
Abstract
Slow recovery after hip fracture has been associated with negative consequences. Thus, there is medical need to improve healing and functional recovery after intertrochanteric fracture. The aim of this study was to measure whether short-term teriparatide would improve healing in intertrochanteric fractures after internal fixation as measured by (1) clinical scores, (2) radiographic fracture healing, and (3) complication rates. We retrospectively reviewed 96 patients (average age, 82 years) who underwent closed reduction and internal fixation with proximal femoral nail (PFN) for unstable intertrochanteric fractures between 2014 and 2016. Of the 96 patients, 56 patients were treated with a PFN alone (group 1). These patients were compared with 46 patients for whom the same device was used and a weekly subcutaneous injection of PTH 1-34 (teriparatide) was prescribed postoperatively (group 2). Questionnaire surveys or telephone interviews were conducted, and patients completed a self-report Harris hip score and visual analog scale scores. The radiological time to fracture healing was assessed as the primary end point. Postoperative complication rates were compared. Functional outcomes at 6 months after surgery were similar in both groups. There were no differences between groups in the proportion of patients achieving radiographic fracture healing. The frequency of patients reporting adverse events was 20% (10 of 50) in group 1 versus 17% (8 of 46) in group 2 (p = 0.744). Short-term teriparatide did not improve radiographic signs of fracture healing of an intertrochanteric fracture and reduce the incidence of complications. The effect of teriparatide on fracture healing remains uncertain. Further multicenter prospective studies are needed to demonstrate objective long-term results of parathyroid hormone therapy in patient with hip fracture.
Level of Evidence:
Level IV, therapeutic study.
Introduction
Approximately 4 million hip fractures are projected to occur worldwide in 2025. 1 With the advancing age of the general population, complications during bone healing due to inadequate fixation cause a significant consumption of the resources of the health-care system. In patients with severe osteoporosis, loss of proximal fixation or cutout can occur when adequate fixation is not achieved in the femoral head. 2 For nonunion, a second intervention will undoubtedly be necessary, carrying additional risks and potential complications as well as increases in health-care costs. Thus, there is medical need to improve healing and functional recovery after intertrochanteric fracture.
Parathyroid hormone (PTH) and its amino-terminal fragments have been shown to increase bone mass, increase bone strength, and reduce bone loss. 3 Teriparatide is a recombinant form of the biologically active component of human PTH and has been shown to stimulate osteoblasts, enhance bone connectivity, increase endosteal cortical thickness, and improve bone mineral content. 4 Teriparatide enhanced bone healing in preclinical models 5 and, in a controlled clinical trial, accelerated radiographic healing of fractures in humans. 6 Published case reports and systematic review suggest that long-term daily teriparatide accelerates bone healing and improves functional recovery after fracture at various skeletal sites including the hip. 7 However, to the best of our knowledge, few studies have evaluated whether the administration of short-term weekly subcutaneous PTH could improve radiographic signs of fracture healing of unstable intertrochanteric fractures treated with intramedullary (IM) nailing.
The purpose of this study was to evaluate whether the administration of short-term PTH could improve early postoperative outcomes including clinical scores, radiographic fracture healing, and complication rates. Our hypothesis was that postoperative teriparatide treatment could improve functional recovery after a trochanteric hip fracture through the mechanism of accelerated fracture healing.
Methods
The institutional review board of the ethics committee of our institution approved this retrospective comparative study (HIRB-2016-009). Informed consent was waived as this was purely retrospective review without intervention.
