
Abstract
Introduction
The influence of prior high tibial osteotomy (HTO) on total knee arthroplasty (TKA) functional outcomes remains widely debated. Alignment of failed HTO can pose technical challenges with subsequent TKA. The primary aim of this study was to evaluate the influence of HTO alignment on the clinical outcomes of subsequent TKA. The secondary aim was to compare the time to TKA for each HTO alignment type.
Methods
Patients who underwent TKA post lateral closing-wedge HTO for symptomatic medial compartment osteoarthritis between 2001 and 2014 were prospectively followed up for 2 years. A total of 159 patients were assigned to three groups based on their pre-TKA femora tibia angles using long lower limb radiographs: varus alignment (VrA) ≤ 3o valgus, neutral alignment (NA) 3-9o valgus alignment, valgus alignment (VlA) ≥ 9o valgus. Functional outcomes were quantified using Knee Society Function Score and Knee Scores (KSFS and KSKS respectively), modified Oxford Knee Score (OKS), Short Form 36 Physical Component Score (SF-36 PCS), and SF-36 Mental Component Score (SF-36 MCS). Pre-operative and post-operative knee range of motion were also measured.
Results
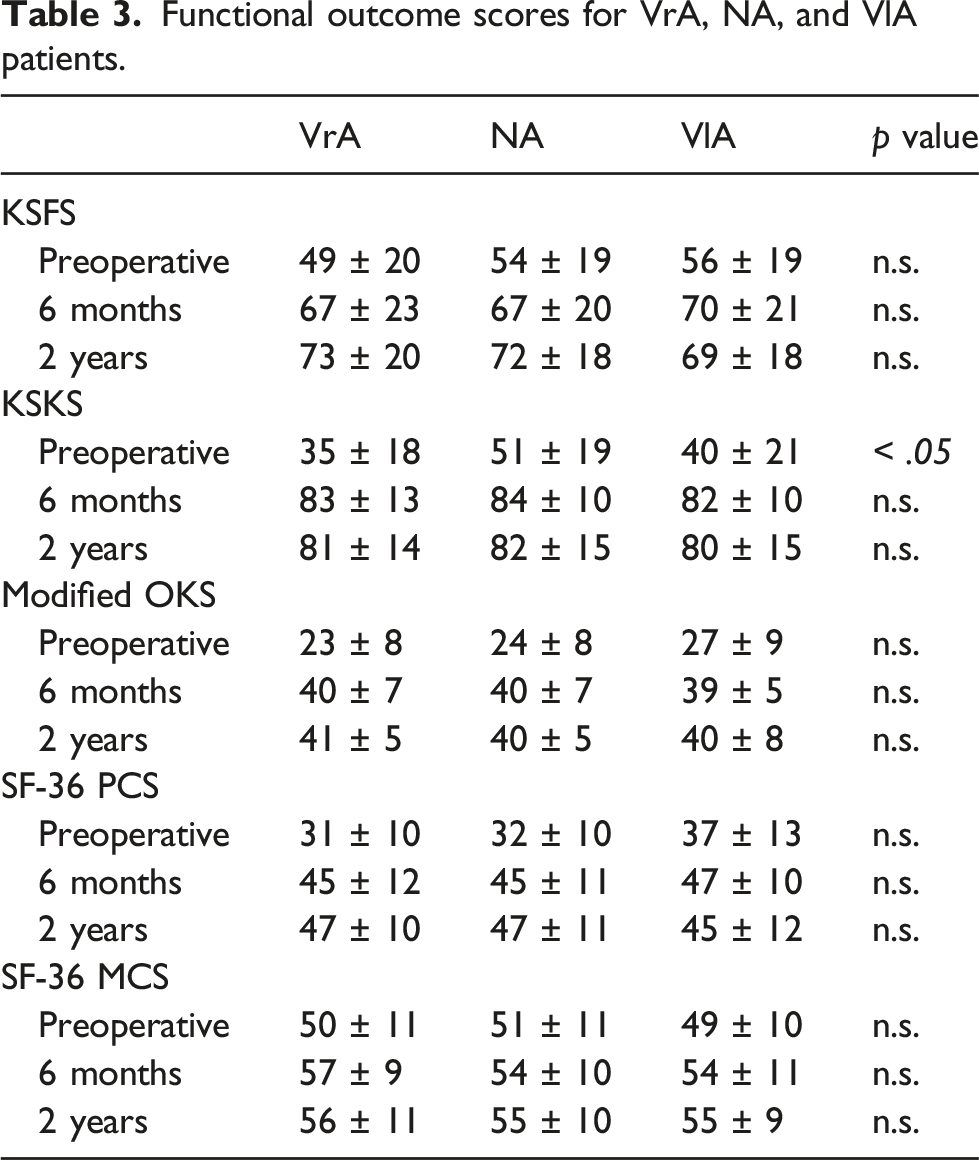
Mean pre-TKA KSKS in VrA patients (35 ± 18) was significantly lower than both NA (51 ± 19) and VlA (40 ± 21) patients (p < .05). Otherwise, there was no significant difference in functional outcome scores (KSFS, KSKS, OKS, SF-36 PCS and SF-36 MCS) or range of motion at 6 months and 2 years post-TKA. The mean duration from HTO to TKA was 12 ± 7 years with no significant differences between VrA, NA, and VlA HTO to TKA (13 ± 7 years, 13 ± 6 years and12 ± 8 years respectively, p > .05).
Conclusion
HTO alignment did not influence time to subsequent TKA. HTO alignment did not influence early outcomes as well as radiological outcomes of subsequent TKA.
Level of evidence
III
Keywords
Introduction
