
Abstract
Study Design:
Retrospective study.
Objective:
The aim of this study was to evaluate the clinical presentation, treatments, outcome, complications, and recurrence rate in the surgical and nonsurgical management of spinal aneurysmal bone cyst (ABC) in a series of 18 pediatric patients.
Methods:
Between 1988 and 2014, we evaluated 18 pediatric patients diagnosed with ABC confirmed by pathology studies. We analyzed clinical and radiological features, non-surgical and surgical treatment, outcome, and complications.
Results:
The series included 12 male and 6 female patients with a mean age of 10 years and 4 months, with a mean follow-up of 5 years. Location of the ABC was lumbar in 8, cervical in 7, thoracic in 2, and sacral in 1 case. Axial pain was the most common symptom followed by radicular involvement. Surgery was performed in the presence of spine instability or neurological involvement (tumor resection) and in the remaining, nonsurgical treatment (percutaneous intralesional injection of methylprednisolone and calcitonin). Recurrence was observed in 4 patients requiring reintervention. There were no procedure-related complications.
Conclusion:
In patients without neurological involvement or spinal instability, nonsurgical treatment is the treatment of choice. Total or subtotal removal combined with posterior instrumented spinal fusion is recommended in cases with a neurological deficit. Both procedures have shown good long-term results.
Keywords
Introduction
The aneurysmal bone cyst (ABC) is a benign tumor of unknown pathogenesis, with potentially aggressive behavior, and a highly vascularized osteolytic nature. The entity was first described by Jaffe and Liechtenstein in 1942. 1,2 It is a rare tumor accounting for 1.4% of the bone tumors. In the spine, ABCs represent 15% of the primary bone tumors. 3 In around 70% of the cases, the ABCs are primary lesions. Age at presentation ranges between 5 and 20 years and there is a female predominance. 4 -7 ABCs are most commonly located in the posterior elements at the thoracic and lumbar levels. 2,5 -7 The tumor is characterized by rapid and aggressive progression with axial pain as the most common symptom. Neurological involvement, albeit infrequent, may manifest due to spinal instability secondary to destruction of the bone or direct myeloradicular compression.
A characteristic finding on magnetic resonance imaging (MRI) is the presence of fluid-filled multilocular cysts and fluid-fluid levels, and an expansive lesion with a thin bone shell, known as the egg-shell image. 1,4,6,8 Several treatment strategies have been described for ABC ranging from nonsurgical treatment, such as selective arterial embolization, intralesional injections, radiation therapy, to surgical interventions, such as partial intralesional resection, filling with bone graft, and spinal fusion, and complete “en bloc” resection with vertebral reconstruction. Local recurrence of the ABC has often been reported in children with rates between 10% and 60%. 4,8 -11
The aim of this study was to assess the clinical presentation, available treatment, and outcome of 18 pediatric patients with ABC of the spine with a minimum of 2 years of follow-up in our public pediatric tertiary care hospital.
Material and Methods
We conducted a retrospective study of 18 pediatric patients with a diagnosis of ABC in the spine, confirmed by pathology biopsy study followed up for a mean of 5 years and 3 months seen at a single center between 1988 and 2014. The study was approved by the hospital institutional review board (IRB), and because of the retrospective observational nature of the study IRB waived the informed consent.
The following variables were assessed: demographic data of the patients, location of the lesion, number of vertebrae involved, neurological and clinical status, Enneking classification, involvement of the functional structures, type of treatment used, and complications. The clinical charts, radiographs, MRIs, computed tomography (CT) scans, and selective angiography studies, as well pathology studies (percutaneous fine-needle biopsy under CT guidance) were assessed.
As described in the literature, percutaneous intralesional injection of methylprednisolone and calcitonin was the treatment of choice for patients without neurological involvement or spinal instability, while total or partial tumor removal combined with posterior instrumented spinal fusion was performed in children with a neurological deficit.
