
Abstract
Objective:
To observe the clinical effect of zoledronic acid (ZA) in patients with cervical spondylosis and osteoporosis after anterior cervical discectomy and fusion (ACDF) surgery.
Methods:
All selected patients were divided into the study group and the control group according to the sequence of surgery time. In the study group, 5 mg (100 ml) of ZA was applied intravenously as intervention on the 5 day after ACDF surgery. Patients were followed up regularly after surgery.
Results:
Forty-three cases completed the follow-ups (21/22), the neck disability index (NDI) score significantly decreased at the 3rd month after surgery in both groups, it came to a plateau at the 6th month after surgery, and it had some rise at the 12th month after surgery, but the NDI score was lower in the study group at the 12th month after surgery (p < 0.05). C-telopeptide of type I collagen (CTX) and amino terminal propeptide of type I procollagen of bone turnover markers in the study group showed a downward trend after surgery, among which CTX decreased significantly and no significant changes in the control group. At the 12th month after surgery, the bone mineral density of lumbar spine area in the study group was significantly improved (p < 0.05). During the 3rd and the 6th month follow-up after surgery, 1/2 osteogenesis rate of the study group was significantly higher (p < 0.05). However, all patients in the two groups obtained stable fusion at the 12th month follow-up after surgery.
Conclusions:
For patients with cervical spondylosis and osteoporosis, intravenous application of ZA after ACDF surgery can shorten the time of cervical osteogenesis, promote local bone graft fusion, and improve the postoperative clinical effect to some extent.
Introduction
With the acceleration of the aging society worldwide, the incidence of diseases related to aging is increasingly high, and the number of elderly patients with primary osteoporosis is increasing, which has posed a serious threat to human health. Elderly patients with osteoporosis are easy to suffer from spinal degenerative diseases. One of the common diseases is cervical spondylosis, and the combination of two diseases would increase the difficulty for treatment. The classification of cervical spondylosis is complex, and surgery is often required for obvious compression of nerve root or spinal cord (cervical spondylotic radiculopathy, cervical spondylotic myelopathy) and poor conservative treatment. The objectives of the surgery include decompression, reconstruction of cervical spine stability, and bone graft fusion, whether bone graft is fused or not will directly affect the clinical effect of surgery.
Zoledronic acid (ZA) is a bisphosphonate drug, which is often used in combination with other drugs (calcium, ossiparol, etc.) for anti-osteoporosis treatment in patients with osteoporosis. However, there is some dispute on the appropriate application after cervical fusion surgery for patients with cervical spondylosis and osteoporosis and its effect on local bone graft fusion of the cervical spine. The current results of animal and clinical studies are not completely consistent. In this study, we selected patients with cervical spondylosis and osteoporosis as the study objects and used a randomized controlled study to explore whether the intravenous application of ZA after anterior cervical discectomy and fusion (ACDF) surgery has an auxiliary therapeutic effect and its effect on local bone graft fusion.
Materials and methods
Patients’ data
Patients with cervical spondylosis who received ACDF surgery in Hunan Provincial People’s Hospital from June 2015 to June 2017 were selected as the subjects. All patients were diagnosed with cervical spondylosis (cervical spondylotic radiculopathy or cervical spondylotic myelopathy) before surgery and diagnosed with osteoporosis (T < 0−2.5 SD) by dual-energy X-ray examination. The patients were divided into two groups according to the sequence of surgery time, with the odd group as the study group and the even group as the control group. The study was completely voluntary and excluded patients who did not agree to participate. All patients were detailed about possible risks and precautions before enrollment, and all patients included in the study signed written informed consent. The study was reviewed and approved by the hospital’s medical ethics committee.
