
Abstract
Combined lateral condyle mass and olecranon fractures are infrequently seen. These cases are easily missed, and only 12 previous cases are detailed in the English medical literature. The decision for surgical fixation usually depends on the amount of displacement of the individual fractures. However, the optimal surgical approach or technique for open reduction and internal fixation has not been agreed upon. We present three original case reports and analyse them together with all other known cases in the English literature. We discuss how to avoid missing these combined fractures and propose a treatment algorithm based on the different permutations of the fracture displacement. Our detailed surgical approach (using a posterior ‘olecranon osteotomy’ approach) is also described.
Introduction
Individually, lateral condyle fractures of the humerus account for 17–34% of all elbow fractures in children 1 –4 and olecranon fractures about 5–7%. 3 –5 The combination of concomitant lateral condyle mass and olecranon fractures in the same elbow occurs even more infrequently.
A Scandinavian epidemiological study of childhood fractures showed one case out of 589 fractures in children aged 0–16. 6 Another study from the United Kingdom showed 8 cases out of 2502 elbow injuries. 7 Isolated case reports 8 –11 and a series of cases collected by Sharma et al. 7 tell us that these cases are easily missed, and they are invariably troubled by elbow stiffness during their recovery.
We combine our case series with existing information from literature review. This article discusses how to avoid missing these combined fractures, and we also present our treatment algorithm as well as a detailed surgical approach (using a posterior ‘olecranon osteotomy’ approach) towards this rare combination of fractures.
Materials and methods
Electronic medical records and radiographs of our three cases were reviewed. A thorough literature review was then performed on PubMed looking for combined or associated lateral condyle and olecranon fractures in children, and we attempted to summarize all existing available cases in the English literature for this rare injury combination. Four individual case reports 8 –11 and a case series of eight patients 7 were identified. There has been a mention of combined lateral condyle and olecranon fractures in several series, but a lack of clinical details prevented them from being used in this analysis. 12 –14
Case reports
Case 1
Our patient is an 8-year-old girl who fell from a monkey bar apparatus in the playground onto her right elbow. She presented to the emergency department with pain and swelling over her right elbow. Physical examination showed tenderness over the olecranon and lateral distal humerus. Bruising was also noted laterally. There were no open wounds and no distal neurovascular deficits.
Preoperative radiographs are shown in Figure 1, which show displaced lateral condyle humerus and olecranon fractures.
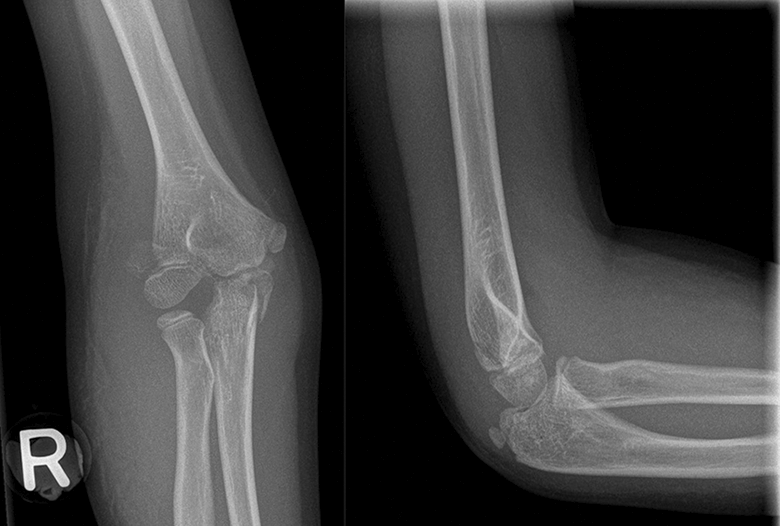
Preoperative radiographs.
An open reduction and percutaneous pinning of the lateral condyle humerus fracture and a tension band wiring of the olecranon fracture were performed via a posterior ‘olecranon osteotomy’ approach on the same day.
There are only four previous cases of displaced lateral condyle with concomitant displaced olecranon fractures reported in the English literature. All cases have been treated surgically. However, the surgical approach and choice of fixations all differ. We present details of our surgical approach, making use of the posterior ‘olecranon osteotomy’ approach to the elbow to get accurate reduction of both the intra-articular fractures. We believe that this approach is optimal, as it allows direct vision of the articular surfaces of both the lateral condyle and the olecranon, while using the olecranon fracture to our advantage.
Figure 2 shows the preoperative positioning of the patient. The patient lies supine and is brought to the edge of the bed. A pillow is then taped across her chest. An image intensifier machine can then come in either perpendicular or parallel to the bed.

