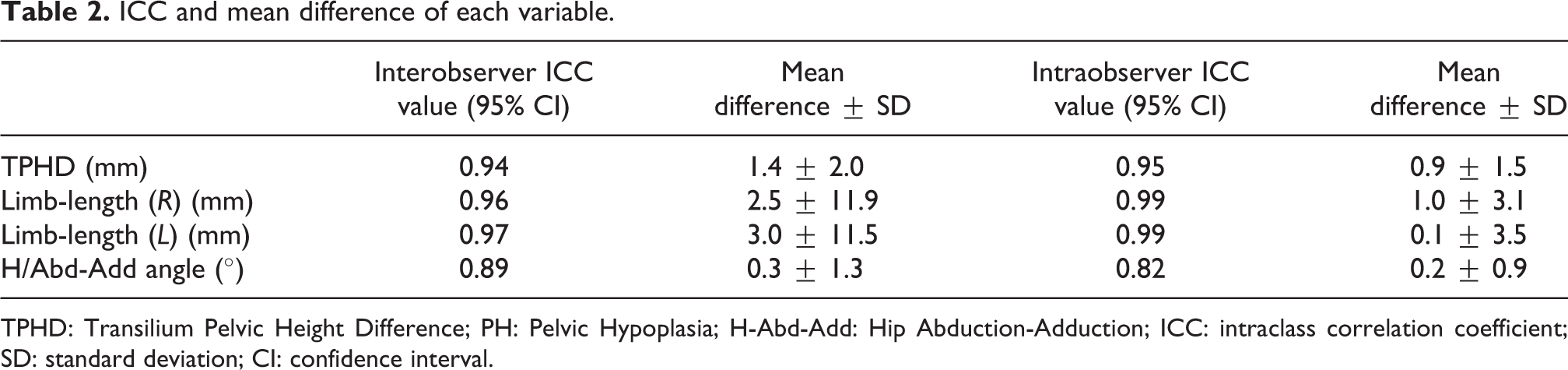
TPHD: Transilium Pelvic Height Difference; PH: Pelvic Hypoplasia; H-Abd-Add: Hip Abduction-Adduction; ICC: intraclass correlation coefficient; SD: standard deviation; CI: confidence interval.
Demographics and incidence of pelvic obliquity
A total of 311 patients were included in the study. 90.7% of patients were females (n = 282), and the average age of this cohort was 15.1 ± 2.6 years. The mean Cobb angle was 64.0 ± 17.2°, whereas the average TPHD was 6.0 ± 5.0 mm. Only 69 patients had a TPHD of 0 mm (22.2%). 57.0% of patients had TPHD of 5 mm or more, whereas 23.6% of patients had TPHD of 10 mm or more (Table 3). In our series, only two patients had TPHD of more than or equal to 20 mm. The majority of the patients in our cohort had Lenke 1 curve (52.4%) followed by 17.4% Lenke 5 curves and 16.7% Lenke 2 curves (Table 3).
Demographics data of the patient cohort.

TPHD: Transilium Pelvic Height Difference; SD: standard deviation.
There was a significant difference between the Lenke curve types in terms of TPHD (p = 0.002). Lenke 6 curve types had the highest TPHD of 9.0 ± 6.3 mm. This was followed by Lenke 5 curves, which had a TPHD of 7.1 ± 4.8 mm and Lenke 2 curves, which had a TPHD of 6.1 ± 5.4 mm. analysis of variance with post hoc Tukey test found statistically significant when comparing Lenke 6 and Lenke 1 curves only with a p-value of 0.002. No significant difference was found when we compared the other Lenke curve types in terms of TPHD. There was also no significant difference between the various Lenke curve types in terms of PH angle and H/Abd-Add angle (Table 4).
TPHD, PH, and H-Abd-Add angle for each Lenke classification.

TPHD: Transilium Pelvic Height Difference; PH: Pelvic Hypoplasia; H-Abd-Add: Hip Abduction-Adduction.
