
Abstract
Purpose:
To identify risk factors for occurrence of symptomatic adjacent segment disease (ASD) after posterior lumbar instrumentation surgery.
Methods:
This retrospective study evaluated 630 patients who underwent posterior lumbar transpedicular instrumentation for degenerative lumbar disorders between April 2008 and April 2012. On the basis of developing ASD at follow-up, patients were categorized into two groups: the ASD group and the non-ASD (N-ASD) group. These two groups were compared for patient characteristics, surgical variables, and radiographic parameters to investigate the possible predictive factors of ASD.
Results:
Of the 630 individuals participated in the study, 76 (12.1%) patients had ASD. Mean and standard deviation of age were 61.37 ± 4.12 years for the ASD group and 62.37 ± 3.9 for the N-ASD group (p = 0.79). The average follow-up period was 51 ± 2.2 months in the ASD group and 52 ± 2.3 months in the N-ASD group (p = 0.691). There were no significant differences between the two groups in terms of gender, diabetes mellitus (DM), hypertension, smoking, and osteoporosis, with all p > 0.05. The logistic regression analysis demonstrated that higher preoperative body mass index (BMI; odds ratio (OR) 1.233, p = 0.005), preoperative disc degeneration (OR 1.033, p = 0.024), decreased postoperative lumbar lordosis (OR 3.080, p = 0.011), fusion at more than four levels (OR 4.280, p = 0.014), and intraoperative superior facet joint violation (OR 7.480, p = 0.009) were independently associated with ASD.
Conclusions:
Patients with higher preoperative BMI, preoperative disc degeneration, decreased postoperative lumbar lordosis, fusion at more than four levels, and intraoperative superior facet joint violation have a statistically significant increased risk of developing ASD.
Introduction
Spinal instrumentation surgery is a common surgical procedure for treatment of various lumbar spinal disorders including spinal degenerative disease. 1 –4 Posterior spinal fusion with transpedicular posterior spinal instrumentation is the standard procedure in the treatment of degenerative spinal disorders. 3 –7 Despite providing stability, spinal fixation disturbs normal biomechanics of the spine, thereby accelerating the degenerative change of the adjacent unfused segments. 8 –33 The various type of pathological changes of the adjacent segments are spondylolisthesis, canal stenosis, disc herniation, disc height loss, osteophyte formation, and scoliosis. 15 –30 The reported prevalence of radiographic-based adjacent segment disease (ASD) and symptomatic ASD is about 40% and between 5.2% and 18.5%, respectively. 12 –34 The most common reported risk factors for developing ASD are age, gender, body mass index (BMI), smoking, osteoporosis, preexisting degeneration of adjacent disc, violation of adjacent facet during surgery, sagittal imbalance, rigid fixation, and the length of fusion. 4 –37
Despite the presence of multiple mentioned risk factors for developing ASD, there is a controversy regarding the most important risk factors for occurrence of ASD.
The main aim of this study was to identify the main risk factors for developing ASD following posterior lumbar instrumentation for degenerative lumbar disorders.
Materials and methods
This study was conducted retrospectively in the Neurosurgery Department of Kermanshah University of Medical Science, Kermanshah, Iran, from April 2008 to April 2012. This study includes consecutive group of patients. Of the 658 patients who met the inclusion criteria, 28 individuals were removed from the study due to incomplete follow-up period or imaging. Approval for this study was obtained from the Scientific Research Board, University of Kermanshah, before data collection and analysis. Medical records of patients who had undergone posterior transpedicular lumbar instrumentation for treating lumbar spinal degenerative disease between April 2008 and April 2012 were evaluated retrospectively. The surgery was performed between 2008 and 2012 by two surgeons in a single tertiary academic institution. Follow-up duration was at least 4 years. The inclusion criteria were posterior spinal fusion for treating degenerative lumbar disorders including degenerative spondylolisthesis, spinal stenosis, disc herniation, and degenerative scoliosis; follow-up duration was more than 4 years with complete radiological data including anteroposterior and lateral lumbosacral X-ray at preoperation, early postoperation, and the last follow-up visit; magnetic resonance imaging (MRI); and computed tomography at preoperation and the last follow-up visit.
Exclusion criteria were posterior spinal instrumentation for treating non-degenerative spinal disorders such as trauma, tumor and infection, and history of previous lumbar surgery. Patients with uninstrumented fusion and patients who had not achieved successful union were excluded. ASD was defined as the pathological process at the closest disc space to the previously fused levels leading to clinical symptoms including radiculopathy, stenosis, and instability.