Positioning and planning of skin incision.
After the skin incision is placed, and periosteum stripped, the displaced olecranon fracture is seen (see Figure 3(a) to (d)). The olecranon fragment is easily retracted to the medial side to expose the articular surface of the lateral condyle fracture. A pointed reduction forceps is then used to reduce the lateral condyle fracture anatomically under direct vision. Once reduction is obtained, two percutaneous 1.6 mm K-wires are placed across the lateral condyle fracture site in a divergent manner. The olecranon fragment is then reduced, and a tension band wire construct is placed across the olecranon fracture. See Figure 4.
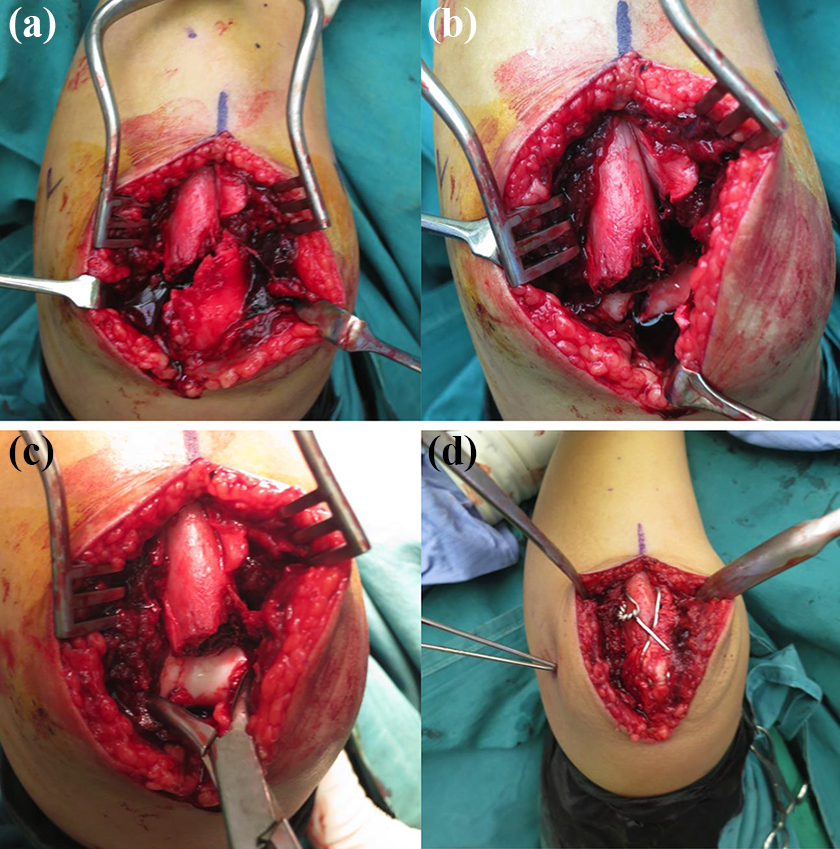
(a) After the skin incision is placed, the displaced olecranon fracture is seen. (b) The olecranon fragment is easily retracted to the medial side to expose the articular surface of the lateral condyle fracture. (c) A pointed reduction forceps is used to reduce the lateral condyle fracture anatomically under direct vision. (d) Once reduction is obtained, two percutaneous 1.6 mm K-wires are placed across the lateral condyle fracture site, and a tension band wire construct is placed across the olecranon fracture.
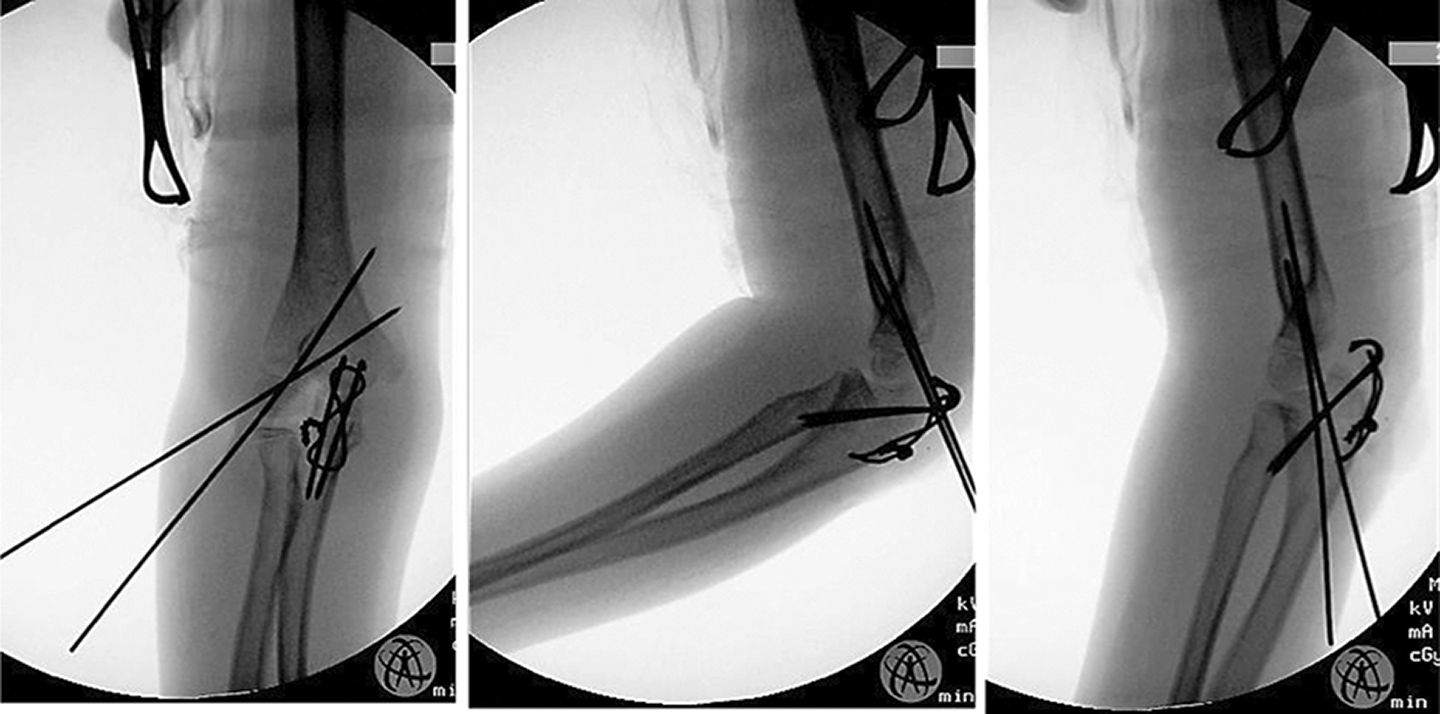
Intraoperative radiographs showing stability of fractures in flexion and extension of elbow.
Post-operatively, she was protected in an above-elbow cast for 4 weeks. The lateral condyle K-wires were removed in clinic at 4 weeks post-op, and the tension band wire was removed in the operating theatre at the 12-week mark. There was some stiffness of the elbow encountered initially, with lack of terminal extension. However, this normalized and she regained full range of motion in her left elbow at 4 months post-operatively.
Case 2
This is an 8-year-old girl who had been playing on the mattress with her brother. She fell onto the mattress on her left flexed elbow, and her brother subsequently fell and landed on her. She presented with left elbow pain and swelling. Physical examination showed tenderness over the olecranon and lateral distal humerus. There were no open wounds and no distal neurovascular deficits.
Radiographs (Figure 5) show a Milch-I displaced lateral condyle humerus fracture and an undisplaced fracture of the olecranon.