Subject cohorts
Between 2014 and 2016, we retrospectively assessed 104 patients who underwent reduction and internal fixation with a short femoral nail for unstable intertrochanteric fractures. We were unable to assess eight patients because three patients were lost to follow-up, three patients didn’t have adequate follow-up radiographs and postoperative functional scores, and two patients died. The final study groups were 96 patients (96 hips). Inclusion criteria were (1) age more than 65 years, (2) patients who were classified as unstable femoral intertrochanteric fractures (AO/OTA type A2, A3 8 ), (3) patients with osteoporosis (T-score of −2.5 or lower), and (4) patients who underwent reduction and internal fixation with a short IM nail. Exclusion criteria were (1) serious concomitant illness, mental instability, or musculoskeletal deficiency which limited the ability to perform objective functional tests; (2) known malignancy within 5 years before the fracture; (3) patients who had multiple fractures that would affect the postoperative functional outcome; and (4) patients who underwent reduction and internal fixation with a sliding screw Dynamic hip screw (DHS).
Most patients underwent dual-energy X-ray absorptiometry (DXA) scans prior to operation with preoperative computed tomography (CT) evaluation. For the patients with severe acute pain, DXA scans were delayed and performed postoperatively. The different osteoporosis medications, the advantages, and disadvantages of osteoporosis treatment based on the guidelines for osteoporosis treatment 9 were explained to the patients and chosen by the patients themselves. Of the 96 patients, 50 patients were treated with a proximal femoral nail (PFN; Proximal Femoral Nail Antirotation (PFNA), AO synthes) alone (group 1) without any other anti-osteoporosis treatment. These patients were compared with 46 patients for whom the same device was used and a weekly subcutaneous injection of 56.5 μg teriparatide (PTH 1-34, Teribone) was prescribed postoperatively for 8 weeks (group 2). Patients were prescribed teriparatide as suggested by the guidelines for osteoporosis treatment and was prescribed from the day of surgery. 9 The average age of the patients at the time of surgery was 82 years (range 65–99 years). There were 44 males and 52 females. Minimum follow-up was 1 year (average 1.9 years; range 1–2.8 years). There was no statistical difference between the two groups in terms of age, gender, affected hip, and osteoporosis at the time of fracture (Table 1).
The preoperative demographic data for groups 1 and 2 (group 1, placebo group; group 2, teriparatide group).

BMD: Bone mineral density.
All procedures were performed at one institution by a single surgeon. All patients underwent surgery under general anesthesia. At operation, the fracture was anatomically reduced. After reduction of the fracture, a PFNA was inserted using the standard technique. The postoperative protocol was uniform for all patients. Weight-bearing with a walker was allowed within the first 2 weeks after surgery and continued for at least 8 weeks. Subsequently, patients could be advanced to full weight-bearing on the basis of the appearance of recanalization or bridging callus on follow-up radiographs. Patients were seen for follow-up at 4, 8, 12, 16, 20, and 24 weeks and then every 6 months thereafter, with clinical and radiographic evaluations.
All patients were seen by the authors at outpatient clinic and examined for any signs of complications after surgery. Clinical assessments were performed with use of the Harris hip score (HHS) 10 and visual analog scale (VAS) 11 scores (pain and stiffness were scored by the patients on a VAS of 0–100, with 100 representing maximum pain or stiffness) at the final follow-up. Questionnaire surveys or telephone interviews were conducted, and patients completed a self-report HHS and VAS scores. Any complications were noted. All data were obtained from medical records and radiographs. Patient rights are protected by a law that requires patients to be informed at the time of examination about the possibility that their medical records and radiographs will be reviewed for scientific purposes.
Imaging
All radiographs were measured using StarPACS PiView STAR 5.0.6.0 software (Infinitt Healthcare Co, Seoul, Korea). The primary outcome comprised radiographic findings of fracture healing and callus formation at each follow-up. Radiological union was defined as bridging at the fracture site by a callus or a cortical continuity involving at least two cortices in the hip using anteroposterior and lateral views of the femur. 12,13 Malunion was defined as varus collapse of more than 15° after comparison with the opposite side. 14 All the radiographs were studied by two observers and were tested for concurrence and reproducibility by interobserver studies. The persons who assessed the outcomes were completely blinded to group assignment.