High tibial osteotomy (HTO) is a surgical treatment option for patients who present with symptomatic isolated medial compartment osteoarthritis.1,2 It reduces pain, improves the function of individuals and retains the native knee joint. 3 The aim of the HTO is to transfer weight-bearing loads to the relatively unaffected lateral compartment in the varus knee. This is achieved by correcting the weight-bearing axis into a slight valgus. 4 Despite good early and mid-term outcomes, HTO is known to fail with time due to progression of osteoarthritis or loss of correction angle.5–7 Registry and cohort studies report that about 24% of HTO fail after 10 years, requiring subsequent total knee arthroplasty (TKA).8–10
The literature on the functional outcomes and survivorship of TKA after HTO is mixed. Some authors suggest that prior HTO has minimal impact on the outcome of subsequent TKA. Haddad et al. reported excellent and comparable midterm outcomes when comparing TKA after HTO with primary TKAs. 11 Meding et al. observed no difference in Knee Society Scores, pain scores, range of motion and radiographic alignment between TKA with or without previous HTO. 12 Others however have reported technical challenges11,13 as well as inferior outcomes.14,15 Niinimäki et al. using registry data, compared 1036 TKA after HTO with primary TKAs and reported poorer mean survivorship in TKA performed with prior HTO compared to primary TKA (95.3% versus 97.2% at 5 years, 91.8% versus 94.5% at 10 years, and 88.4% versus 90.6% at 15 years respectively). 14
Alignment failures after HTO may be a factor influencing clinical outcomes of subsequent TKA. Failure in a varus HTO alignment may result in metaphyseal bone loss and medial sided contractures – making subsequent TKA technically challenging. HTO that fail in valgus may have greater longevity owing to successful transfer of weight-bearing axis. However, TKA of valgus knees post-HTO may result in poorer patellofemoral tracking and peroneal nerve injuries. Existing literature offers little insight into the impact of the different HTO alignments and its influence on subsequent TKA.
Our study aims to study the influence of HTO alignment on HTO survivorship. In addition, compare the clinical outcomes of TKA after prior HTO in varus, neutral and valgus alignments. The authors hypothesize that HTO in varus alignment tend to have shorter time to TKA. The authors assume the null hypothesis that subsequent TKA clinical outcomes are comparable regardless of alignment failure.