Exclusion criteria include (1) those who have used bisphosphonates in the past or are allergic to bisphosphonates; (2) patients diagnosed with secondary osteoporosis, such as osteoporosis that is secondary to adrenal gland, sexual gland, thyroid gland, parathyroid gland, and other endocrine metabolic diseases; (3) suffer from diseases that may affect bone metabolism at the same time, such as infection, tumor, trauma, and so on; (4) drugs that may affect bone turnover metabolism or renal function, such as parathyroid hormone, calcitonin, glucocorticoid hormone, estrogen, and so on, were used within 6 months before surgery; (5) patients with poor basic physical condition who cannot tolerate general anesthesia, such as heart failure, severe pulmonary dysfunction, liver and kidney failure, and other serious functional or organic diseases; and (6) patients who had other types of cervical spine surgery, such as anterior cervical corpectomy decompression and fusion, anterior cervical hybrid surgery, and posterior surgeries, were not included in this study.
Study methods
Diagnosis of primary osteoporosis, cervical spondylotic radiculopathy, and cervical spondylotic myelopathy
Dual-energy X-ray absorptiometry was the gold standard tool for measuring bone mineral density (BMD), we use South Korea Osteosys Dexxumt dual-energy X-ray BMD instrument to measure three parts, bilateral femoral necks and lumbar. All patients were using the same instrument operated by the same technician, roughly the same body position.
Diagnostic main points of cervical spondylotic radiculopathy: (1) typical symptoms include limited mobility and stiffness in the neck, neck unilateral pain, presents electric shock-like radiating from neck root to the shoulder, to upper arm and forearm and finger with numbness feeling, and so on. (2) Brachial plexus traction test positive, or holes among cervical vertebras extrusion test positive. (3) Computed tomography (CT)/magnetic resonance imaging (MRI) examination shows reduced cervical lordosis, protrusion of cervical intervertebral disc, and so on.
Diagnostic main points of cervical spondylotic myelopathy are as follows: (1) Typical symptoms include progressive lower extremity numbness, chills, pain, unsteady gait, trip over easily, patients may feel feet step on cotton, and so on. (2) Muscle tension increases, tendon hyperreflexia, and positive pyramidal tract signs. (3) CT/MRI examination shows constrictive segment spinal cord has signal changes, with wave-like pressure trace.
Operation indication and methods
