
Abstract
Aneurysmal bone cysts (ABCs) rarely trigger pathological fractures. Various surgical and nonsurgical treatments have been reported for this condition. Herein, we present the examination findings and treatment for a 15-year-old girl who initially presented with adolescent idiopathic scoliosis and mild back pain, but subsequently experienced severe back pain. Magnetic resonance imaging revealed an ABC at T1, with an associated pathological fracture. We successfully treated the patient using posterior fixation with instrumentation, curettage, and bone grafts combined with calcitonin and methylprednisolone (mPSL). At 3 years post-surgery, there was no ABC recurrence and only mild back pain persisted. To our knowledge, this is the first report of open surgery (curettage and fixation) with local intralesional administration of calcitonin and mPSL for an ABC-induced pathological spinal fracture. We believe that this treatment is an effective option for ABCs associated with a pathological spinal fracture.
Introduction
Aneurysmal bone cysts (ABCs) are benign bone tumors that account for approximately 1% of all primary bone tumors. 1 –3 The majority of ABCs appear before the age of 20, with approximately 10–30% of these tumors originating from the spine. 1,4 ABCs are benign lesions but are locally destructive and aggressive in nature. 5,6 If surgical treatment targeting only the cyst is performed, a high recurrence rate can be expected. 2 In this case report, we describe a good outcome with no recurrence following curettage and bone grafting accompanied by intralesional administration of calcitonin and methylprednisolone (mPSL) for an ABC in the first thoracic vertebra (T1).
Case presentation
A 15-year-old girl with scoliosis was referred to our department from an orthopedic clinic. The patient, and her guardian, provided informed consent for the publication of this report. Our initial examination revealed no remarkable neurological findings or medical history, although the patient complained of mild back pain and had a hump on the right rib. Total spinal radiography revealed a thoracic curve with a convex right side and a Cobb’s angle of 20° at T5–T11 (Figure 1). Based on these findings, we diagnosed the patient with adolescent idiopathic scoliosis, assuming that the scoliosis was the source of her mild back pain. However, 3 months after her first outpatient visit, the patient complained of severe back pain that had forced her to cease her sporting activities. Our examinations revealed no abnormal neurological findings, although magnetic resonance imaging of the total spine revealed an expansive mass at T1, along with a fluid–fluid level in the T1 vertebra, a characteristic sign of an ABC. No spinal cord or nerve root compression was observed (Figure 2). A percutaneous transpedicular biopsy at T1 was subsequently performed under radiographic guidance. Pathological examination of the specimen revealed blood and a fibrous cyst wall with giant cells, confirming the diagnosis of an ABC at T1 (Figure 3). Computed tomography (CT) further revealed an enlarged bone, an osteolytic lesion, a thinning cortex, and a loss of cortical continuity of the anterior and posterior elements of the vertebra (Figure 4). Based on these findings, we diagnosed the patient with a pathological fracture of T1 and allocated a score of 14 for the T1 ABC according to the Spinal Instability in Neoplastic Score: “unstable” is superior to 13. 7 This led us to consider internal fixation. The tumor was classified as an Enneking stage 2 lesion, 8 with the involvement of zones 1–8 (Weinstein–Boriani–Biagini (WBB) class B and superficial intraosseous lesion). 9 Thus, based on the Enneking staging and WBB classification, the ideal scenario would have involved extracapsular excision at T1. However, in this case, the tumor extended to the anterior cortex of the T1 vertebra, with thinning of the cortices of the vertebra. We therefore considered resection of the T1 vertebra through either an anterior or posterior approach. The anterior approach was complicated by the location of large vessels (the brachiocephalic vein and aortic arch) and the necessity for a median sternotomy. Given these safety considerations, we selected a posterior approach and the use of calcitonin and mPSL with transpedicular curettage, bone grafting (using autologous and artificial bone), and posterior fixation from C7 to T2 using pedicle screws (Figure 5). Because we planned to remove the implants after confirming osteosclerosis of T1, we did not place the bone grafts between the intervertebral spaces. There was marked bleeding from the tumor during curettage, but this was subsequently controlled. Autologous bone was obtained from the iliac region, and artificial bone was constructed using hydroxyapatite. Both types of bone were mixed with calcitonin (200 IU) and mPSL (125 mg) and were then grafted into the curettage and fracture sites. The dosage of calcitonin and mPSL was determined in accordance with previous studies. 10,11

Standing spinal radiograph showing a right convex thoracic curve with a Cobb’s angle of 20° at T5–T11.