The radiographic criteria for ASD were the development of disc height collapse >20%, the presence of olisthesis of >4 mm, segmental motion instability of >10° on flexion and extension lateral radiography, and detection of spinal stenosis or disc herniation at an adjacent level in follow-up MRI.
Radiographs at the first surgery and at the last follow-up were evaluated in both groups to evaluate the lumbar lordotic angle, the S1 sagittal slope angle, L1 to S1 sagittal plumb lines, and adjacent disc height. Preoperative adjacent disc degeneration (ADD) was determined based on MRI of patients according to the classification of Pfirrmann et al. 25 (five grades: I (best)–V (worst)). The lumbar lordosis was measured by Cobb’s method between the T12 inferior end plate and S1 superior end plate.
The L1 sagittal plumb line was drawn from the center of L1. The S1 sagittal plumb line was drawn from the posterior end of S1 vertebrae. The distance between the L1 and S1 plumb lines was measured as the shortest perpendicular length between the two lines. The sacral sagittal slope angle was measured as the angle between the superior end plate of S1 and a horizontal line. The adjacent disc height was measured from the middle of the superior border of the disc to the middle of the inferior border of the adjacent disc on lateral radiograph.
According to the presence of ASD at the final follow-up, patients were categorized into two groups: the ASD group and the non-ASD (N-ASD) group.
We analyzed the risk factors for ASD development, including age, gender, BMI, smoking, hypertension, osteoporosis, preexisting degeneration of adjacent disc, violation of adjacent facet during surgery, type and length of fusion, preoperative and postoperative lumbar lordotic angle, preoperative S1 sagittal slope angle, and preoperative and postoperative L1 to S1 sagittal plumb lines.