Statistical analysis
Data were recorded using Microsoft® Excel® 2007 version (Microsoft Corp., Redmond, Washington, USA) and analyzed using SPSS® software (SPSS Inc., Chicago, Illinois, USA). Various radiographic indices (radiologically defined union) were described by a mean ± standard deviation (SD). Student’s t-test was used to compare the clinical parameters of group 1 to those of group 2. The χ 2 test was used to compare the radiological assessment (fracture healing times) with the treatment given and to evaluate differences in the complication rates between groups. A subgroup analysis of the outcomes of patients with severe osteoporosis (T-score less than −3.0) was also performed separately to evaluate whether there is a difference in the clinical and radiographic outcomes. Significance was reported at the 95% confidence level (p < .05). Radiographic parameters were tested for reproducibility by intra- and interobserver studies using Pearson correlation coefficients; correlation coefficients ranged from 0.886 to 0.912, indicating good reliability.
Results
At the final follow-up, the HHS average scores were 62.2 and 65.4, in groups 1 and 2, respectively, and the difference between the two groups was not statistically significant (p = 0.515). Also, VAS pain and VAS stiffness scores at 6 months after surgery were similar in both groups (p = 0.331 and p = 0.346, respectively) (Table 2). It seemed that VAS stiffness score was higher in group 2 at the time of the final follow-up but did not reach statistical significance.
Clinical outcomes for groups 1 and 2 (group 1, placebo group; group 2, teriparatide group).
HHS: Harris hip score; VAS: visual analog scale.
Postoperatively, the mean time to radiologically defined union was 12.7 weeks (SD 6.1) and 12.3 weeks (SD 6.4) in groups 1 and 2, respectively (p = 0.562). There was no difference between two groups with respect to radiographic fracture healing at the final follow-up (Table 3). Fractures in group 2 showed a tendency to heal sooner, but this was not statistically significant compared with group 1. There were no cases of nonunion or avascular femoral head necrosis.
Fracture healing times for groups 1 and 2 (group 1, placebo group; group 2, teriparatide group).

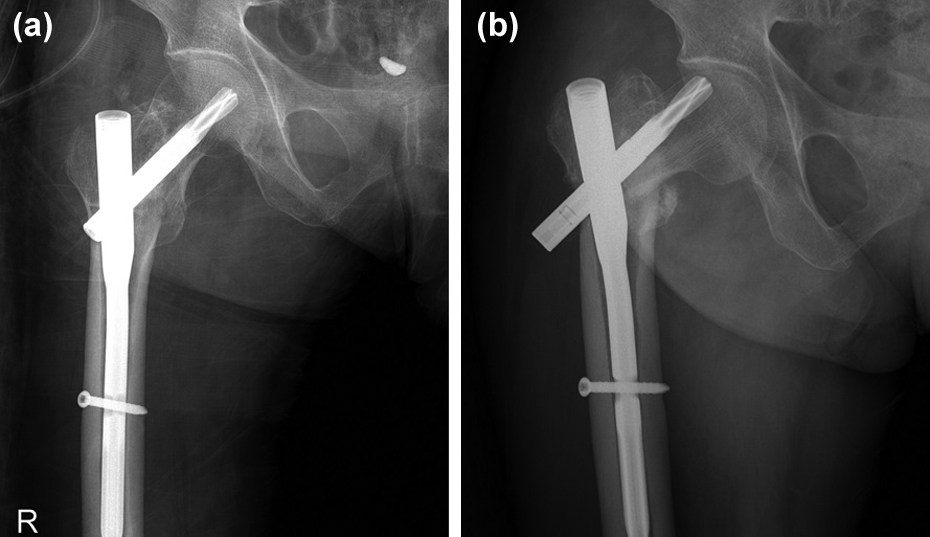
A total of 10 complications were encountered in group 1 and 8 complications in group 2. The rates for total complications were 20% in group 1 and 17% in group 2. This result was not significant (p = 0.744) (Table 4). Excessive screw sliding occurred in one patient in group 1 and one patient in group 2, who required further intervention because of severe skin irritation (screws were exchanged) (Figure 1). Loss of reduction with screw sliding occurred in two patients, who were reoperated for a bipolar hip replacement (Figure 2). No implant failure or cutting out of the lag screw was observed in both groups.