One of the nonsurgical procedure consisted in fine-needle biopsy and percutaneous intralesional drug injection were performed in the CT scan room with the patient under general anesthesia. The mandatory preprocedure biopsy was performed in the site of the spine that was most severely affected. Once histology confirmation was done, after placement of the needle, a contrast agent was injected into the cyst to define the contents, followed by an injection of 150 mg methylprednisolone associated with 200 IU calcitonin. Because of the multilocular nature of the cyst generally several injections were necessary to fill the largest number of cysts as possible. Six patients required an additional open biopsy as the sample obtained with the fine-needle biopsy under CT guidance was too small for evaluation. The follow-up protocol after injection of the drugs consisted of a CT scan at 60 days followed by a second injection.
On the other hand, patients who underwent surgical procedures a conventional posterior approach was used. Lesional or, if not possible, intralesional tumor resection was performed followed by posterior instrumented fusion with pedicle screws. If necessary, because of the postresection bone defect, the anterior and mid spine was supplemented with structural support with bone from the bone bank, a titanium component, or another substitute. Follow-up consisted of clinical and imaging studies every 3 months in the first year postoperatively, yearly in the subsequent 5 years, and sporadic controls thereafter.
Results
We evaluated 18 patients, 12 boys and 6 girls, with a mean age of 10 years 4 months (4 years 4 months to 15 years 3months) were included in the study. Mean follow-up was 5 years 3 months (2 years 3 months to 11 years). In 8 patients (44%), the ABC was located in the lumbar, in 7 (40%) in the cervical, in 2 (11%) in the thoracic, and in 1 (5%) in the sacral region. Axial pain was the most common symptom, observed in 100% of the cases. Seven patients (33%) reported radiculopathy (brachyalgia, paresthesia, sciatalgia, and cruralgia) and/or myelopathy (urinary retention and paraparesis).
The Enneking staging system was used to stratify the type of lesion. Two patients had a stage 2 (active) and 16 patients had a stage 3 (aggressive) lesion. The mean number of vertebrae involved was 1.7 (1-3). In all patients, the diagnosis of ABC was confirmed by mandatory biopsy and histology studies before any treatment has taken place. In 6 patients, an open biopsy was required as fine-needle biopsy did not provide enough tumor material to perform the studies.
In 15 patients (78%) selective angiography and preoperative embolization was performed, which was successful in 8 (57%). Of the total of the series of 18 patients, 15 underwent surgery because of either neurological compromise or vertebral instability. In 10 of these patients total “en bloc” tumor resection and in the remaining 5 intralesional resection was done. Surgical approach was a conventional posterior in 8, a double approach in 6, and an anterior approach in only 1 patient. Two patients received postoperative radiotherapy because of tumor recurrence. The 3 remaining patients who did not undergo surgical tumor resection received serial intralesional injections (150 mg methylprednisolone and 200 IU calcitonin) under CT guidance. No intraprocedure complications were recorded. After the injection, external immobilization (thermoplastic cervical collar) was used in all patients.
Four patients, 3 who underwent surgery and 1 who did not, presented with tumor recurrence. In 2 of them, an increase in tumor size was observed associated with reappearance of signs and symptoms. In both cases, decompression, tumor excision, and revision surgery instrumented spinal fusion was performed. In the other 2 patients, radiotherapy was conducted with acceptable results (Table 1).
Demographics.