Methods
The retrospective study was approved by the hospital’s ethics committee (CIRB 201908-00042) and carried out in accordance with the ethical standards established in the 1964 Declaration of Helsinki.
A single centre retrospective review was performed between 2001 and 2014, 269 patients underwent TKA after previous closing-wedge HTO and completed the routine 2 years post-operative follow up. Patients who lacked pre-operative radiographic data (n = 52), had TKA to the contralateral knee to the HTO side (n = 40), had medial opening-wedge HTO performed (n = 6), had unicompartmental knee arthroplasty performed (n = 1), or who were lost to follow up (n = 11) were excluded from this study. TKA was offered to all patients who were symptomatic of knee osteoarthritis and have failed at least 6 months of prior conservative treatment.
The remaining patients (n = 159) were divided into 3 separate groups based on their coronal alignment deformities – varus, neutral and valgus. Varus alignment (VrA) (n = 99) was defined as having a pre-operative femoral tibial angle (FTA) of less than or equal to 3o valgus, neutral alignment (NA) (n = 35) as pre-operative FTA of 3 – 9o valgus, and valgus alignment (VlA) (n = 25) as pre-operative FTA of more than or equal to 9o valgus.16–18 Prior closing-wedge HTOs were performed using staples in 36% (n = 57) of cases and with plates and screws in 64% (n = 102) of cases.
Surgical technique
Removal of HTO implant was performed through the old HTO scar. The authors then proceeded to perform TKA through a midline incision and performed a medial parapatellar arthrotomy.2,19 Should the patella be at risk of avulsion, a pin was placed in the tibial tubercle to further protect the patellar tendon. Standard femoral preparation and bony cuts were performed with 3° of external rotation off the transepicondylar axis. Gap balancing technique was applied to establish a symmetrical and rectangular flexion gap once bony cuts are completed. The proximal tibia was prepared using an extramedullary cutting jig perpendicular to the mechanical axis of the tibia. The thinnest possible cut was employed to enable stable cementation of tibial implants. Tibial cuts were aimed at maintaining knee alignments at slight valgus. Technical considerations were similar to those described by Chen et al. 2 All cases were performed with a fixed bearing cruciate retaining (CR) implant planned. In cases with ligamentous imbalance or posterior cruciate ligament (PCL) compromise, a posterior stabilising (PS) polyethylene insert was used instead.
Post-operatively, patients underwent standard post-operative TKA protocol at the institution. Patients worked with an inpatient physiotherapist on post-operative day (POD) one doing bed exercises consisting of hamstring stretches, knee flexion and quadriceps activation exercises. Patients also practiced sit to stand exercises and if confident, attempted ambulation with a walking aid under supervision by the physiotherapist. POD 2 and three focused on building on exercises taught on POD 1 with the additional goal of attempting stair climbing. Once successful with stair climbing, the patient was then assessed by the physiotherapist for safety upon discharge. Those deemed safe to care for themselves continued their care at home, whilst those who required further care continued their rehabilitation in the setting of a community hospital. Patients were followed up in the specialist outpatient setting at 2 weeks, 3 months, 6 months and 1 year and 2 years from the date of surgery.
Radiographic measurements were carried out for the pre-TKA FTA which was defined as the medial angle between the anatomical axis of the femur and tibia on weight-bearing lower limb radiographs.18,20,21 FTA was measured on weight bearing knee radiographs using the technique described but Ishii et al. 22 Measurements were made to the nearest 0.1o and were recorded on two separate occasions by two reviewers who were blinded to the outcome measures. Coronal plane measurements were studied and inter-rater reliability was 0.80, p < .001 and intra-rater reliability was 0.93, p < .001. An independent assessor, a trained senior physiotherapist at the institution, followed up the patients pre-operatively and at 6 months, 1 year, and 2 years post-operatively. Knee Society Function Score (KSFS), Knee Society Knee Score (KSKS), modified Oxford Knee Score (OKS) as well as the Physical Component Score (PCS) and Mental Component Score (MCS) of the Short Form-36 Questionnaire (SF-36) were used to record pre-operative and post-operative functional scores.
