
Abstract
Objective:
The aim of this study was to compare the outcome of after-hours electively planned Posterior Spinal Fusion surgeries for Adolescent Idiopathic Scoliosis (AIS) patients with daytime surgeries.
Methods:
This was a retrospective propensity score-matched study using prospectively collected data. Surgeries performed between 08:00 and 16:59 h were labeled as daytime surgeries (group 1) and surgeries performed between 17:00 and 06:00 h were labeled as after-hours surgeries (group 2). The perioperative outcome parameters were average operation time in and out, operation duration, intraoperative blood loss, blood transfusion, intraoperative hemodynamic parameters, preoperative hemoglobin, postoperative hemoglobin, and total patient-controlled anesthesia (PCA) morphine usage. Radiological variables assessed were Lenke subtypes, preoperative Cobb angle, number of fusion levels, number of screws used, postoperative Cobb angle, correction rate, side bending flexibility, side bending correction index, complications rate, and length of hospitalization.
Results:
Average operation time in for daytime group was 11:32 ± 2:33 h versus 18:20 ± 1:05 h in after-hours group. Comparing daytime surgeries with after-hours surgeries, there were no significant differences (p > 0.05) in the operation duration, intraoperative blood loss, intraoperative pH, bicarbonate, lactate, postoperative hemoglobin, hemoglobin drift, blood transfusion, postoperative Cobb angle, correction rate, side bending flexibility, side bending correction index, length of hospitalization, and complications rate. Total PCA morphine usage was significantly lesser in the after-hours group (18.2 ± 15.3 mg) compared with the daytime group (24.6 ± 16.6 mg; p = 0.042).
Conclusions:
After-hours elective spine deformity corrective surgeries for healthy ambulatory patients with AIS were as safe as when they were done during daytime.
Introduction
Spine deformity corrective surgery for patients with Adolescent Idiopathic Scoliosis (AIS) is a major surgery with potential risk of serious complications or mortality. Neurological complications and non-neurological complications for fusion surgeries in pediatric scoliotic patients were reported to range from 0.5% to 15.4%. 1,2 Therefore, all efforts to maintain the surgical safety for these patients are very important.
Due to constraints of resources, facility, and time, some centers had resorted to performing elective surgeries during after-hours. It is also common to have major elective surgeries that require a longer surgical duration to extend into after-hours. In our center, elective surgeries are allowed to be done after-hours, and therefore, we commonly list and perform elective corrective scoliotic surgeries during after-hours. However, studies had reported that surgeries that were done after-hours led to higher morbidity and mortality. 3 –11 This was perceived that the poorer outcome of after-hours surgeries may be attributed to surgeon fatigue, lack of availability of support staffs, and other logistical facilities and resource factors. 3,6 However, all of these studies were either retrospective studies or studies which included patients who needed emergency surgeries or patients with fractures and other conditions whom were hospitalized for semi-emergency surgeries. None of them exclusively looked into elective surgeries on healthy ambulatory patients. A study by Sessler et al. 12 looked into after-hours elective general surgery and found it to be comparably safe at any time of the workday. However, it only included with the operation starting time from 06:00 to 19:00 h and not any later in the day.
Therefore, the aim of this study was to determine the safety and outcome of after-hours surgeries by analyzing the perioperative outcome of electively planned Posterior Spinal Fusion (PSF) surgeries for healthy ambulatory patients with AIS comparing it with daytime surgeries by using propensity score-matched comparable groups.
Methodology
Study design
This was a retrospective propensity score-matched study using prospectively collected data from 2014 to 2016. Institutional ethical board approval was obtained for this study. The inclusion criteria were AIS patients who had PSF surgery. The exclusion criteria were patients who were undergoing revision surgery, non-idiopathic scoliosis, psychological disorders, metabolic bone disease, and atypical curve patterns not classifiable using the Lenke classification. Surgeries performed between 08:00 and 16:59 h were labeled as daytime surgeries (group 1) and surgeries performed between 17:00 and 06:00 h were labeled as after-hours surgeries (group 2). 5,13 This distinction was made based on the starting time of the surgery. There were no specific criteria or distinction on how the patients were listed as patients were scheduled serially on the next available time slot for surgery whether it was daytime or after-hours.