Preoperative routine examinations included the anterior and lateral position of cervical vertebra, X-ray images of hyperextension and flexion position, three-dimensional (3D) CT reconstruction of cervical vertebra, and MRI plain scan. Definite diagnosis of cervical spondylosis was obtained before surgery, surgical indications (obvious compression or even denaturation of spinal cord or nerve root, invalid conservative treatment for 3 months, obvious instability or sliding of cervical vertebra) were matched, and all patients agreed to accept surgical treatment. All the patients in this study were operated on by the same treatment group. The surgical method was ACDF (Figure 1). All bone graft materials are homologous bone of the same source (Beijing Xinkangchen, China).
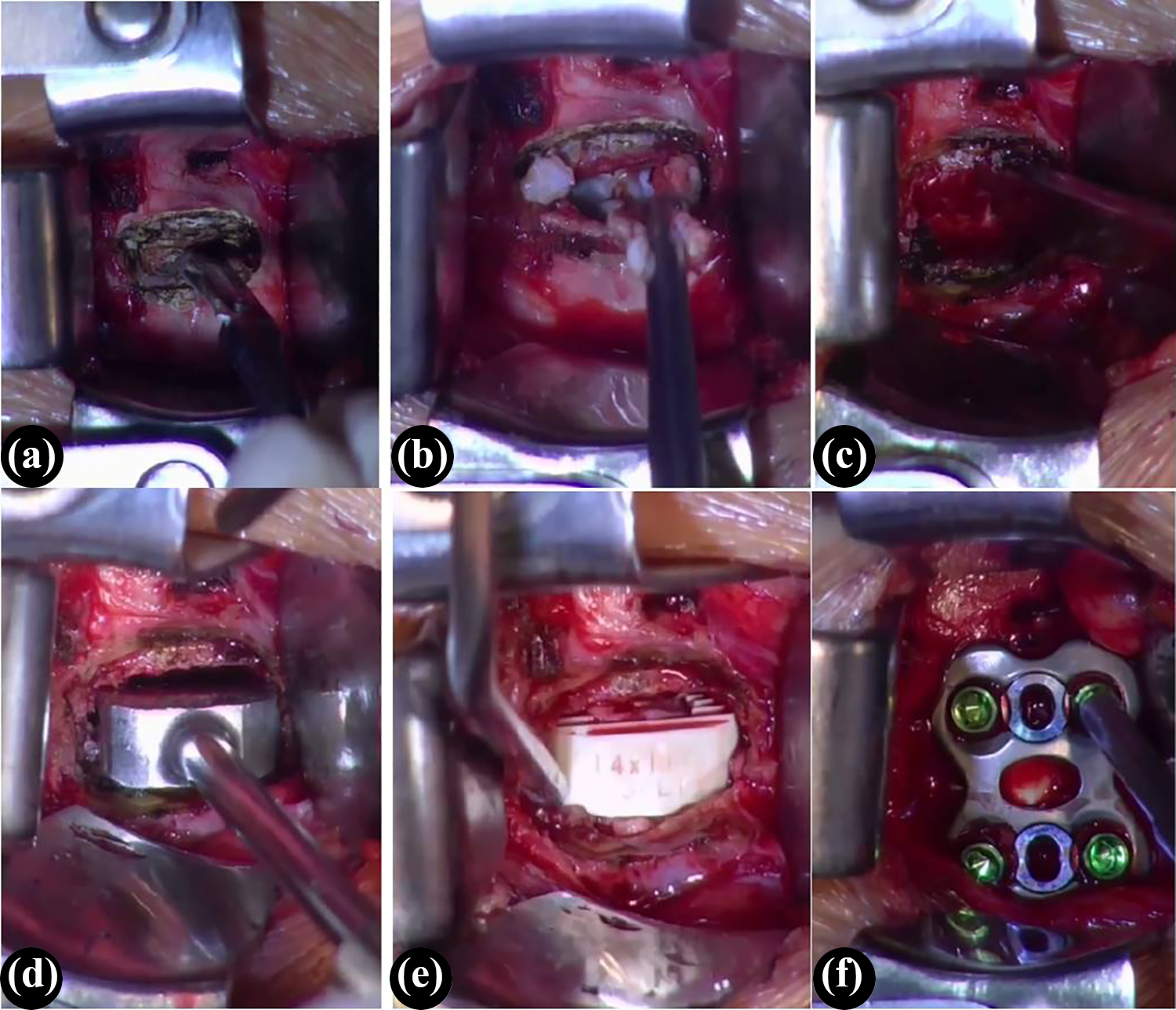
Surgical procedures of ACDF: After exposure, the target disc fibrous ring was incised (a); the intervertebral disc tissues were removed with a curette and nucleus pulposus forceps (b); laminectomy forceps were used to remove hyperplastic osteophytes (c); place a suitable trial in the intervertebral space (d); a cage which was the same size as the trial was inserted (allograft bone was filled in the center) (e); selected a titanium plate of suitable length, and fixed it to the upper and lower vertebrae with screws (f). ACDF: anterior cervical discectomy and fusion.
Postoperative anti-osteoporosis treatment program
Once-yearly intravenous infusion of 5-mg ZA had been proved safe and effective in patients with osteoporosis. 1 On the fifth day after surgery, the study group patients were given 5-mg ZA injection (Yigu, produced by Zhengda Tianqing Pharmaceutical Group, China), which was hydrated with 0.9% sodium chloride injection 500 ml before the infusion, and the intravenous infusion time was >30 min. For patients who have reactions such as fever, antipyretic and analgesic drugs are given for symptomatic treatment. At the same time, orally took Caltrate D3 (1.5 g of calcium carbonate and vitamin D3 125 international units per tablet) 2 tablets/day and Rocaltrol capsule (0.25 µg ossification triol per pill) 1 tablet/day combined with anti-osteoporosis treatment. The control group was given 100 ml of normal saline intravenous drip on the fifth day after surgery and received 2 tablets/day of Caltrate D3 and 1 tablet/day of Rocaltrol capsule. After discharge, the patients in the two groups continued to receive oral Caltrate D3 and Rocaltrol capsule. Smoking was prohibited in all patients 2 weeks before surgery and 12 months after surgery, regardless of whether or not they had smoked before.