This study used the 200-point scoring system by the Knee Society with 100 points for the KSFS and 100 points for the KSKS. 23 This study also used the modified Oxford Knee Score, as recommended by Murray et al., whereby a score of 48 out of 60 is best and a score of 0 being the worst. 24 Quality of life was assessed using the physical and mental components of SF-36. 25
Statistical analysis
A power analysis was conducted prior to the commencement of the study, based on the known minimum clinically important difference (MCID) of OKS. To detect a difference of 5 points in OKS from a mean of 37 and a standard deviation of 8, a sample size of at least 19 patients in each group will be required to achieve a power of 0.80. This calculation was done for a two-sided test with a type I error of 0.05.
For statistical analysis, normality testing was done with the Shapiro-Wilk test. The one-way ANOVA with Bonferroni post-hoc test was used for continuous variables with normal distribution (e.g. time to TKA, KSFS, KSKS, OKS, SF-36, range of motion). Pearson’s chi-squared test was used for categorical variables (e.g. Gender, side of surgery). Analyses were performed using SPSS version 23.0 (SPSS, Inc, an IBM Company, Chicago, IL), and p ≤ .05 was considered significant.
Results
Patients’ demographics.

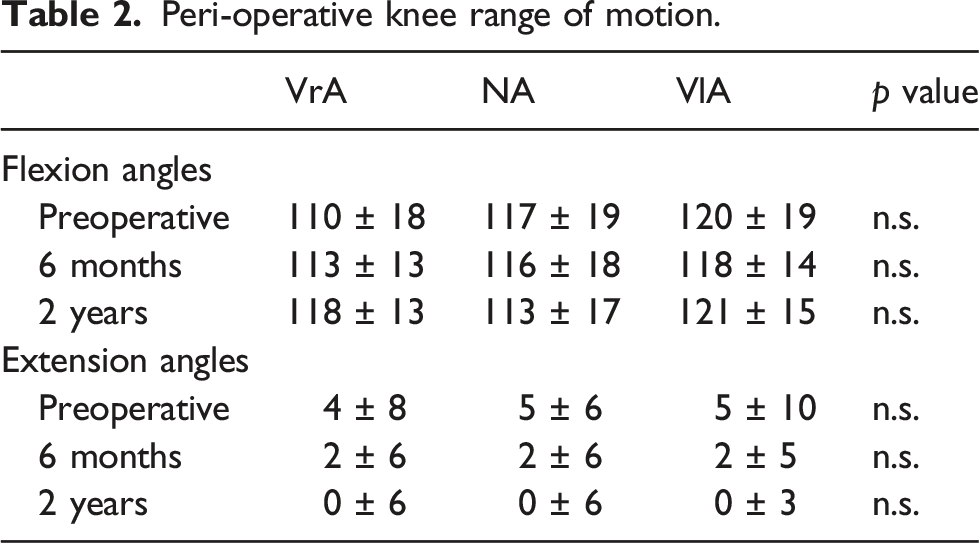
Peri-operative knee range of motion.
Functional outcome scores for VrA, NA, and VlA patients.
Radiological parameters for VrA, Na, and VlA patients.

Abbreviations: High tibial osteotomy (HTO); Femoral tibia angle (FTA); Caton-Deschamps index (CDI).
In the 2 years of follow up post-TKA, there was 1 case of wound infection in the VrA group, and 1 case of septic arthritis in the VrA group and NA group respectively.