The preoperative, anesthetic, intraoperative, and postoperative protocols used were similar for both groups. Surgeries for both groups were done by a dedicated spine team that comprised the same anesthetist, nurses, radiographers, surgeons, and assistants. The same sets of equipment and operating room were used. Intravenous tranexamic acid 20 mg/kg was administered to all patients. All patients underwent PSF using alternate level pedicle screw configuration with four to six pedicle screws at lower end (base anchor) and upper end (proximal anchor). Facetectomies were performed to increase the spinal flexibility as well as to facilitate spinal fusion. Reduction was performed using translation and direct vertebral rotation techniques. Fusion was augmented using autogenous local bone graft obtained from facet joints, spinous processes, transverse processes, and decorticated laminae of each instrumented vertebra. Cell salvage autologous blood recovery system was used in all cases (Haemonetics Cell Saver® 5+). Subfascial drains were inserted in all patients and were removed 18–24 h after surgery.
Data collection
The demographic variables were age, gender, weight, and body mass index. The perioperative outcomes parameters were average operation time in and out, operation duration, intraoperative blood loss, blood transfusion, intraoperative hemodynamic parameters, preoperative hemoglobin, postoperative hemoglobin, and total patient-controlled anesthesia (PCA) morphine usage. Radiological variables assessed were Lenke subtypes, preoperative Cobb angle, number of fusion levels, number of screws used, postoperative Cobb angle, correction rate, side bending flexibility, side bending correction index, complications rate, and length of hospitalization.
Propensity score matching
Propensity score matching was used in this study to create comparable groups: group 1 (daytime surgery) and group 2 (after-hours surgery). The propensity score for each parameter was estimated using logistic regression, which created probability scores for each subject. One-to-one matching analysis using “propensity score-matched cohort patient sampling method” was done for age, gender, height, weight, preoperative Cobb angle, number of screws, and Lenke classification. Matched pairs were then created using nearest-neighbor matching without replacement with a match tolerance of 0.05. The outcome measures included operative duration, blood loss, postoperative hemoglobin, need for transfusion, morphine usage, and duration of hospital stay.
Statistical analysis
The procedure required SPSS Version 22.0 (SPSS Statistics for Windows, IBM Corp., Armonk, New York, USA) with Statistics Regression module, FUZZY extension command (Version 1.4.1), and the Python Essentials. In order to compare the outcomes between the matched groups, independent t-test was used for continuous variables, and chi-square test was used for categorical variables. Statistical significance was established at p < 0.05.
Results
A total of 349 AIS patients were operated from January 2014 until December 2016. Among the 349 patients, 108 were operated during the daytime and 241 were operated after-hours. From the 108 patients operated during daytime, 54 patients were matched with the 54 patients who were operated during after-hours using propensity score-matched cohort patient sampling method.
Baseline patient demographics are shown in Table 1. A total of 108 patients were included with 54 patients in the daytime group and 54 patients in the after-hours group. Patients recruited presented with a mean age of 15.0 ± 3.9 and a body mass index of 18.7 ± 3.1 kg/m2. Lenke classification comprises 32.4% of Lenke 1, 26.9% of Lenke 2, 7.4% of Lenke 3, 3.7% of Lenke 4, 21.3% of Lenke 5, and 8.3% of Lenke 6. The average preoperative Cobb angle is 68.9 ± 22.0°. The average number of fusion level is 10.2 ± 2.4, and the average number of screw used is 14.0 ± 2.7. The preoperative hemoglobin level is 13.7 ± 1.3 (g/dL). There were no statistically significant differences in patient characteristics such as age, gender, body mass index, preoperative Cobb angle, number of fusion level, and number of screws used between after-hours and daytime groups.
Demographic data of patients (n = 108).