During the whole experiment, the principle of randomness and double-blind was strictly observed. Patients were randomly assigned without knowing their group. When saline was used as a placebo, the specifications and appearance were exactly the same as that of ZA, while the nurses’ education of the two groups was also consistent.
Follow-up evaluation
Regular follow-up was conducted at the 3rd, 6th, and 12th month after surgery, and each observation included the neck disability index (NDI), bone resorption marker carboxy terminal cross-linked telopeptide of type-I collagen (CTX), bone formation marker amino terminal propeptide of type I procollagen (PINP), BMD measurement, cervical anteroposterior and lateral and functional X-ray film, and cervical 3D CT scan.
NDI scores are mainly used for the quantitative evaluation of the clinical effect of patients after cervical surgery. When the biochemical markers of bone turnover (including CTX and PINP) were determined, all the plasma samples were collected between 6:00 am and 7:00 am (before breakfast), and the samples were immediately sent to the laboratory of the hospital for examination. CTX and PINP were measured using Roche e2010 analyzer (Sandhofer, Mannheim, Germany).
Cervical X-ray film and CT are mainly used for accurate observation and evaluation of bone graft fusion, subsidence of cervical intervertebral fusion cage, adjacent vertebral fracture, titanium plate and screw loosening, and so on. Evaluate and grade according to the standard evaluation of bone graft fusion rate of each patient, is accurately recorded. The abovementioned work is independently evaluated by two highly specialized radiologists with distinct expertise in the evaluation of spinal pathologies.
According to the assessment criteria made by Siepe et al., 2 the bone fusion in the graft area can be divided into four levels: grade 1, complete fusion (clearly visible continuous trabecular bone growth connecting the vertebral bodies with evidence of bony remodeling of callus, continuous bridging bone surrounding or within the cage, solid incorporation of implant at the cage/endplate interfaces, lack of lucency at cage margins, lack of visible fracture of cage or vertebrae, lack of cystic changes within adjacent endplates, lack of linear defects/fracture through the intervertebral new bone formation within or surrounding the cage, and lack of subsidence or dislocation of cage); grade 2, predominant/prevailing signs of solid interbody fusion (bridging callus including trabeculations with extent of fusion >75%, partial signs of trabecular bone connecting the intervertebral space, and exclusion of any clear signs of nonunion); grade 3, likely not fused/incomplete signs of solid interbody fusion (partial bony bridging and/or bridging callus in the intervertebral space, and solid graft incorporation only at one side of the cage/endplate interfaces); grade 4, nonunion (formation of complete/continuous clefts, sclerotic margins at clefts, vacuum phenomena, insufficient intervertebral bone bridging, lucency at cage margins, visible fracture of cage or vertebrae, cystic changes within adjacent endplates, linear defects/fracture through the intervertebral new bone formation within or surrounding the cage, or absence of continuous bridging bone surrounding or within the cage). The standard of the stability of cervical spine fusion is 1 or 2 grade osteogenesis with local angulation activity less than 2° at the same time. 3
Statistical analysis
SPSS 20.0 statistical software was used for data analysis, and the measurement data were expressed as mean plus or minus standard deviation (x ± s), with two digits after the decimal point. Quantitative data were tested for normality before statistical analysis, and all parameters were in normal distribution. Therefore, student’s t test and χ 2 test were used in comparison of the difference between study and control groups, and p < 0.05 was defined as statistically significant difference.
Results
Clinical effect
A total of 52 patients were selected, including 43 cases with complete follow-up, 21 in the study group and 22 in the control group. Detailed case data of the two groups are given in Table 1. There was no significant difference in sex ratio, age, NDI score, and body mass index (BMI) between the two groups before surgery (p > 0.05). During the postoperative follow-up, the NDI scores of the two groups at each time point significantly decreased compared with the preoperative ones which have statistically significant differences (p < 0.05). Two groups both showed a significant decrease in NDI scores at the 3rd month after surgery, and they came to the plateau at the 6th month after surgery, while their scores had some rise at the 12th month. However, the difference in NDI scores between the two groups was not statistically significant at any of the follow-up times except for the last one. The NDI score of the study group was lower than that of the control group at the 12th month after surgery (p = 0.026 < 0.05), as shown in Figure 2.