Clinical outcome was assessed before surgery and at the latest follow-up using the Oswestry questionnaire.
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, Illinois, USA) version 21.0. Continuous variables were measured as mean ± standard deviation, and categorical variables were expressed as frequency or percentages. An independent t-test was used to analyze the difference of continuous variables. Categorical data were compared using the χ 2 analyses and Fisher’s exact test. Logistic regression analysis was used to analyze the assumed risk factors with backward elimination, in which variables with a significance level of >0.10 were removed. The confidence interval of the odds ratio (OR) was 95%. A value p < 0.05 was considered statistically significant.
Results
Of the 630 consecutive patients participated in the study, 303 (48.09%) were male and 327 (51.91%) were female.
Seventy-six (12.1%) patients had ASD (Table 1). Mean and standard deviation of age at the time of surgery were 61.37 ± 4.12 years for the ASD group and 62.37 ± 3.9 years for the N-ASD group, with no significant difference between the two groups (p = 0.79; Table 4).
Descriptive characteristics of the variables.
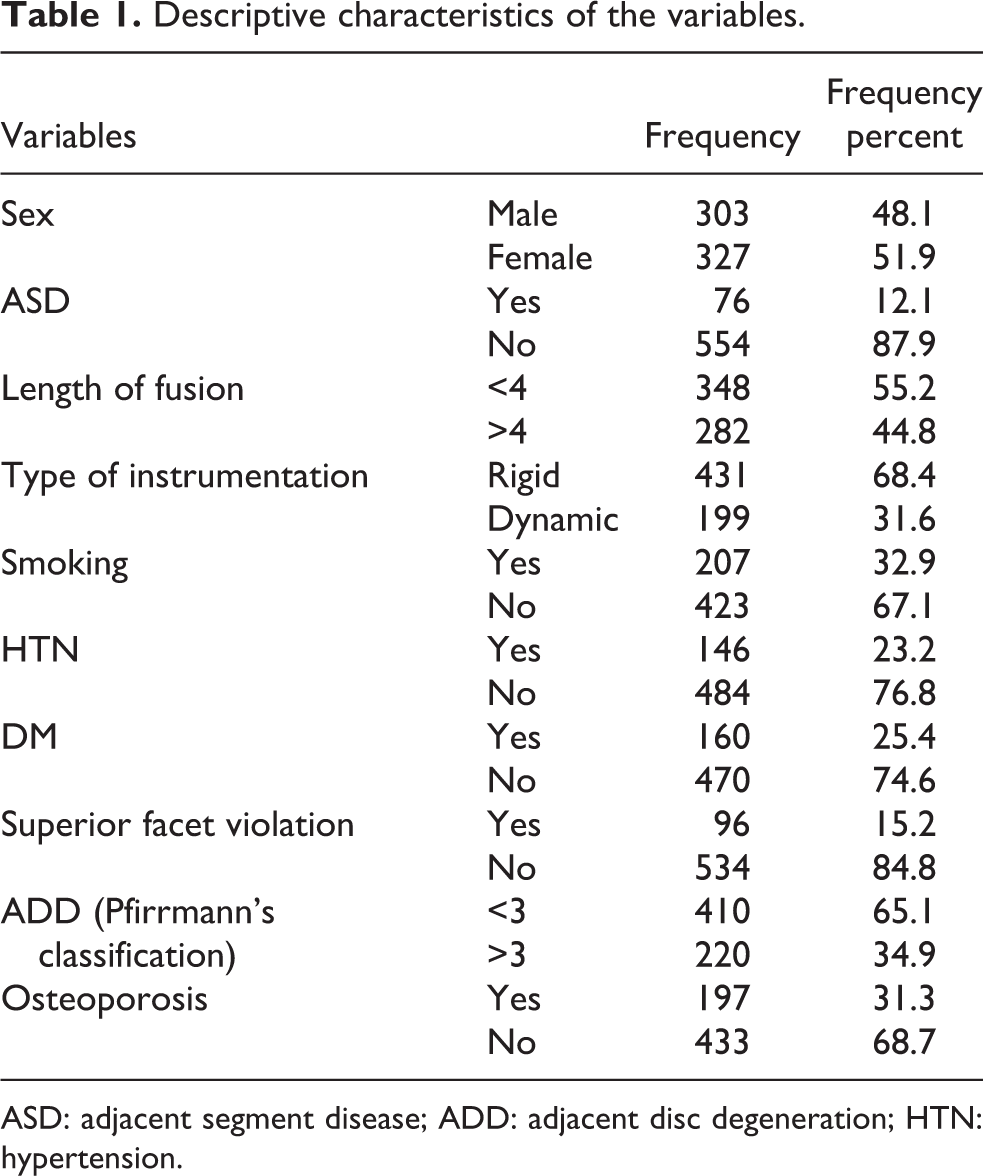
ASD: adjacent segment disease; ADD: adjacent disc degeneration; HTN: hypertension.
The average follow-up period was 51 ± 2.2 months in the ASD group and 52 ± 2.3 months in the N-ASD group, presenting no significant difference (p = 0.691).
Spinal stenosis and spondylolisthesis were the most common imaging finding, and progressive back pain was the most common clinical symptom in the ASD group (Table 2).
Clinical presentation and radiologic finding in ASD group.
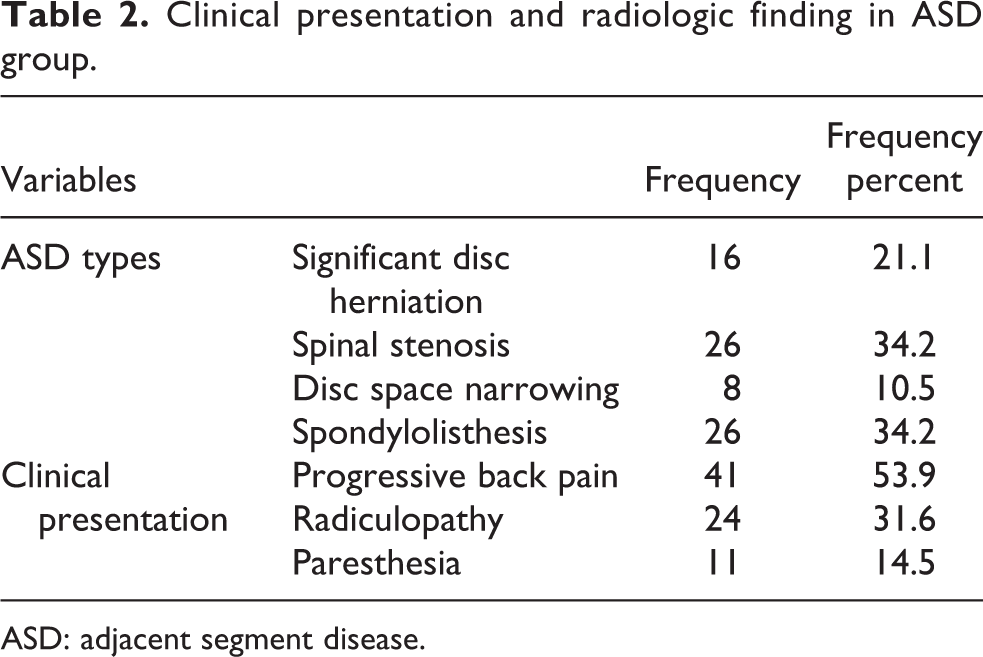
ASD: adjacent segment disease.