In Lenke 1 and 2 curves, the left hemipelvis was higher than the right in the majority of cases. In Lenke 1 curves, among patients with pelvic obliquity, 44.2% of patients had positive TPHD, and in Lenke 2 curves, 50.0% of patients had positive TPHD. This is in comparison with Lenke 5 and Lenke 6 curves whereby the larger proportion of patients had negative TPHD. In Lenke 5 curves, 66.7% of patients had negative TPHD, and in Lenke 6 curves, 74.1% of patients had negative TPHD. The difference in the direction of TPHD between the various Lenke curve types showed statistically significant difference with p < 0.05 (Figure 6).
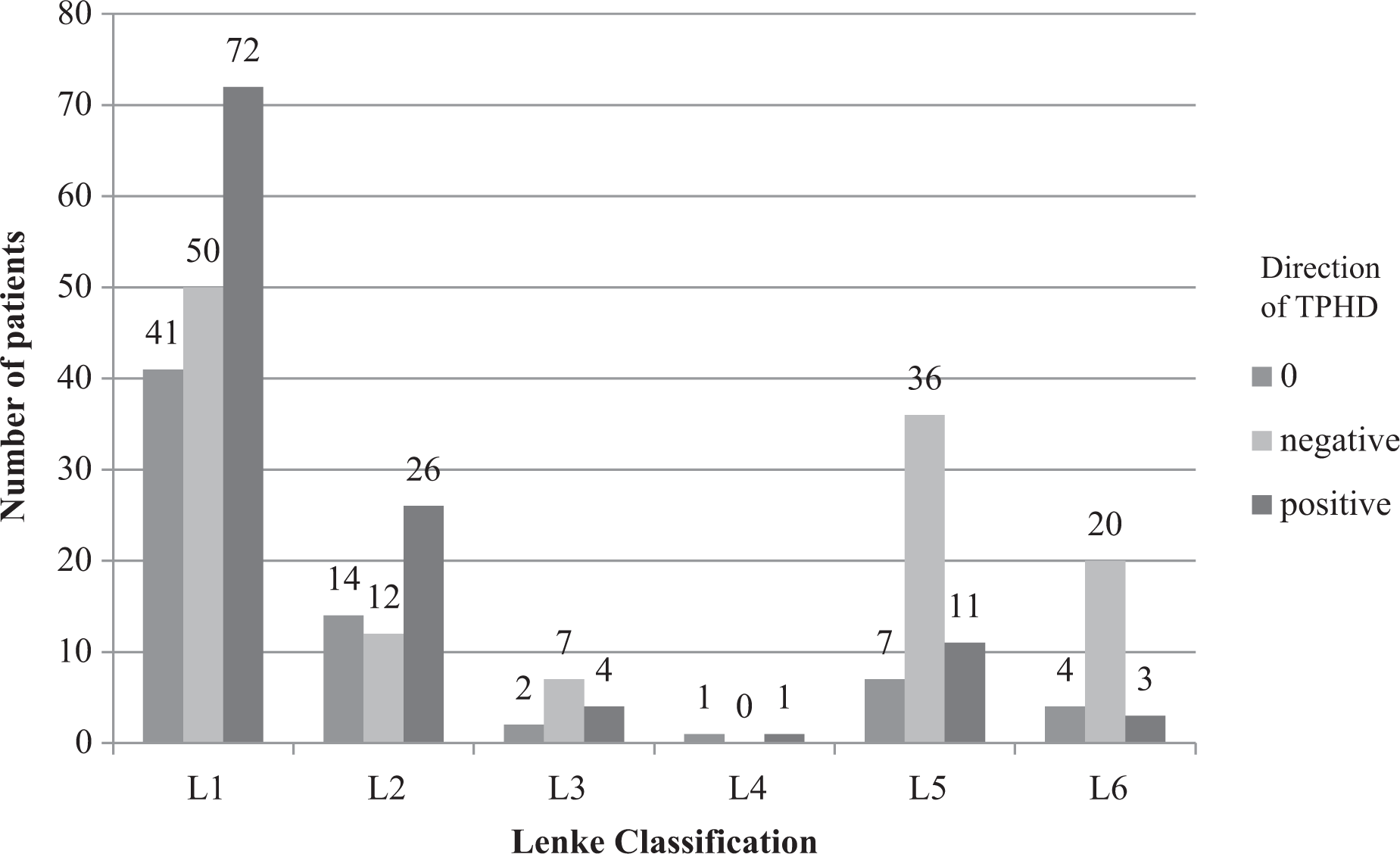
Direction of TPHD stratified to Lenke classification. TPHD: Transilium Pelvic Height Difference.