General information of the cases.
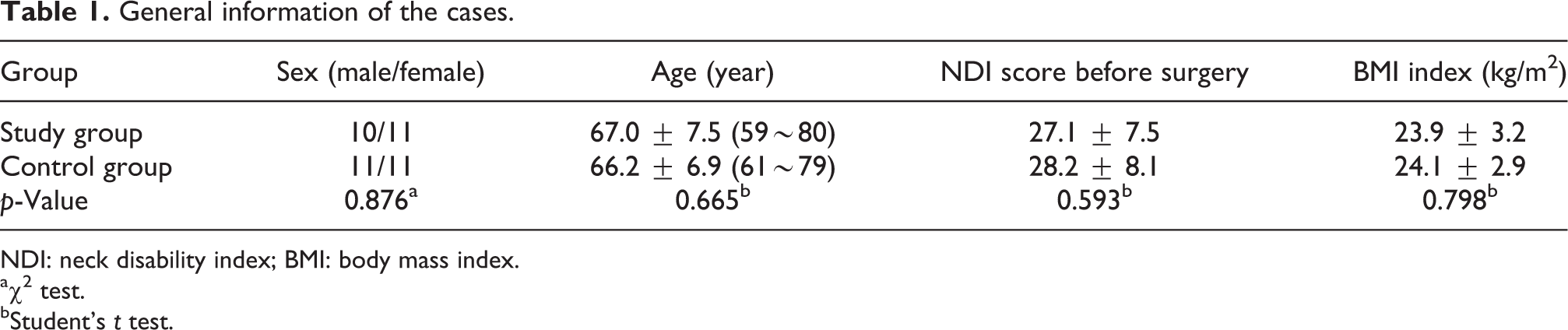
NDI: neck disability index; BMI: body mass index.
a χ 2 test.
bStudent’s t test.

NDI score trend of two groups varied with time. Study group: NDI scores before surgery was 27.1 ± 2.4, 10.8 ± 2.1 at the 3rd month after surgery, 11.2 ± 1.9 at the 6th month after surgery, and 11.5 ± 1.9 at the 12th month; control group: NDI scores before surgery was 28.2 ± 2.6, 10.9 ± 2.3 at the 3rd month, 12.3 ± 2.2 at the 6th month, and 13.9 ± 2.0 at the 12th month. In both groups, the decrease was most obvious after 3 months, and then increased slightly in varying degrees, especially in the control group. NDI: neck disability index.
Changes of biochemical markers in bone turnover
There was no significant difference in serum PINP and CTX levels between the two groups before surgery (p = 0.764, 0.556). PINP in the study group showed a downward trend at each time point after surgery, which decreased by 40.5% at the 12th month compared with the preoperative level, while there was no significant change in the control group. CTX in the study group showed a downward trend at each time point after surgery, which was 70.4% lower than the preoperative level at the 12th month, while there was no significant change in the control group. There were significant differences between the two groups at each time point after surgery (p < 0.001), as given in Table 2.
Changes in biochemical markers of bone turnover for two groups at different phases.a

PINP: amino terminal propeptide of type-I procollagen.
aStudent’s t test was used.
Change of BMD
Bilateral femoral necks and lumbar were selected for BMD measurement. There was no statistically significant difference between the two groups before surgery (p > 0.05). At the 12th month follow-up after surgery, the BMD in the three parts of the study group was improved, among which the BMD of the lumbar spine was significantly improved compared with that of the preoperative group, and the difference was statistically significant (p = 0.013 < 0.05), while there was no significant difference in the control group, see Table 3 for details.
BMD changes at different phases in two groups.a

BMD: bone mineral density.
aPaired t test was used.
Imaging evaluation
At the 3rd month follow-up after surgery, the grade 1/2 osteogenesis rate of the study group was 76.2% (16/21), while that of the control group was only 45.5% (10/22), showing statistically significant differences (χ 2 = 4.246, p = 0.039 < 0.05). At the 6th month after surgery, the grade 1/2 osteogenesis rate of the study group was 90.5% (19/21), still statistically higher than 68.2% (15/22) of the control group (χ 2 = 4.337, p = 0.037 > 0.05). However, all patients in both groups achieved
grade 1/2 osteogenesis at the 12th month follow-up after surgery, and all achieved the standard of cervical stable fusion.