There were no significant differences between the two groups in terms of gender, DM, hypertension, smoking, and osteoporosis, with all p > 0.05 (Table 4).
Mean BMI for the ASD group (27.86 kg/m2) was higher than that for the N-ASD group (23.15 kg/m2; p = 0.033).
No significant differences were observed between the two groups in radiographic parameters of preoperative S1 slope angle and postoperative L1 to S1 sagittal plump line, while there were a significant difference between two groups in terms of preoperative and postoperative lumbar lordotic angle, preoperative L1 to S1 sagittal plumb lines, and preoperative adjacent segment disc degeneration (Tables 3 and 4).
Comparison of qualitative variables between ASD group and N-ASD group.
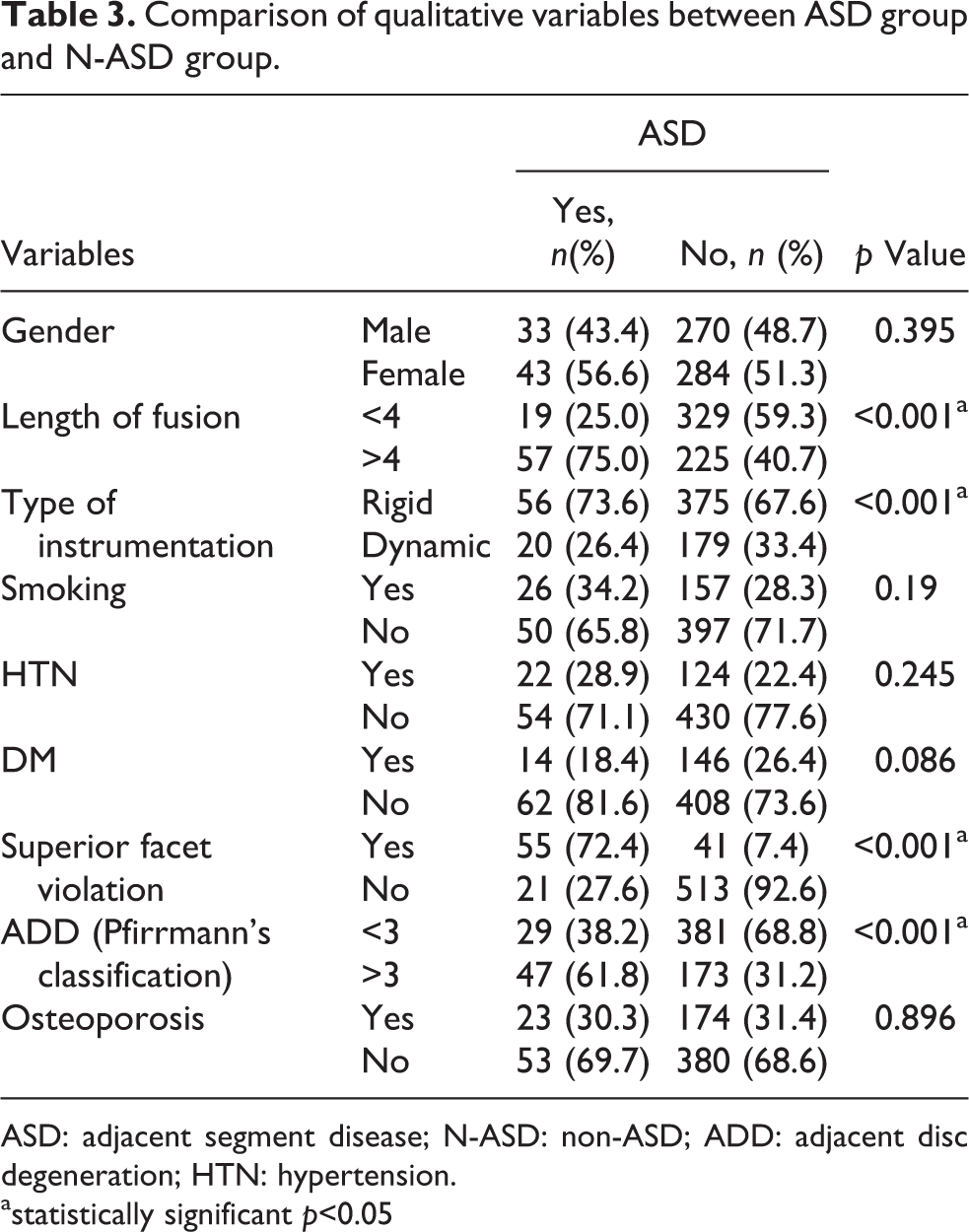
ASD: adjacent segment disease; N-ASD: non-ASD; ADD: adjacent disc degeneration; HTN: hypertension.