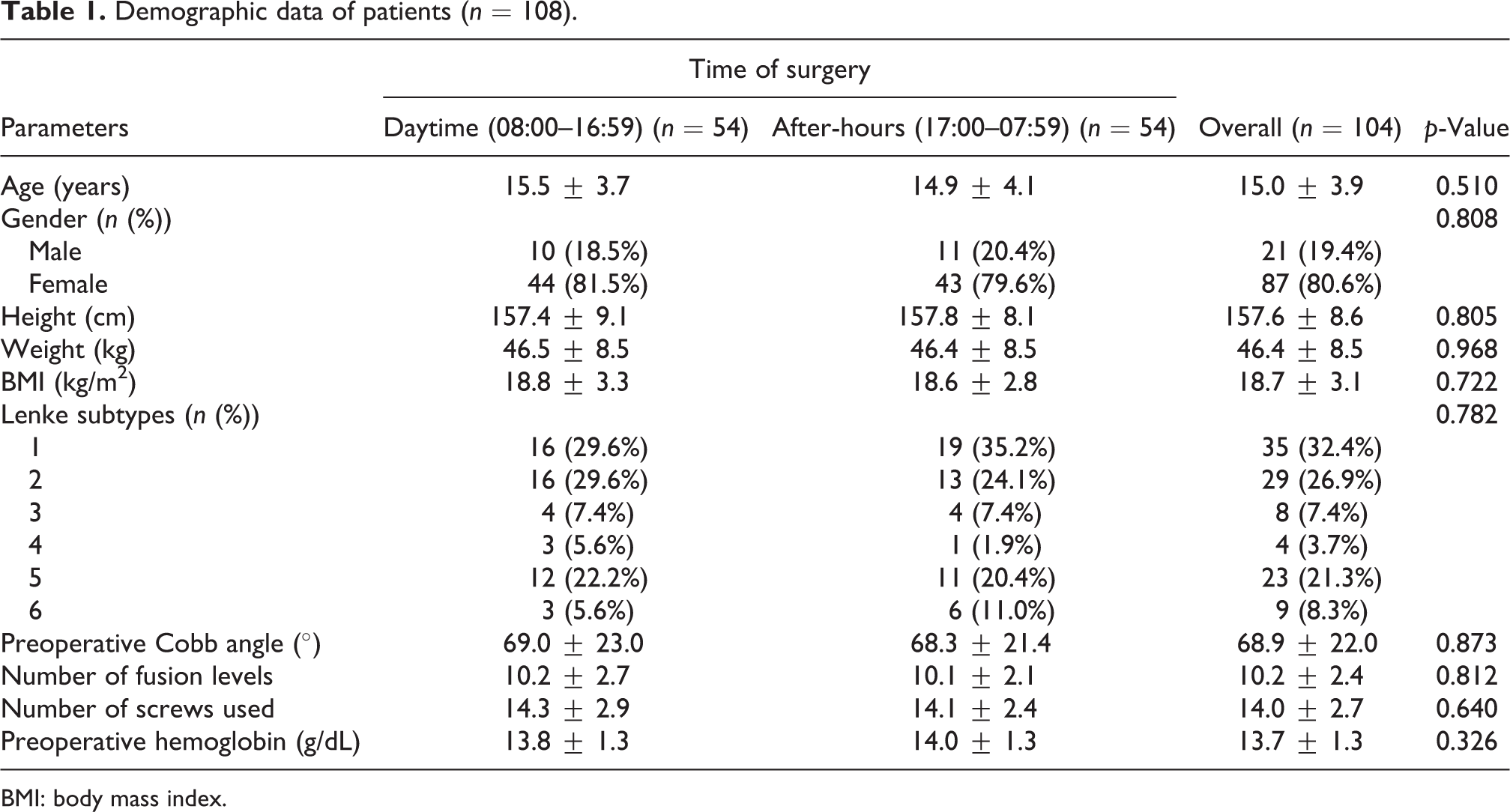
BMI: body mass index.
Perioperative outcome parameters for patients are demonstrated in Table 2. Average operation time in for daytime group was 11:32 ± 2:33 h versus 18:20 ± 1:05 h for after-hours group. There was no significant difference in the operation duration between daytime group (142.1 ± 40.7 min) and after-hours group (137.9 ± 32.9 min; p = 0.553). There was no significant difference in the average intraoperative blood loss between daytime group (983.8 ± 864.9 mL) and after-hours group (992.7 ± 548.0 mL; p = 0.949). Intraoperative pH, bicarbonate, lactate, postoperative hemoglobin, and hemoglobin drift were not significantly different between the two groups. Total PCA morphine usage was significantly lesser in the after-hours group (18.2 ± 15.3 mg) compared with the daytime group (24.6 ± 16.6 mg; p = 0.042). There were two patients who received blood transfusion, each in different groups (p > 0.05). There were also no significant differences between the two groups in terms of postoperative Cobb angle, correction rate, side bending flexibility as well as side bending correction index. The length of hospitalization for both groups was approximately the same with the mean hospital stay of 72.1 ± 9.8 h for daytime and 70.0 ± 10.6 h for after-hours (p = 0.282) groups. There were two complications in the daytime group: One patient had massive hemorrhage and the other patient had superficial wound infection. There were two complications in the after-hours group: Both patients had superficial wound infections. There was no mortality in both groups.
Perioperative outcome parameters for patients (n = 108).