During the follow-up, different levels of subsidence of cervical intervertebral fusion cage were observed in both groups, including two cases in the study group and four cases in the control group; one case of anterior titanium plate and screw loosening occurred in the control group.
Discussion
Effect of bisphosphonates on spinal fusion
Bisphosphonates can be bound to bone surface on which the bone reconstructive is active, to inhibit the function of osteoclasts, and thereby inhibit bone resorption. Bisphosphonates are the most widely used anti-osteoporosis drugs in clinical practice, mainly including alendronate sodium, ZA, risedronate sodium, ibandronate sodium, itidronate disodium, and so on.
The mechanism of bisphosphonates action is to inhibit the differentiation of osteoclasts precursors into osteoclasts, increase the apoptosis of osteoclasts, 4 and reduce the level of bone turnover. Therefore, it has an inhibitory effect on both bone resorption and bone formation. Meanwhile, bisphosphonates also have potential anti-angiogenesis effects, 5 which may lead to the reduction of blood supply at the fusion site. In view of the abovementioned factors, the effect of bisphosphonates on spinal fusion is still controversial. For example, Yalçin et al. 6 established a rabbit lumbar posterior fusion model, applied hyperbaric oxygen and ZA for grouping intervention, and found that local application of ZA combined with hyperbaric oxygen can increase the fusion rate of lumbar posterior fusion surgery. Bransford et al. 7 observed the effect of ZA on lumbar fusion in rabbits and found that it increased the volume, density, and fusion rate of fusion bone fragments. Kodera et al. 8 established the spinal fusion model of rats and applied rhBMP-2 locally and subcutaneous one-time injection of ZA. The results showed that the fusion rate of rats in the combined application group was significantly higher than that of the control group. The results of microscopic CT analysis showed that the callus tissue and bone volume were significantly higher than those of the control group. Another randomized controlled study involving 69 patients found that postoperative intravenous ZA could shorten the time of spinal fusion after lumbar surgery in patients with osteoporosis, increase the fusion rate, and prevent adjacent vertebral compression fractures, thereby improving clinical effect. 9 However, not all the results were so optimistic. For example, Xue et al. 10 studied the effect of oral alendronate on spinal fusion after lumbar posterolateral fusion in a pig model and found that alendronate had no effect on lumbar fusion rate after lumbar fusion. Therefore, to determine the effects of bisphosphonates on spinal fusion, further large prospective randomized controlled studies are needed.
Effect of ZA on cervical fusion
In review of previous studies, we found that studies on the effects of bisphosphonates on spinal fusion were mainly focused on the lumbar spine, 9,11,12 while few on the cervical or thoracic spine. There have been many animal studies, 13 but few animal models of osteoporosis are available, so it is not possible to simulate the spine fusion when osteoporosis occurs.
In this study, 43 cases of cervical spondylosis and osteoporosis patients involved in the study at the time of 12th-month follow-up after surgery all get good fusion, and at the 3rd and sixth month after surgery, the group’s grade 1/2 osteogenesis rate is significantly higher than that of the control group, all these show that the intravenous application of ZA after cervical fusion can promote fusion and accelerate local osteogenesis. This finding is consistent with previous observations in lumbar fusion. For instant, Tu et al. 14 explored the efficacy of intravenous infusion of ZA on clinical outcome and bone fusion after lumbar interbody fusion surgery. At 2-year follow-up, a solid fusion was achieved in 75% of the ZA group and only 56% of the control group. A similar study conducted by Ding et al. 11 showed that the lumbar spinal fusion rate of ZA group was 92% at 12 months, while it was 92.86% in control group. Compared with previous studies on lumbar fusion, the subjects in this study had a higher fusion rate, which may be related to large contact surface between grafted bone and upper/lower vertebral body in ACDF surgery.