Postoperative complications for groups 1 and 2 (group 1, placebo group; group 2, teriparatide group).


(a) Postoperative AP radiograph shows that the fracture was well reduced and fixed with an IM nail. (b). Excessive screw sliding occurred in the PTH group after 2 months. AP: anteroposterior; IM: intramedullary; PTH: parathyroid hormone.
(a) Immediate postoperative radiograph shows that the fracture was well reduced and fixed with an IM nail. (b) Excessive screw sliding and loss of reduction of fracture were noted at 2 months after surgery in the control group. IM: intramedullary.
According to the analysis of the outcomes of patients with severe osteoporosis, functional outcomes at 6 months after surgery were similar in both groups (Table 5). The mean time to radiologically union was 12.9 weeks (SD 6.6) and 12.1 weeks (SD 6.4) in groups 1 and 2, respectively (p = 0.146). The frequency of patients reporting adverse events was 22% (7 of 32) in group 1 versus 16% (5 of 30) in group 2 (p = 0.604).
The outcomes of patients with severe osteoporosis (T-score less than −3.0).

HHS: Harris hip score; VAS: visual analog scale; SD: standard deviation.
Discussion
As hip fractures represent the most costly fracture with large socioeconomic costs, 15 there is a medical need for therapies that improve hip fracture healing. If a pharmacological therapy could improve hip fracture healing, this may reduce the number of revision surgical procedures and potentially improve other aspects important for recovery, such as early ambulation. The purpose of this study was to evaluate whether the administration of short-term PTH could improve early postoperative outcomes including clinical scores, radiographic fracture healing, and complication rates in intertrochanteric fractures.
Park et al. 16 reported that most of the patients treated with teriparatide showed significant symptom improvement within approximately 2 or 3 weeks, which is quite rapid compared with conventional conservative treatment with only pain management and bracing after vertebral compression fracture. However, statistical analysis of the changes in clinical symptoms was not performed in the study. Tu et al. 17 demonstrated that teriparatide therapy significantly decreased VAS pain scores and increased functional scores but suggested that therapy should continue for at least 6 months to ensure it is effective. However, because PTH treatment is more expensive than other treatments and subcutaneous injection remains the only licensed route of administration, 18 the greatest challenge of delivering this study was that of identifying a sufficient number of eligible patients. For these reasons, we couldn’t recommend the use of injection therapy for patients over 2 months. The dose, duration, and cost-effectiveness of treatment remain in question. 19 In the present study, major differences between groups regarding the functional end points were not observed. Short-term teriparatide didn’t improve functional score and decrease pain compared with the placebo.