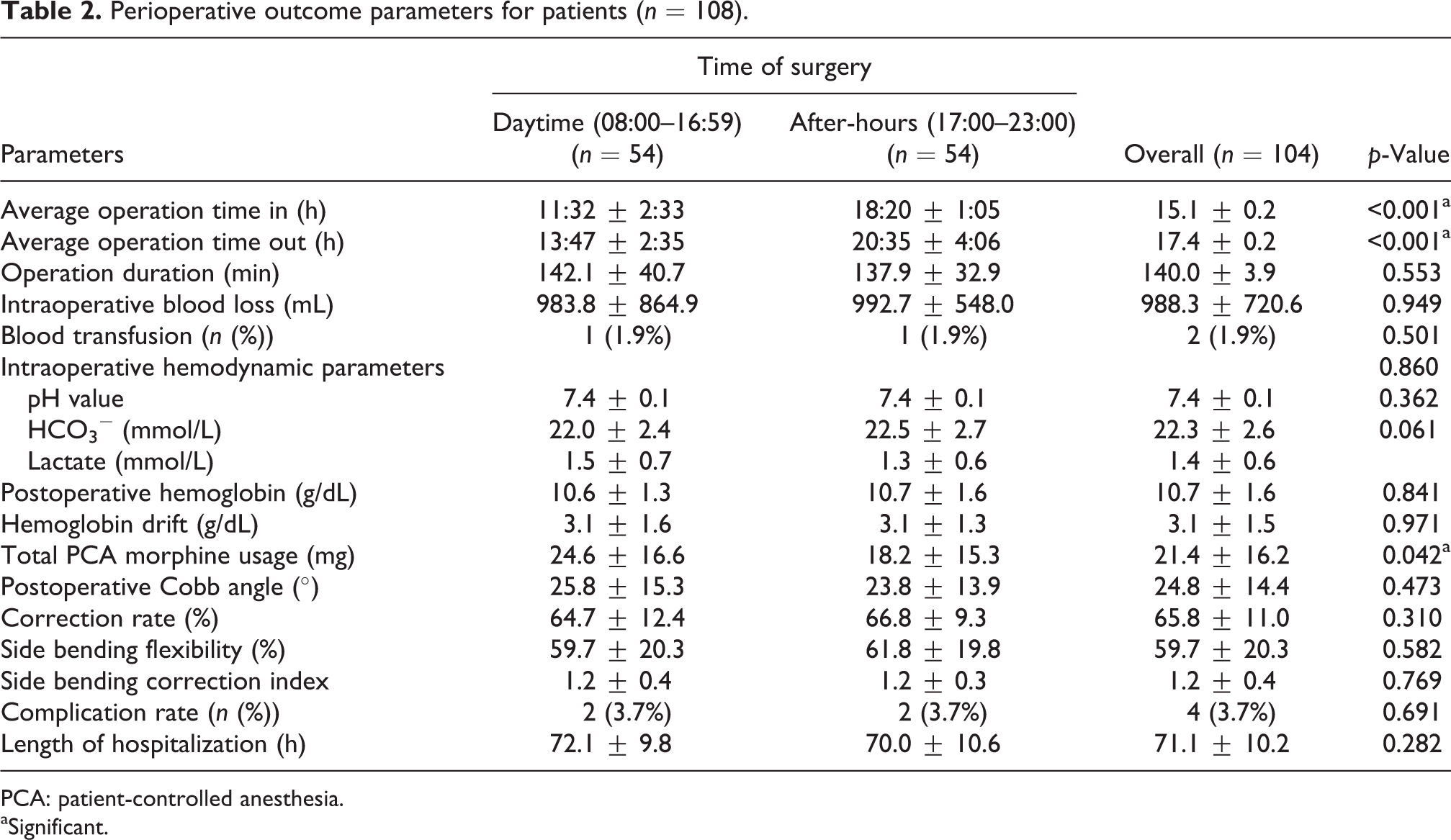
PCA: patient-controlled anesthesia.
aSignificant.
Figure 1 showed the pattern of operation start time. The highest number of patients had their surgeries started between 18:00 and 1900 h (31.5%). This was followed by 09:00–10:00 h (13.0%) and 08:00–09:00 h (9.3%). Only one patient had surgery started between 22:00 and 23:00 h (0.9%).