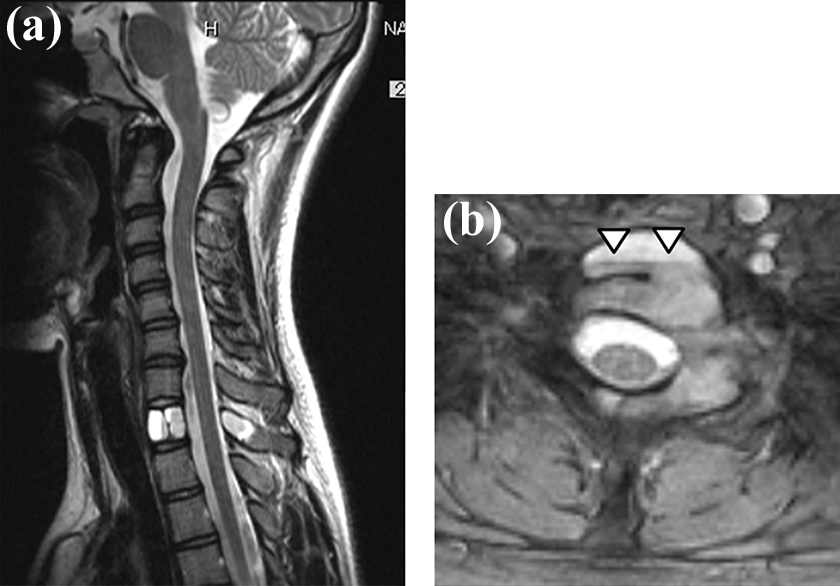
Magnetic resonance image showing (a) an expansive mass at T1 and (b) a fluid–fluid level (arrowhead) of the T1 vertebra. No spinal cord or nerve root compression was detected.

Pathological examination of the biopsy specimen showing blood and fibrous cyst walls (arrowhead) with giant cells (arrow). Hematoxylin–eosin staining. Scale bar = 250 μm.

Computed tomography image showing an enlarged bone, an osteolytic lesion, a thinning cortex, and loss of cortical continuity of both the anterior and posterior elements of T1 (a to d).
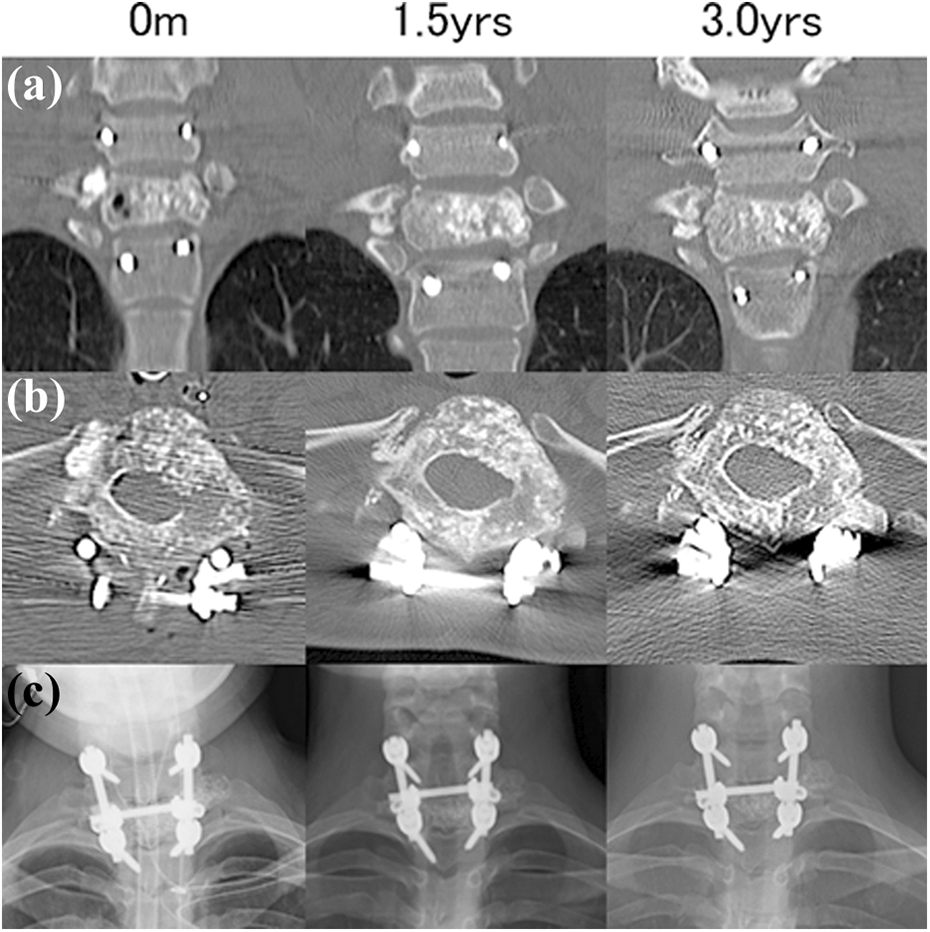
Computed tomography (a and b) and radiographic images (c) obtained immediately post-surgery (0 m), 1.5 years post-surgery (1.5 years), and 3 years post-surgery (3.0 years). Several postoperative cysts within the T1 vertebra are visible in (a) and (b) at 0 m. These cysts were filled with bony tissue in (a) and (b) at 1.5 and 3.0 years, with no evidence of recurrence of the aneurysmal bone cyst.
At the final follow-up, 3 years post-surgery, CT imaging indicated no recurrence, calcification of the bone grafts, remodeling of the cortical bones, and an absence of regions showing bone resorption (Figure 5). The patient reported only a mild level of back pain, and the Cobb angle had remained at 20° without progression of the scoliotic curvature.