Radiographs of case 2 showing Milch-I displaced lateral condyle humerus fracture and an undisplaced fracture of the olecranon.
The patient was brought to the operating theatre for an open reduction and percutaneous pinning of the lateral condyle humerus fracture via a lateral approach. The olecranon fracture was then assessed for stability via intraoperative radiographs, and the decision was made to treat it without any fixation (see Figure 6).

Intraoperative radiographs showing stability of both the lateral condyle and the olecranon fractures after fixation of the lateral condyle fracture.
She was managed in an above-elbow cast for 4 weeks post-operatively. The cast and percutaneous wires were removed in the outpatient clinic on the 4th week post-operation. At the 2-month review, her elbow range of motion was from 20° to 130°. Pain-free, full range of motion of the elbow was achieved at the 3-month review. Final radiographs at 5 months post-injury (Figure 7) showed complete healing of both fractures.

Final radiographs of case 2 at 5 months post-injury.
Case 3
Our patient is a 2-year-old girl who presented with a deformed right elbow after a fall onto her outstretched right hand. She had been standing on her bed of about 1-m height when she fell from the bed. The right elbow was noted to be very swollen, but there was inadequate assessment and documentation of the areas of tenderness over the elbow.
Radiographs show both displaced lateral condyle humerus and olecranon fractures (See Figure 8). However, the olecranon fracture was not diagnosed initially.