Contributing factors for pelvic obliquity
Among the 57 patients with TPHD ≥10 mm without significant PR, we found that in 33.3% of cases, PH contributed to pelvic obliquity. In 24.6% of cases, isolated significant LLD was the contributing factor for pelvic obliquity, whereas in 19.3% of cases, the contributing factor was a combination of PH and H/Abd-Add positioning. Regardless of the underlying contributing factor for pelvic obliquity, the TPHD magnitude did not show a statistically significant difference. Table 5 summarizes the causes of Pelvic Obliquity (PO) and the corresponding TPHD, LLD, PH, and H/Abd-Add measurements.
Contributing factors towards pelvic obliquity.
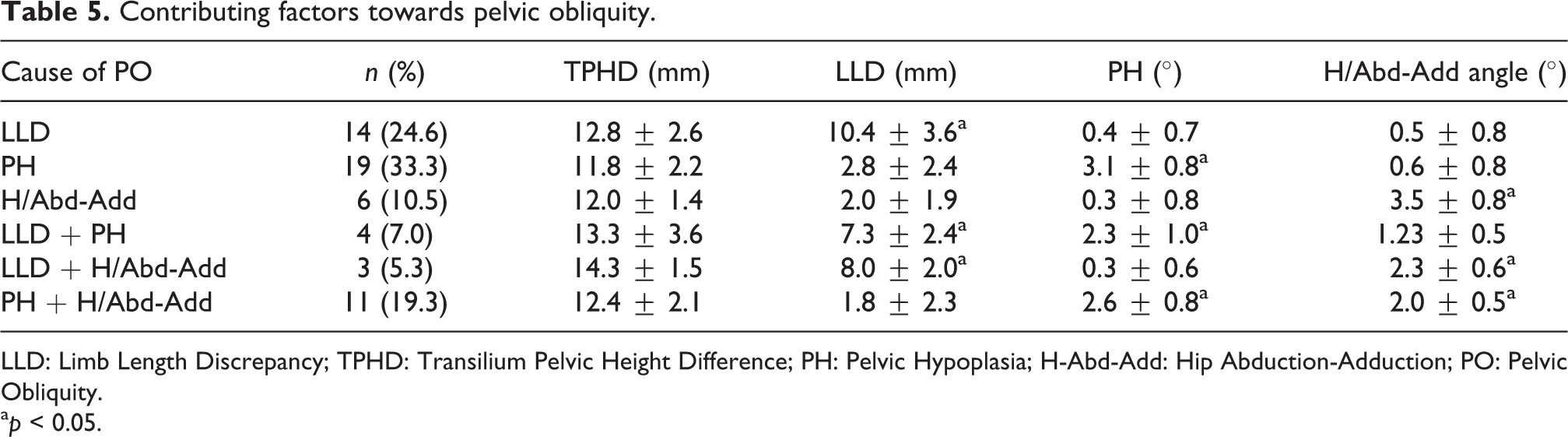
LLD: Limb Length Discrepancy; TPHD: Transilium Pelvic Height Difference; PH: Pelvic Hypoplasia; H-Abd-Add: Hip Abduction-Adduction; PO: Pelvic Obliquity.
a p < 0.05.
Postoperative changes in pelvic obliquity
Figure 7 illustrates the changes in pelvic obliquity measured on the final follow-up whole spine erect radiographs. Pelvic obliquity which was contributed by H/Abd-Add showed the largest change with a mean difference of 2.5 ± 1.2°. This was in comparison to pelvic obliquity contributed by lower LLD and PH, which showed a mean difference of 0.8 ± 0.7° and 0.6 ± 0.8°, respectively. The differences between postoperative changes in pelvic obliquity comparing the three groups were statistically significant (p < 0.05).