There have been many confusing reports about the effect of PTH on bone healing. Animal experiments show a dramatic improvement of radiological skeletal repair by teriparatide. 5,20,21 Andreassen et al. 22 reported that PTH improves rate of callus formation and bone strength even in older bone in aged rats at 3 and 8 weeks after fracture. Positive effects on femoral fractures have been demonstrated also in Cynomolgus monkeys, where a treatment twice per week for 3 weeks led to a healing process with a higher mineralization and better mechanical properties. 23 The lack of valid studies on fracture healing in humans is a direct consequence of the difficulties that are present in monitoring the healing process in human, both for the frequency of the controls and the difficulty in measure the healing process, radiographically or clinically. 24 The effects of teriparatide on normal primary fracture in human subjects have been examined. 6 Systemic therapy with teriparatide has been shown to improve healing in clinical studies of wrist fractures, 6 pubic bone fractures, 25 and in case reports. 26 On the contrary, according to a recent randomized placebo-controlled study, 27 teriparatide did not improve radiographic signs of fracture healing or decrease pain compared with the placebo after femur neck fracture fixed with multiple cancellous screws. However, the authors tried to evaluate the effect of long-term daily teriparatide (20 μg/day) for 6 months versus placebo after femur neck fracture. Johansson 28 also reported that there were no radiographic signs of enhanced healing or improved clinical results in the group treated with short-term (4 weeks) daily teriparatide (20 μg/day) in proximal humerus fractures. In the present study, we have evaluated whether the administration of short-term weekly PTH (56.5 μg/week), which was prescribed postoperatively for 8 weeks, could improve radiographic signs of fracture healing of intertrochanteric fractures treated with IM nailing. There continues to be anecdotal evidence for the use of recombinant PTH to enhance fracture healing. 29 In our study, although fractures in group 2 showed a tendency to heal sooner after surgery, there was no significant difference between two groups with respect to radiographic fracture healing at the final follow-up. We couldn’t confirm that radiographic outcomes of intertrochanteric hip fractures were improved even in the patients with severe osteoporosis treated with teriparatide. Reasons for the lack of treatment effect are speculative. Possibly, the treatment duration was too short to have a treatment effect in this context or the sample size was too small to detect a difference in plain radiographs obtained at the selected intervals. Measurements of the X-ray cannot be so accurate, and this will also reduce the importance of the difference. 30 Further multicenter studies are needed to demonstrate objective long-term results of PTH therapy in patient with fracture before this method attains widespread use.
Varus collapse or excessive shortening of a limb are common postoperative complications in unstable three- and four-part trochanteric fractures because of pronounced impaction of the fracture. 31 Bhandari et al. 27 recently reported that the proportion of patients undergoing revision surgery after femoral neck fracture at 12 months was 14% (11 of 81) in the placebo group versus 17% (13 of 78) in the teriparatide group and teriparatide did not decrease the risk of revision surgery. Similarly, in the present study, there was no between-group difference in the proportion of patients undergoing revision surgery at 1 year with the numbers available. On the other hand, although the side effects are mild, it has been reported that adverse events including nausea, sweating, and headache can occur after teriparatide injection in human without enhancing bone healing. 28 In addition, another major concern about PTH therapy is cost-effectiveness. Definitely, teriparatide is expensive and may produce a smaller increase in quality-adjusted life year. It could become more cost-effective if short courses of teriparatide could provide the same fracture reduction efficacy as those reported in longer clinical trials. 32
Our study has some limitations. First, since our study is a retrospective review with a small population, the conclusions from the results are limited. Because the cohort size was smaller than planned, the studies were substantially underpowered to detect the treatment effect included in the original study protocols. This is not unexpected in frail, elderly subjects with a hip fracture, and it stresses the difficulties of performing randomized clinical trials involving frequent, cumbersome postoperative assessments. Second, although we attempted to make the two groups as equivalent as possible in age and gender structure and average pretreatment score, there may be certain dissimilarities in the two groups such as the quality of the reduction, fixation, and implant positioning which is known to have a bearing on the outcome of surgery.
In conclusion, with the patients available, short-term teriparatide did not decrease pain, improve radiographic signs of fracture healing, or decrease postoperative complication rate compared with the placebo in intertrochanteric fractures. The effect of teriparatide on fracture healing in humans remains uncertain. The possible benefits of PTH cannot be ruled out for this group of patients if treated with a different regime or for other types of fractures. Additional randomized placebo-controlled trials are needed to determine the potential benefit of PTH as an adjunct to enhance fracture healing and its efficacy in broader populations with varying comorbidities and fracture types.
Footnotes
Author contributions
SJK and HSP contributed to the study design, carried out acquisition of the data, made the analysis, and interpreted the data. DWL and JWL had participated in conceiving the study design and revising the data and manuscript. All authors had read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.