Discussion
The main findings of this study were, 1 the mean time interval to TKA after HTO is 12 years, regardless of HTO alignment; 2 Whilst VrA patients had poorer pre-operative KSKS, 3 all groups studied had comparable range of motion, clinical and radiological outcomes at 2 years after TKA. 3 Half of patients that failed in varus were originally under-corrected post-HTO.
In this study, the duration of time till TKA surgery was similar between the patient groups as well as existing literature. Odenbring et al. showed that 2 out of three patients had TKA at 13 years because of under-correction. 26 Similarly, Chalmers et al. demonstrated a mean time interval of 13 years between HTO and TKA. 27 Filho et al. showed that the mean time from HTO to TKA was 12 years 28 This is consistent with what we have seen in our study. However, there are papers which have reported shorter time intervals of 5–7 years before TKA surgery.5,15,29 This difference can be explained by the aforementioned articles dealing with selected patients. Haslam et al. and Staeheli et al. both included patients with previous surgeries on their knees prior to the HTO procedure.5,29 Erak et al. included older patients, with a mean age of 57 years, which has been shown to be a risk factor for TKA. 15 Similarly, Chalmers et al. performed a multivariate analysis and reported patients under the age of 60 years were at a higher risk of requiring subsequent conversion to TKA post-HTO (p = .04). 27
Patients who fail in varus alignment had significantly inferior pre-operative KSKS scores. There is an inherent bias when using KSKS to compare between groups with deformities. Alignment is a component of the KSKS scoring system and deviations from neutral negatively influences the score. 23 This is evident as other pre-operative outcome measures showed no statistical difference. Nevertheless, under-corrected HTOs fair poorer compared to neutral or valgus knees within literature.30–34 A previous study by El-Azab et al. on 50 open-wedge HTOs showed inferior Lysholm-Gillquist scores in under-corrected knees as compared to accurately corrected and over-corrected knees at 36 months post-operatively. 30 Under-correction, which can occur due to ligamentous laxity and neglect of weight-bearing effects on the mechanical axis of the lower limb, has been shown to lead to varus recurrence and pain reoccurrence.31,32 Furthermore, the degree of varus alignment is linked with the severity of medial compartment osteoarthritis. 35 Varus recurrence has also been linked with high knee adductor moments.33,34,36,37 Prodromos et al. showed that patients who had lower pre-HTO knee adductor moments had better clinical outcomes post-HTO compared to patients with higher pre-HTO knee adductor moments who tended to revert back to varus alignment. 38
Majority of the patients in our study failed in varus alignment. This is consistent with another study by Erak et al. which showed that 22 out of 34 knees (64.7%) failed in varus alignment post-HTO.15 A previous study on closing-wedge HTO by Shaw et al. attributed the high number of varus recurrence to 2 factors. 39 Firstly, osteotomy angles more than 10o resulted in the lateral collateral ligament being non-functional, therefore allowing the knee to swing back to its native alignment with varus loading. Secondly, shifting the mechanical axis to result in increased lateral joint loading required large angular changes that was deemed aesthetically and functionally unacceptable to most patients, therefore making HTOs prone to under-correction and reverting back to varus alignment. Insall et al. reported nearly one-third of their patients reverting back to varus alignment post-HTO and this was not just restricted to under-corrected patients. 40 Matthews et al. reported 7 out of 40 patients (17.5%) reverting back to varus alignment post-HTO. 41 In our study, half the patients in the VrA group were under-corrected and the other half, adequately corrected post-HTO. This finding is consistent with existing literature, suggesting a significant proportion of patients do continue to revert to varus alignment post-HTO.