Postoperative difference in pelvic obliquity stratified to the contributing factors for pelvic obliquity.
Discussion
One of the aims of scoliosis surgery is to achieve a well-balanced spine. Spinal balance in the coronal plane is achieved by aligning the centroid of the C7 to the center of the sacrum. Therefore, the pelvis forms the foundation for the spinal construct in PSF for scoliosis.
In both King’s and Lenke’s classification, the importance of a leveled pelvis was emphasized. In King’s classification, the authors recommended that when LLD was present, the pelvis should be leveled with an appropriate shoe lift and the central vertical line must always be based on a horizontal pelvis. 8 In Lenke’s classification, the authors recommended that pelvic obliquity is secondary to limb length inequality <2 cm should be ignored unless the surgeon believes that this worsens the severity of the spinal deformity. When the discrepancy is >2 cm, the radiograph should be performed with the presence of a shoe lift. 9 However, in both classification, the pelvis was not included as part of the classification, which was the subject of the critique by Maurice et al. 10
Asymmetry of pelvic morphology is often encountered in erect anteroposterior whole spine radiograph in AIS patients. The pelvic axial rotation has been investigated by many authors. 6,7,11 –13 Gum et al. concluded that the PR in the transverse plane was in the same direction of the apical thoracic vertebral rotation in major thoracic curves (Lenke 1, 2, and 3 curve types) and that Lenke 1 and 2 curve types without a compensatory thoracolumbar or lumbar curve did not have the predicted rotation. 6 Zhao et al. 7 defined physiological PR as left/right ratio within the range of 1 ± 0.1, whereas Lucas et al. 12 defined the normal range of convex/concave ratio as from 0.95 to 1.05. Qiu et al. performed a retrospective study in 38 AIS patients with thoracolumbar/lumbar curve and found that in patients with pelvic axial rotation, there was a higher incidence of coronal decompensation. 13
Abnormalities in the pelvis and hip geometry have also been associated with AIS. Tomasz reported that AIS patients had significant adduction range deficit of the right hip compared to normal subjects. 14 Saji et al. studied 61 AIS patients and compared to normal subjects was found to have increased femoral neck-shaft angle. 15 Stylianides et al. reported that the difference in iliac spine geometry was noted in AIS patients with severe scoliosis compared to those without scoliosis or with moderate curves and, therefore, in surgical correction of AIS, the presence of pelvic obliquity could increase the incidence of coronal decompensation particularly when fusion was extended to the lumbar spine. 16
Schwender and Denis reported the results of a retrospective radiographic analysis of 50 AIS patients with lumbar curve more than 40°. 17 The incidence of coronal decompensation was 43% in King 1 curves, 42% in King 2 curves, and 50% in T/L or lumbar curves. In patients with L4 tilt more than 20° to the horizon, 96% had decompensation before surgery. This group of patients also had a higher incidence of coronal decompensation postoperatively. Sacral obliquity and iliac obliquity were identified as risk factors for coronal decompensation as well. McCance et al. reported that the incidence of decompensation in King 2 curves was 30%, but the authors did not identify the causes of the decompensation. 18 Li et al. concluded that in Lenke 5C curves, preoperative Lowest Instrumented Vertebra (LIV) tilt exceeding 25° or failure of postoperative LIV tilt to reduce below 8° were predisposing factors for global coronal imbalance. 19
In one recent publication, Cho et al. described the association with sacral slanting and pelvic obliquity in AIS. In this study which included analysis of 303 AIS patients, the authors reported a high correlation rate between sacral slanting with pelvic obliquity and lumbar curve. However, pelvic obliquity was found to correlate significantly with L4 tilt and lower limb discrepancy. Lower limb discrepancy did not have a significant correlation with sacral slanting. However, in that study, the direction and contributing factors toward pelvic obliquity were not described. 20 Our study was the first study to analyze the lower limb axis film in AIS patients and to investigate the incidence, pattern, and possible causes of pelvic obliquity. Only 22% of patients had a perfectly horizontal pelvis and Lenke 5 and 6 curves had the highest magnitude of pelvic obliquity. From our data, pelvic obliquity more than 2 cm was uncommon and this occurred in only 2 (0.6%) patients. There was also a significant difference in the direction of pelvic obliquity in patients with main thoracic major curves compared to patients with lumbar major curves. In patients with lumbar major curves, majority of patients had higher right hemipelvis.