Discussion
ABCs are benign but locally destructive and aggressive lesions. 5,6 Total excision, including the entire cyst, would represent an obvious treatment choice from the viewpoint of preventing recurrence, 12 but was considered not in line with oncological strategy. 8,9 According to the Enneking 8 and WBB classifications, 9 total ablation is required for ABCs, including the film. In our patient, however, the tumor infiltrated almost the entire vertebral body and the cortical bone was flattened. It was thought that an excision, including the film, would correspond to the total removal of the tumor vertebrae. However, the tumor was localized to the T1 vertebrae, and we selected a posterior approach after considering operational safety. In addition, the T1 vertebral body caused a pathological fracture; consequently, tumor curettage, bone grafting, and posterior spinal fixation with fusion were performed. We also planned to use a chemical adjuvant prepared from a combination of calcitonin and mPSL for the ABC.
A wide range of methods have been used to treat ABCs, including surgical treatment, 1,4,12 –16 selective arterial embolization (SAE), 1,4,17 radiation, 1,15 Ethibloc injection, 18,19 denosumab, 6 doxycycline, 20,21 and injection of calcitonin and mPSL (Table 1). The recurrence of ABC is a concern during surgical treatment, and the reported recurrence rates are as high as 20%. 2 Our review of the literature showed that the recurrence rate of curettage with or without embolization was approximately 10% (15 cases in 145 patients; Table 1). On the contrary, no recurrence has been reported following en bloc excision. 4,16 Except for surgery, SAE is considered the first choice of treatment because of its osteoblastic effect on spinal ABCs and the reduced intraoperative blood loss associated with this technique. 4,7 However, we did not select SAE in the present case because of the patient’s unwillingness to undergo the procedure. The recurrence rate after radiotherapy alone has been reported to be 25% and was expected for this type of treatment; however, the general consensus is that the most significant problem is the risk of complications and side effects, such as growth plate damage, radiation myelopathy, gonadal damage, and sarcoma induction. 2 Moreover, a complication rate as high as 30% has been associated with injection of the fibrosing agent Ethibloc, including complications such as pulmonary embolism, aseptic fistula, transient inflammatory reaction, and brain death. 18,19 Lange et al. recently reported that denosumab injection was an effective treatment for spinal ABCs, although the potential side effects and the appropriate duration of this form of therapy remain unclear. 6
Summary of treatment, recurrence rate, site of occurrence, and complications in 145 patients.

PE: pulmonary embolism.
Recent reports have indicated that percutaneous intralesional injection of calcitonin and mPSL can provide successful treatment and lead to regression of an ABC and subsequent ossification of the cyst. 2,3,10,11 Szendroi et al. reported that multiple intralesional injections of calcitonin also caused ossification of ABCs. 22 Furthermore, it has been reported that frequency fewer number of combined calcitonin and mPSL injections were needed to achieve ossification of cysts than injections of calcitonin alone. 2,11 These positive treatment outcomes are likely to reflect the suppressive effect of calcitonin on osteoclast formation and subsequent promotion of bone formation. 2,3,10,11,23 Moreover, mPSL inhibits both angiogenesis and fibrogenesis effects that are likely to be synergistic to those of calcitonin. 2,3 To date, no negative effects, such as tumor growth and recurrence, side effects, and complications, have been associated with the combined injection of calcitonin and mPSL. Furthermore, the chemical adjuvant may have an effect on ABC treatment. Thus, we used calcitonin and mPSL to prevent recurrence after curettage of the patient’s ABC with the expectation of a chemical adjuvant effect. Following intralesional administration of these drugs, the patient remained recurrence free at the last follow-up visit 3 years post-surgery. In the previously mentioned reports, multiple intralesional injections of calcitonin and mPSL were required to achieve the desired effect. However, we were able to achieve the desired therapeutic effect with one intralesional administration in combination with surgical curettage. This suggests that reduction of tumor volume might be important for single intralesional injections to exert a sufficient effect.
There are some limitations to this report. The detailed mechanisms underlying the effects of calcitonin and mPSL, both individually and in combination, are unknown. Although the short-term effects of combined calcitonin and mPSL treatment have been reported, there is no long-term follow-up data. The absolute safety and the ability of this treatment to suppress tumor recurrence in the long term remain unknown. Future prospective studies are now required to determine the true chemical adjuvant effect associated with combined calcitonin and mPSL treatment.
We described for the first time a case of spinal ABC treated by open surgery (curettage and fixation), bone grafting, and local intralesional administration of calcitonin and mPSL. No recurrence has been observed at 3 years after treatment. Based on our experience, we believe that this method can effectively treat ABCs associated with pathological spinal fractures.
Footnotes
Authors’ contribution
Akinori Okuda and Hideki Shigematsu contributed to conception and design; Yasuhiko Morimoto and Keisuke Masuda helped in data acquisition; Chiho Ohbayashi performed analysis of data; Eiichiro Iwata and Masato Tanaka drafted the manuscript; Akinori Okuda and Hideki Shigematsu helped in critical revision; Eiichiro Iwata, Masato Tanaka, Yasuhiko Morimoto, and Keisuke Masuda helped in administrative support; Yasuhito Tanaka supervised.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.