astatistically significant p<0.05
Comparison of quantitative variables between ASD group and N-ASD group.

ASD: adjacent segment disease; N-ASD: non-ASD; BMI: body mass index.
astatistically significant p<0.05
Intraoperative superior facet joint violation was more common in ASD group than that in N-ASD group (Table 3).
ASD was more common in patients with more than four levels of fusion and in those with rigid fixation than those with dynamic instrumentation (Table 3).
The logistic regression analysis demonstrated that higher preoperative BMI (OR 1.233, p = 0.005), preoperative disc degeneration (OR 1.033, p = 0.024), decreased postoperative lumbar lordosis (OR 3.080, p = 0.011), fusion at more than four levels (OR 4.280, p = 0.014), and intraoperative superior facet joint violation (OR 7.480, p = 0.009) were independently associated with ASD.
The preoperative Oswestry scores of the ASD and N-ASD groups did not have statistical difference (26.6 for ASD vs. 27.9 for N-ASD; p = 0.216).
Patients with ASD had worse Oswestry scores than the patients without ASD at the latest follow-up (19.6 vs. 11.4, p < 0.001).
Revision surgery for ASD was undertaken in 33 patients (5.23%). All patients had intractable symptoms including neurologic claudication, radicular pain or both; 27 patients underwent autogenous posterolateral arthrodesis and extended transpedicle screw fixation and 6 patients underwent simple decompression.
Discussion
Posterior lumbar laminectomy fusion is a common surgical procedure for treatment of patients with degenerative spinal disorders. 3 –7 Complications of the lumbar fusion surgery include implant failure, pseudarthrosis, high rates of reoperation, sagittal spinal imbalancing, and adjacent segment degeneration. 34,37
ASD is a common long-term complication of spinal fusion surgery. The reported prevalence of radiographic-based ASD and symptomatic ASD is about 40% and between 5.2% and 18.5%, respectively. 12 –33
Significant questions remain unclear about the nature and risk factors of ASD. Most literature on ASD is level III and level IV studies and is strongly affected by patient selection bias and reporting.
Cheh et al. 6 declared that radiographic ASD developed in 42.6% of patients and that symptomatic ASD occurred in 30.3% of patients at a minimum of 5 years of follow-up.
In our study, the incidence of ASD was 12.1% (76 of 630) at a period of minimum 4 years of follow-up.
Despite the considerable amount of studies, the exact causes of ASD are uncertain, but changes in spinal biomechanics including increased facet loading, increased intradiscal pressure, and hypermobility at the segments adjacent to fusion levels are believed to play a key role. 13 –31
It is believed that the presence of increased segmental motion and increased intervertebral mechanical stress adjacent to fusion is the primary cause of ASD. 16 –31
The biomechanic changes in the adjacent segment to fusion were studied by different authors. Weinhoffer et al. 31 found that as flexion motion increases, intradiscal pressures increased within adjacent levels. Umehara et al. 28 found a significant increase in the weight bearing and load burden of the posterior column at the adjacent segments after lumbar fusion.
A significant amount of effort has been made to identify the risk factors for ASD.
Liang et al. 18 reported that higher BMI, preoperative adjacent disc bulging, and preoperative ADD were risk factors for ASD.
Lee et al. 17 determined that preexisting facet degeneration is associated with a high risk of ASD.