We excluded cases with pelvic obliquity <10 mm and with significant PR to analyze the possible contributing factors toward the pelvic obliquity. PR will affect the measurement of pelvic obliquity and PH. It is of interest to note that among the 57 cases analyzed for the cause of pelvic obliquity, 33.3% of the cases were attributed to isolated PH, whereas 24.6% of cases were caused by isolated LLD. We would consider these two causes as structural causes of the pelvic obliquity, which needs to be considered during surgical correction of AIS even though the degree of pelvic obliquity could be less than 2 cm. As shown in the results (Figure 7), when pelvic obliquity was contributed by H/Abd-Add, the magnitude of the pelvic obliquity would diminish postoperatively as a patient would compensate following correction of the scoliotic curve. However, when PH or LLD was present, the pelvic obliquity would still persist at the final follow-up, indicating they were indeed structural causes.
In the presence of structural causes of the pelvic obliquity, overcorrection of the lumbar curve would increase the likelihood of coronal decompensation or distal disc wedging. This was important particularly when fusion was extended to the lumbar spine (Figure 8). To mitigate this potential complication, intraoperative coronal balancing should account for the difference in ilium height when simulating the Center Sacral Vertical Line (CSVL). In contrast, there was a possibility that when the pelvic obliquity was caused by H/Abd-Add positioning, patients would be able to compensate for the pelvic obliquity postsurgical correction as the positioning of the hips could be postural. Therefore, when intraoperative confirmation of spinal balance is performed (CSVL as aligned to C7), there is a structural cause leading to pelvic obliquity, the difference of TPHD should be accounted for when this step is performed (Figure 9). However, this research question would need to be answered in a larger scale study.

Case illustration of pelvic obliquity caused by isolated Lower Limb Length Discrepancy of 11 mm. Postoperative radiographs showed coronal decompensation of 20 mm with significant distal disc wedging.

Intraoperative confirmation of spinal balance in the presence of significant pelvic obliquity (a and b).
This study had several limitations. Although this is currently the largest series of cases, which analyzed the lower limb axis of AIS patients, we could only include 57 cases in the analysis of the contributing factors for the pelvic obliquity. The lower limb axis radiographs were not centered on the pelvis and, therefore, there could be some parallax effect in the measurement of the pelvic obliquity. However, we have shown high interrater reliability in the measurement of the outcome parameters in this study. This study was designed to investigate the incidence, pattern, and contributing factors for pelvic obliquity in AIS. A different study would be needed to analyze the effect of the degree of pelvic obliquity and the cause of pelvic obliquity toward the outcome of surgical correction. In such study, other parameters such as curve flexibility, L5 orientation, and C7 plumb line distance should be taken into account. A computed tomography scan would be more reliable in studying the geometry of the pelvis particularly in the presence of PH but this was not feasible in our study as this would subject the patients to higher radiation exposure. In determining the presence of PH, even slight rotation in the pelvis might affect the measurement of the transilium–transischium angle, this might result in a higher incidence of PH in our series. However, the method of determining physiological PR has been validated in other studies. Future studies would be needed in multicenter trials to validate the contributing factors for PH, as described in this study.
Conclusion
In conclusion, pelvic obliquity was present in 77.8% of patients. However, pelvic obliquity >2 cm was only present in 2 (0.6%) patients. Significant differences exist in the severity and direction of pelvic obliquity in different Lenke curve types. Isolated PH and LLD were the two most common causes of pelvic obliquity ≥10 mm in the absence of significant PR. Both the identification and quantification of pelvic obliquity are important prior to corrective surgery for a patient with idiopathic scoliosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.