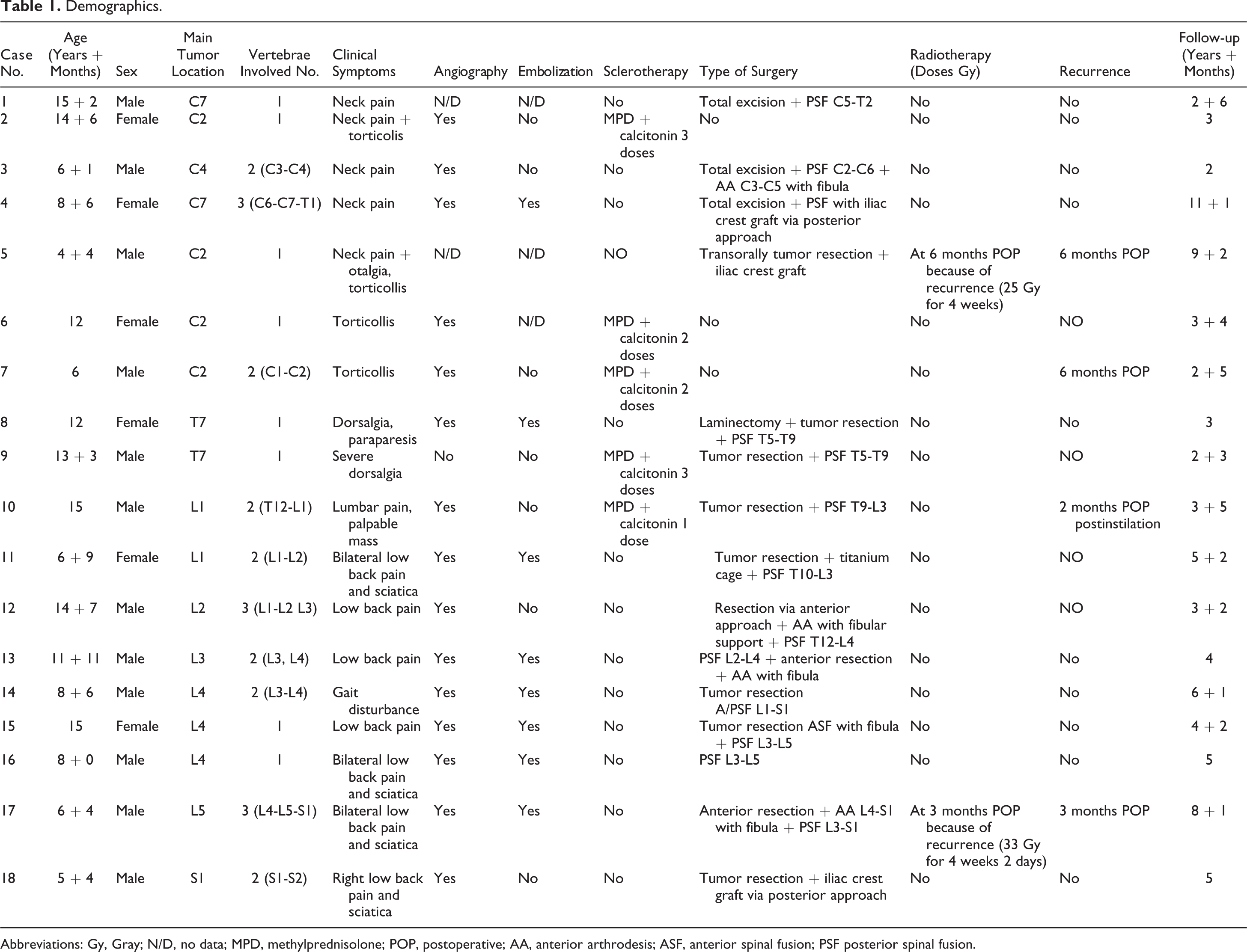
Abbreviations: Gy, Gray; N/D, no data; MPD, methylprednisolone; POP, postoperative; AA, anterior arthrodesis; ASF, anterior spinal fusion; PSF posterior spinal fusion.
At the time of diagnosis, 15 patients had ASIA (American Spinal Injury Association) stage E on neurological examination. Three patients had stage D, which returned to ASIA E in the long-term posttreatment follow-up
Case
Figure 1 presents the radiographs, MRIs, and CT scans of a 15-year-old male patient
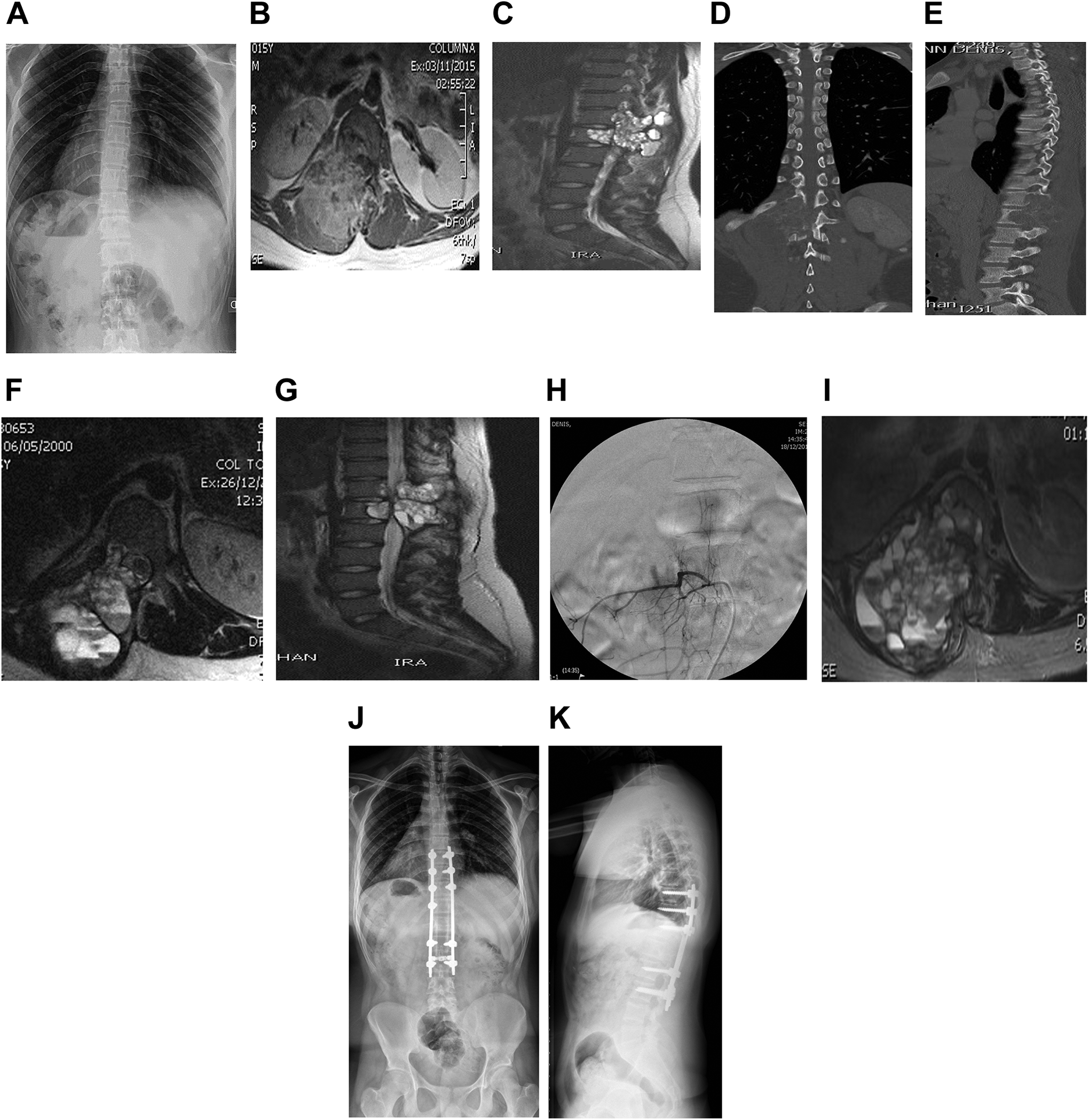
Case: Male 15 years. Lumbar pain 3 months. No trauma. Partially solved with nonsteroidal anti-inflammatory drugs. Labs okay. Neurologically intact. (A) Radiographs without findings. (B, C) Magnetic resonance imaging (MRI): axial and sagittal planes T1/T2. Lesion T12-L1. (D, E) Computed tomography (CT) scan: coronal and sagittal planes. Blastic lesion T12-L1. One week later. Percutaneous T12/L1 CT-guided biopsy and methylprednisolone (150 mg) and calcitonin (200 IU) injection. Pathology: compatible with aneurysmal bone cyst (ABC). (F, G). Post 60 days injection MRI axial and sagittal plane T2. Lesion T12-L1. (H) Arteriography. Right femoral artery catheterism, segmentary afferents T11-T12, L1-L2, no positive results. (I) MRI axial plane T2/STIR. Severe spinal cord compression. No signs of tumor ossification. Severe axial and radicular pain. (J, K) Radiographs anterior-posterior and lateral. Decompression and posterior spinal fusion T9 L3; 36 months postoperative.