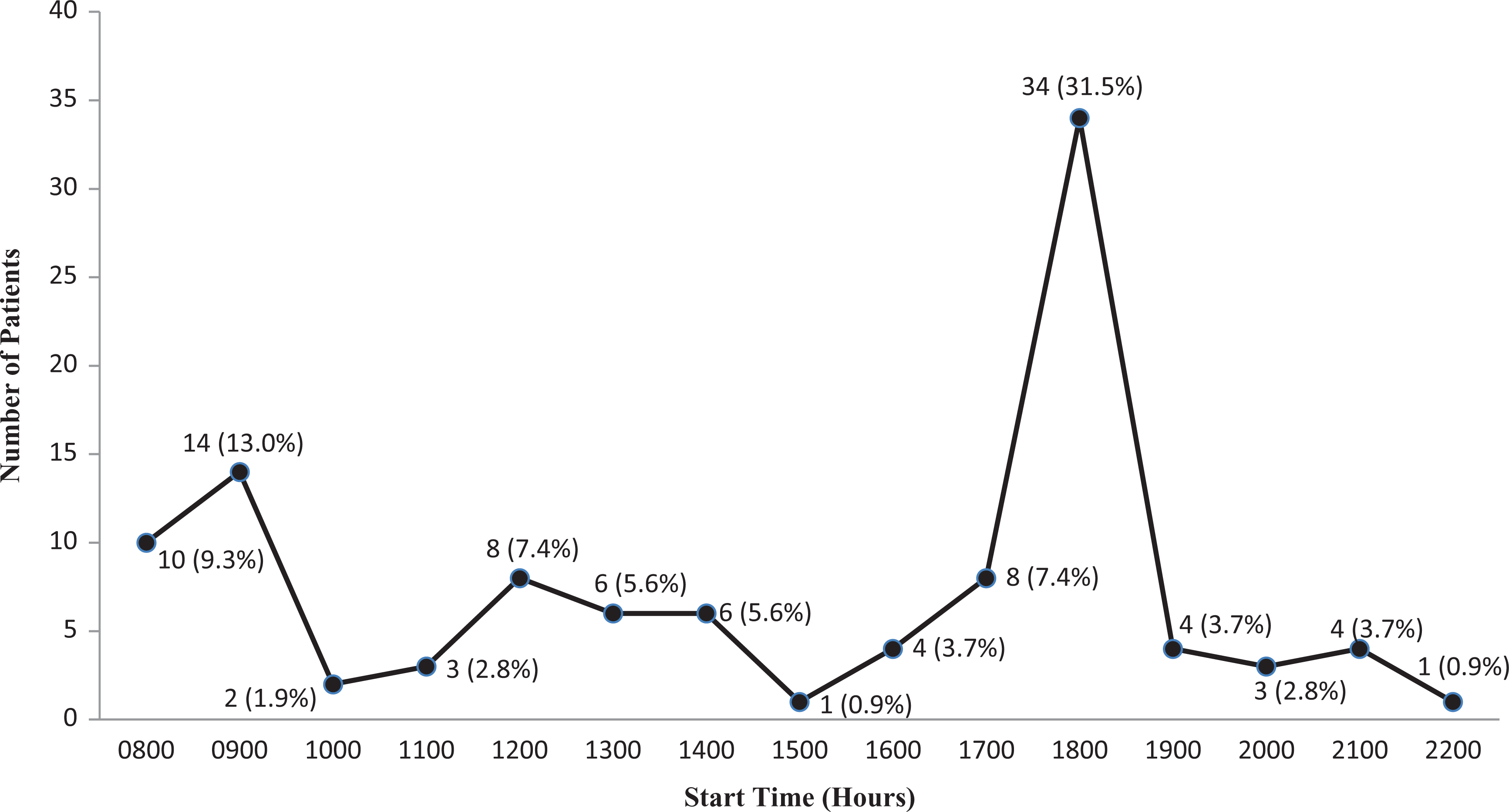
Operation start time and number of patients.