Park et al. 23 reported that older age, female sex, osteoporosis, addition of instrumentation, postmenopausal state, and fusion length are the risk factors for ASD.
Patient age at the time of surgery has been identified as one of the most important risk factors for ASD. Most studies have shown an increase of ASD incidence according to advancing age. 13 –21 However, some studies have reported no correlation between ASD incidence and age. 9 –27 In our study, there was no relationship between advancing age and ASD.
The significance of sagittal balance after posterior lumbar fusion has been shown in several clinical studies. 16 –31 Oda et al. 21 demonstrated that a kyphotic lumbar fusion could lead to degenerative changes in adjacent facet joints.
Patients with long fusion and postoperative sagittal imbalance have a statistically significant increased chance of developing ASD. 8 –23,35,36 It is believed that the reason is due to an overloading of the adjacent segments and limited compensatory capacities of the long fixed mobile segments. 16 –28 Nagata et al. 20 reported that the increase in motion at adjacent segments was in proportion to the length of fusion. However, Soh et al. 27 demonstrated that there was little relationship between the ASD and the length of fusion. Penta et al. 24 analyzed 52 patients with at least 10 years of follow-up. The investigators showed that 32% of the 52 patients had adjacent segment degeneration and the degenerative changes were independent of the fusion length. Wiltse et al. 32 reported that there was not a relationship between the length of fusion and development of ASD in his study of patients with a maximum three-level fusion. Ghiselli et al. found that patients who had a single-level fusion were more likely to have clinical ASD than those who had a multilevel fusion. 10 Our finding is in line with Scemama et al. 26 who found, when examining up to four-level fusions, an increased incidence of ASD as more levels were included in a fusion.
Dynamic devices have been used to solve the complication of ASD with controversial results. 7 –20,35,36 It has been suggested that motion preservation surgery without fusion may prevent accelerated ASD.
Dynamic devices allow mobile load transfer, thereby off-loading posterior disc and the facet joints. 7 –20,35,36 But a recent prospective clinical study showed that disc degeneration at the cranial adjacent segment continues (20%) despite dynamic stabilization. 29
Etebar and Cahill 36 performed a retrospective analysis. They reported that the risk of ASD is higher for patients with rigid instrumentation.
The incidence of revision surgery in the presence of ASD has been reported to be about (2–15%) in the literature. According to these findings, radiographical degeneration of the adjacent segment is relatively common after lumbar spinal fusion, but only a small proportion of patients with ASD require revision surgery. 7 –15,35,36
Aiki et al. 2 reported that 7.7% of patients with posterolateral fusion needed a second operation for adjacent segment alteration after a minimum of 2 years. Ghiselli et al. 10 reported that the rates of symptomatic degeneration requiring surgery at adjacent segments were 16.5% at 5 years and 36.1% at 10 years after the index fusion. New alteration at an adjacent segment thus developed at a rate of 3.9% per year. In our study, revision surgery was needed in 5.23% of the 630, showing relatively low incidence. However, the incidence is expected to increase with longer follow-up.
In the present study, preoperative disc degeneration, higher preoperative BMI, decreased postoperative lumbar lordosis, fusion at more than four levels, and intraoperative superior facet joint violation were significantly and independently associated with the occurrence of ASD.
We supposed that: Patients with the risk factors mentioned above should be well informed about the risk of ASD before surgery. Reducing body weight before and after surgery may be of some help to reduce the incidence of ASD. Restoration of sagittal balance and normal lumbar lordosis is the important factors in spine surgery to maintain normal spinal biomechanics and reducing ASD. Prevention of intraoperative facet joint violation by meticulous manipulation in exposure, accurate identification of the facet joints, and meticulous insertion of pedicular screw could provide a chance to reduce the incidence of postoperative ASD.
There are several limitations in this study. First, this was a retrospective study and was not randomized and controlled. Second, the number of patients is relatively small, and the study may be under influenced to detect the importance of some risk factors. However, the results of our study could provide valuable data for helping surgeons and patients who undergone posterior lumbar instrumentation and fusion.
Conclusions
The occurrence of ASD is most likely multifactorial. Our study suggested that patients with higher preoperative BMI, preoperative disc degeneration, decreased postoperative lumbar lordosis, fusion at more than four levels, and intraoperative superior facet joint violation have a statistically significant increased risk of developing ASD after posterior lumbar fusion and pedicular fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.