Discussion
ABC is a benign bone tumor, but potentially aggressive because of its fast growth and potential bone destruction. ABCs may cause fractures and vertebral instability and a mild to high recurrence rate has been reported. 12,13 It may present as a primary bone lesion or may coexist with another type of tumor. 3,13 Certain factors should be considered in the management of ABCs in the spine in children, 8 including future growth, fusion levels, radiotherapy, and the potential development of radiation-induced sarcoma, 9 deformity, 14 or postlaminectomy kyphosis. 15
In our series, similar to the findings in the literature, 4,12,16 the most common location of the tumor was in the lumbar region, followed by the cervical region. Unlike other studies, in our cohort there was a male predominance. 4,12,13 Six patients (33%) showed neurological involvement at the time of diagnosis, a finding similar to other series that reported a neurological deficit in up to 50% of the cases. 9,12,16 In our series, 100% of the patients recovered completely after tumor removal, decompression, and spinal fusion. Preoperative angiography combined with embolization to avoid massive intraoperative bleeding has been broadly recommended, 2,4,17 -20 and is currently one of the main tools in the nonsurgical treatment of ABC. We agree this treatment modality is the management of choice in cases with tumors that are difficult to access without neurological involvement or imminent risk of fractures. Fifteen patients were submitted to angiography as a first line of treatment, and embolization was successful in only 8 cases.
According to published literature, surgical “en bloc” resection is the treatment of choice in spinal ABCs associated with neurological deficit or spinal instability. 8,9,12,15,17,21,22 In our series, 10 of 14 patients who underwent surgery, were treated using this technique with good results. In the four remaining patient’s resection and tumor curettage was performed.
A higher frequency of local recurrence of the ABC has been reported in children, 9,11 with rates of 10% to 60%. 8,10 En bloc surgical resection may be important to avoid recurrence. 8 In our series, tumor recurrence was observed in 4 patients (22%); 2 of them had undergone tumor surgical resection and 2 had received percutaneous intralesional injection of methylprednisolone and calcitonin.
Intralesional injection of calcitonin—a suppressor of osteoclast activity and promotor of osteogenesis—was first described by Szendroi et al. 23 Recently, good results have been reported with percutaneous injection of calcitonin combined with methylprednisolone acetate—with angiostatic and fibroblastic inhibitory effects. 24 -27 Some authors state that intralesional injection of calcitonin and methylprednisolone is efficacious and a less aggressive and invasive treatment for ABC. 24 -27 In our series, intralesional injection with calcitonin and methylprednisolone was performed in 5 patients, in C2 in 3, L1 in 1, and T7 in 1 case. Two of these patients required subsequent surgery because of worsening of the lesion with pain associated with a pathological fracture in one and neurological involvement in the other patient. Two patients were submitted to radiotherapy.
In our hospital, before any nonsurgical and surgical procedure, we conducted a mandatory percutaneous biopsy, followed by angiography and embolization if possible, intralesion injection of calcitonin and methylprednisolone when no fracture or instability was present. On the other hand, surgery was conducted if instability of fracture was noticed. Currently, denosumab, a human monoclonal antibody that inhibits osteoclast function by blocking the cytokine-induced expression of receptor activator nuclear kappa B ligand (RANKL), is being tried in the pediatric population. 7,28 The preliminary results of these trials suggest that denosumab is a safe and promising treatment for ABC. 28
Within the limitations of our study we may consider that the different treatment modalities used in our patients, separated in small subgroups, make it difficult to outline treatment guidelines for ABC. Additionally, the sample size was relatively small. On the other hand, one of the strengths of the study is that this study presents one of the largest series of pediatric patients with ABC located in the spine to date in published literature.
Conclusion
We consider that in patients with ABC with location in the spine without neurological deficit or suspicion of imminent vertebral instability, nonsurgical treatment, either with intralesional injection with calcitonin and methylprednisolone or with selective embolization, is the management of choice. In patients with aggressive, locally invasive tumors, potential instability of the spine, or neurological deficit, tumor resection associated with instrumented spinal fusion and bone grafting allowed us to control the disease with a lower rate of recurrence and good long-term clinical and radiological results.
Footnotes
Author Contributions
Design of study: LRS, RR, CAT
Consulting references: IAFW, LP, EG, LRS
Participation in draft manuscript: LRS, LP, IAFW, MN
Revision of manuscript: IADFW, CAT, RR, MN, LP
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.