Discussion
There were studies that documented surgeries done after-hours carried higher morbidity and mortality. 3 –11 Chacko et al. 3 performed a retrospective study of 767 consecutive patients with intertrochanteric, subtrochanteric, or femoral neck fractures and found that the duration of surgery, blood loss, and postoperative mortalities were significantly less for surgery done during the day compared with night. Ricci et al. 4 conducted a prospective study among 203 patients with femur and tibia fractures comparing surgeries done at daytime and after-hours. They found that the rates of nonunion, infectious complications and radiation exposure were similar, but after-hours femoral nail fixation was associated with an increased frequency for the removal of painful hardware. They concluded that daytime surgery has the potential to reduce minor complication rates for intramedullary nail fixation. Aydogmus et al. 5 found that among 91 patients with Gartland type 3 fractures, pediatric supracondylar humerus fractures, after-hours surgery resulted in higher poor fixation rate compared with daytime surgery. Kelz et al. 6 reported a retrospective study of 144,740 nonemergent general and vascular surgical procedures, comparing the operation start time of 7 a.m. to 4 p.m., 4 p.m. to 6 p.m., and 6 p.m. to 11 p.m. and found that morbidity was significant higher when the operation start time was later in the day. Desai et al. 7 performed a retrospective study on 710 urgent or emergency pediatric neurosurgical procedures and found that 30-day morbidity and mortality were significantly higher when these procedures were done during the weekend or after-hours. Komen et al. 8 found that anastomosis leakage was significantly higher among patient who underwent a primary colorectal anastomosis operation during after-hours compared with daytime. Dalton et al. 9 found that acute care emergency trauma and general surgery done at night was a potent predictor of mortality. Phatak et al. 10 found that nonelective nighttime laparoscopic cholecystectomies are associated with increased postoperative complications. Saleem et al. 11 reported that hospital mortality was higher in patient who had percutaneous transluminal coronary angioplasty for acute myocardial infraction during off-normal hours compared with normal hours. None of these studies included elective surgery on healthy ambulatory patients.
More recently, some studies have found that there were no differences in the mortality and morbidity rates between daytime and after-hours surgeries. 13 –17 Rashid et al. 13 retrospectively reviewed 220 dynamic hip screws performed for intertrochanteric fractures and found that there was no difference in the rates of wound infection, length of hospital stay, postoperative ambulation status, intraoperative blood loss, type of anesthesia, and mortality between daytime and after-hours surgeries. Switzer et al. 15 performed a retrospective review on 859 with hip fractures and found that surgical time of day did not affect 30-day mortality or total number of complications. Fernandez et al. 14 found that among patients with acute colorectal disease subjected to urgent surgery, there was no significant association between nighttime surgery and the presence of postoperative medical and surgical morbidities. Zafar et al. 16 found that trauma surgery during the night did not have an increased mortality when compared with surgery during the day. Turrentine et al. 17 found that patients undergoing nonemergent general and vascular surgery procedures at night do not seem to be at an increased risk for postoperative morbidity or mortality. However, all of these studies were retrospective studies on patients who had fracture or had included patients who required emergency surgery, and none of them had matched comparable group that looked exclusively into elective major surgical procedures.
This study looked into elective corrective PSF surgery on healthy ambulatory patients with AIS. It compared propensity score-matched comparable groups between patients who had surgeries done during daytime and after-hours. We found that there are no significant differences between perioperative outcome parameters for PSF performed during daytime and after-hours. Time of surgery did not affect the duration of operation, intraoperative blood loss, the rate of blood transfusion, intraoperative hemodynamic parameters, postoperative hemoglobin levels, hemoglobin drift, complications rate, and the length of hospitalization. The surgical correction parameters such as postoperative Cobb angle and correction rate were also not affected by the time of surgery. This may be due to the fact that planned elective major surgeries had less risk of unexpected of unpredictable problems compared with unplanned emergency surgeries. We also noted that after-hours surgery had lesser total PCA morphine usage compared with daytime surgery. This may be attributed to the more likelihood of patients having less pain while sleeping throughout the night following after-hours surgery as compared to surgery done during daytime. We therefore postulate that after-hours elective corrective PSF surgery on healthy ambulatory patients with AIS by a dedicated spine team had similar safety and outcome as of daytime surgery.
There were several limitations in this study. This study did not have any patients who had surgery starting time after 23:00 h and thus may only represent the earlier phase of after-hours and not the later phase of after-hours. The negative effects of surgeon fatigue, lack of availability of support staffs, and other logistical facilities and resources factors in after-hours surgeries may be more prominent in the later phase of after-hours and not in the earlier phase of after-hours. This study only looked into PSF surgery for patients with AIS and had not included more complex deformity surgeries that have higher demand on surgeons and support staffs. We also did not study the differences in satisfaction of patients and parents between daytime and after-hours groups.
In conclusion, we found that there was no significant difference in the perioperative outcome and safety between daytime and after-hours surgeries for PSF surgeries. After-hours elective spine deformity corrective surgeries for healthy ambulatory patients with AIS done by a dedicated spine team were as safe as when those done during daytime.
Footnotes
Acknowledgements
We would like to acknowledge Miss Devinder Kaur D/O Joginder Singh, Mr Low Yee Kok, Mrs Diana Gatot, and all medical record department staff for their contribution in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.