Only patients with lateral closing-wedge osteotomy were studied. One of the disadvantages of closing-wedge osteotomy is that it affects the proximal tibiofibular joint and lateral collateral ligament, therefore resulting in higher adductor moments, and higher possibility of persistent lateral tibial thrust.42,43 A study by Duivenvoorden et al. showed a significantly higher proportion of closing-wedge HTO patients needing TKA at 6 years post-HTO compared to opening-wedge HTO. 44 92 patients were randomized to closing-wedge HTO and opening-wedge HTO; 10 (22%) closing-wedge HTO patients needed TKA compared to 3 (8%) opening-wedge HTO patients (p = .05). However, a meta-analysis by Kim et al. showed no difference in the survivorship of opening- and closing-wedge osteotomy at 5 years 42 Performing TKA after previous HTO can be technically more challenging due to distortion of normal tibial anatomy.4,45 In closing-wedge HTO, the distance between the tibial tubercle and joint line is decreased, therefore resulting in increased difficulty in exposing the proximal tibia and eversion of the patella. 6 Conversely, opening-wedge HTO can shorten the length of the patella tendon above the joint line and cause increased posterior tibial slope, which commonly requires restoration during TKA. 6 Despite TKA being more challenging and VrA patients having inferior clinical pre-operative scores, the clinical scores were comparable among all groups of patients 2 years after TKA. The improvements in the clinical score in VrA patients post-TKA might be explained by meticulous surgical techniques aimed at correcting deformity, balancing, and restoration of the joint line height and patella height through the use of appropriate prostheses and polyethylene inserts with sufficient thickness.6,46
There was no difference in range of motion among all three groups of patients after TKA. Only VrA patients had significant improvements for both knee extension and flexion. The lack of overall improvement in range of motion across all patient groups post-TKA is also demonstrated by a previous study by Amendola et al. which showed that the mean knee range of motion was 101o before and after TKA for HTO patients at an average follow up of 36 months 3 These results are similar to the study by Nizard et al., which showed the range of motion in HTO patients was 100.6o compared to 103.2o post-TKA at a mean follow up of 4.6 years 47 This is in contrast to Kazakos et al. which showed significant improvement in flexion and extension post-TKA after a mean follow up time of 7.3 years 48 Chalmers et al. also showed significantly improved mean knee flexion post-TKA from 104o to 112o post-operatively at a mean follow up time of 8 years in 207 patients (27). Patients in our study were followed up at 2 years and we believe this could be a contributing factor in the lack of overall improvement in range of motion across all three groups of patients. Despite the lack of overall improvement in range of motion post-TKA, clinical outcomes and radiographical parameters significantly improved post-TKA. A multivariate analysis had previously shown that the success of TKA correlated more with overall function than range of motion. 49
The clinical implications of this study include that mean survivorship of closing-wedge HTO in this cohort is 12 years, regardless of HTO alignment. In addition, this is the first study investigating the impact of HTO alignment on the clinical and radiological outcomes of subsequent TKA. Whilst alignment differences did not negative impact TKA outcomes, patients with prior HTO who fail in varus had significantly poorer outcomes.
There are limitations to this study. Firstly, the design of this study was retrospective in nature. In addition, this study was from a single institution and focused on a specific cohort of patients and therefore may be subject to selection biases. Future prospective studies, matched-paired with a control group of primary TKA may offer better comparisons. Secondly, this study focused on coronal alignment after HTO on its impact on subsequent TKA. Sagittal plane alignment such as tibia slope was not studied and should be an area for further evaluation in the future. In addition, this study reports early clinical outcomes of TKA after HTO failure. A future long-term follow up study for this cohort of patients is warranted as it will shed greater insight onto the effect of HTO alignment on the survivorship and long-term clinical outcome on TKA. Nevertheless, this study is adequately powered and follows a large cohort of patients who underwent HTO and required subsequent conversion to TKA.
Conclusion
The mean time interval to TKA surgery after HTO was 12 years, regardless of HTO alignment. Coronal alignment of prior HTO does not impact early range of motion, clinical or radiological outcomes of subsequent TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the FY2017 Singhealth Duke-NUS Musculoskeletal Sciences Academic Clinical Programme Research Support Programme Grant under the Nurturing Clinical Scientist Scheme (NCSS) (13/FY2017/P1/16-A30).