On the other hand, intravenous ZA intervention can alleviate the symptoms of bone pain in patients with osteoporosis 15 and reduce the incidence of cervical intervertebral fusion cage subsidence and titanium plate and screw loosening, thereby reducing the NDI score of patients and improving the clinical effect of patients. Results show that at the 3rd month after surgery, NDI score decreased significantly in both groups which was related to the surgery removing pathogenic factors; at the 6th month, it came to the plateau; and at the 12th month, NDI score had some rise which had statistically significant difference when compared with study group (p < 0.05). It was suggested that ZA could optimize the NDI score of patients after fusion surgery by the abovementioned method and improve their quality of life.
For intravenous application of ZA, how to promote local spinal fusion concrete mechanism is not very clear. Five milligrams of ZA should be distributed to the whole body bone after intravenous drip, cervical vertebra can be assigned to very few amount of ZA, so it needs further research to confirm how such few amount of ZA promote spinal fusion. Xue et al. 16 studied oral alendronate effect for screw–bone interface fixation after lumbar posterolateral fusion by pig models, and the results found that alendronate treatment of 10 mg/daily orally increased bone purchase of stainless steel screw surfaces. By analogy, ZA enhances fixation at the cervical screw–bone interface, thus increasing local stability may be one of the mechanisms that promotes spinal fusion. These need to be further verified in animal and clinical trials.
Analysis of the effect of ZA application on bone conversion index and bone density
Respectively, this study measured the bone resorption marker CTX and bone formation marker PINP, compared the change of bone turnover markers at the preoperative and postoperative time points, the results show that ZA can last for a long time (up to 12 months), significantly reduced bone turnover markers CTX and PINP levels, especially bone resorption markers CTX which was reduced by 70.4% after 12 months treatment compared with that before surgery, its decrease was 40.5% significantly greater than bone formation marker PINP. In recent researches on lumbar spinal fusion, ZA also showed similar effects in inhibiting bone metabolism. For example, Li et al. 17 found that after intravenous infusion of 5-mg ZA, the serum CTX and PINP value decreased from the early phase after surgery and thereafter had a gradual decrease until 12 months postoperatively. While the placebo group even increased slightly. Similarly, Chen et al. 9 proved that both beta-CTX and PINP were suppressed in ZA group. Besides, CTX, the bone resorption marker, decreased more significantly than PINP, which is a bone formation marker. In our opinion, this is in relation with ZA, which mainly antagonizes osteoclasts, induces their apoptosis, and reduces bone resorption, 18,19 but has relatively weak inhibiting effect on bone formation.
BMD, which can reflect the filling of bone reconstruction space and the degree of bone mineralization, is one of the important indicators to predict fracture risk and is widely used in the evaluation on the effect of anti-osteoporosis drugs. In previous studies, ZA, when applied once a year intravenously, has been found to significantly increase BMD and decrease the incidence of osteoporotic fractures. 20,21 The results of Chen et al. 9 showed that BMD at the femoral neck in the ZA group was elevated gradually after lumbar interbody fusion surgery and significantly higher than the saline group at all postoperative periods (3, 6, and 12 months post-surgery). In this study, BMD changes were observed after 12 months of anti-osteoporosis with ZA, and the BMD in three selected parts (bilateral femoral necks and lumbar) was improved, especially the lumbar spine was improved most significantly, but the improvement of bilateral femoral neck was relatively small, which was mainly related to the short observation time by our speculation.
Limitations
However, there were some limitations in this study. The included sample size was small, and the follow-up time was only 12 months. Since the recommended amount of ZA used for the treatment of osteoporosis was 5 mg, 20,22 we did not try other doses. Therefore, further studies on larger sample size, longer follow-up time, and deeper mechanism of ZA effect on cervical fusion are needed.
Conclusion
The results of this study indicated that the intravenous application of ZA in patients with cervical spondylosis and osteoporosis after anterior cervical decompression and fusion can shorten the time of cervical osteogenesis, promote local bone graft fusion, and improve the postoperative clinical effect to some extent. This study is a randomized, double-blind, placebo-controlled trial, so it can well avoid the interference of some potential confounders, such as BMD, BMI, psychological factors, and so on, and the results are highly reliable. The previous literature was reviewed, and no similar reports of clinical trials were found. Therefore, it was quite innovative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.