Radiographs showing both displaced lateral condyle and olecranon fractures (inset arrows).
The child was brought into the operating theatre on the same day for an open reduction and internal fixation of the lateral condyle fracture via a posterolateral approach. Intraoperative radiographs are shown in Figure 9. Intraoperatively, reduction of the lateral condyle fracture was noted to be much more difficult to obtain and maintain than usual. We postulate that this could be due to the mobile olecranon fragment.

Intraoperative radiographs after open reduction and internal fixation of the lateral condyle fracture. The olecranon fracture was still not diagnosed at this point.
Post-operatively, the child was kept in an above-elbow cast. The radiographs at 1 month (Figure 10) showed callus over the olecranon fracture, thus confirming the presence of a concomitant olecranon fracture. The cast was removed after 1 month.

Radiographs at 1 month post-injury, showing healing fractures of both the lateral condyle of the humerus and the olecranon.
She achieved full range of motion in her right elbow at the 3-month review. Follow-up radiographs, however, showed avascular necrosis of the capitellum (See Figure 11). This could have resulted from the severe displacement from the initial injury or due to an increased amount of soft tissue dissection that was needed to obtain reduction.

(a and b) Radiographs at 3 months post-injury show the appearance of avascular necrosis of the capitellum. (c and d) Radiographs at 1 year show some re-ossification of the capitellum.
During follow-up, she remained asymptomatic from the capitellar avascular necrosis. Radiographs at the 1-year follow-up showed some re-ossification of the capitellum. She is planned for the removal of the wires.
Discussion
There are only 15 (including 3 contributions from this article) combined lateral condyle mass and olecranon fractures that are detailed in the English literature to date. While occasional mention has been made of these fractures from some other case series, the lack of clinical details limits us from analysing them gainfully. A summary of these 15 cases is shown in Table 1.
Summary of published cases of combined lateral condyle humerus and olecranon fractures.a

M: male; F: female; FOOSH: fall-on-outstretched hands; LC: lateral condyle; OC: olecranon; ORIF: open reduction and internal fixation; CRPP: closed reduction and percutaneous pinning; TBW: tension band wire; OR: open reduction; PP: percutaneous pinning; AVN: avascular necrosis; ROM: range of motion.
a The boldfaced text refers to the cases that were initially missed. This resulted in differences in surgical plans and eventual outcomes.
Easily missed diagnosis
The combined lateral condyle mass and olecranon fractures are easily missed. From the 15 known cases in the English medical literature, 3 cases (20%) were initially missed. The three fractures that were missed included two displaced olecranon fractures and an undisplaced lateral condyle fracture. The key to identifying these fractures is to have awareness and a heightened index of suspicion. When encountering a fracture in the paediatric elbow, it is necessary to clinically exclude a concomitant fracture. This can be done by direct palpation over the bony prominences over the elbow, namely the lateral condyle, medial epicondyle, olecranon and radial neck. Where tenderness is elicited both over the olecranon and the lateral condyle, proper AP and lateral radiographs should be obtained. In cases where the diagnosis is still not clear, oblique radiographs could be useful as well. In case 3 where the olecranon fracture was missed, there was inadequate assessment and documentation of the areas of tenderness over the elbow.
Mechanism of injury
From the available cases, two mechanisms of injury have been identified. One is the classic fall-on-outstretched hand (FOOSH), usually from a height. The second mechanism is that of a fall and direct impact on a flexed elbow. Interestingly, all the fractures that resulted from a FOOSH mechanism were displaced. Unfortunately, details of the mechanism of injuries were not available for the eight patients in Sharma et al.’s series. 7
Complications
From the cases identified, we have encountered the following complications. Stiffness. Almost all patients needed at least 3–6 months before they recovered full range of motion in their elbows. One patient had a residual loss of 10° of terminal elbow extension.
7
Late displacement of lateral condyle fracture resulting in 5° of cubitus varus. This complication was noted in the case report from Cattle and Hemmadi.
10
Missed diagnosis resulting in additional incisions during surgery.
9
Avascular necrosis of the capitellum
Treatment algorithm
We propose a treatment algorithm based on the various fracture patterns that have been encountered. All fractures that show more than 2 mm displacement should be reduced anatomically and fixed surgically. This algorithm is shown in Figure 12.
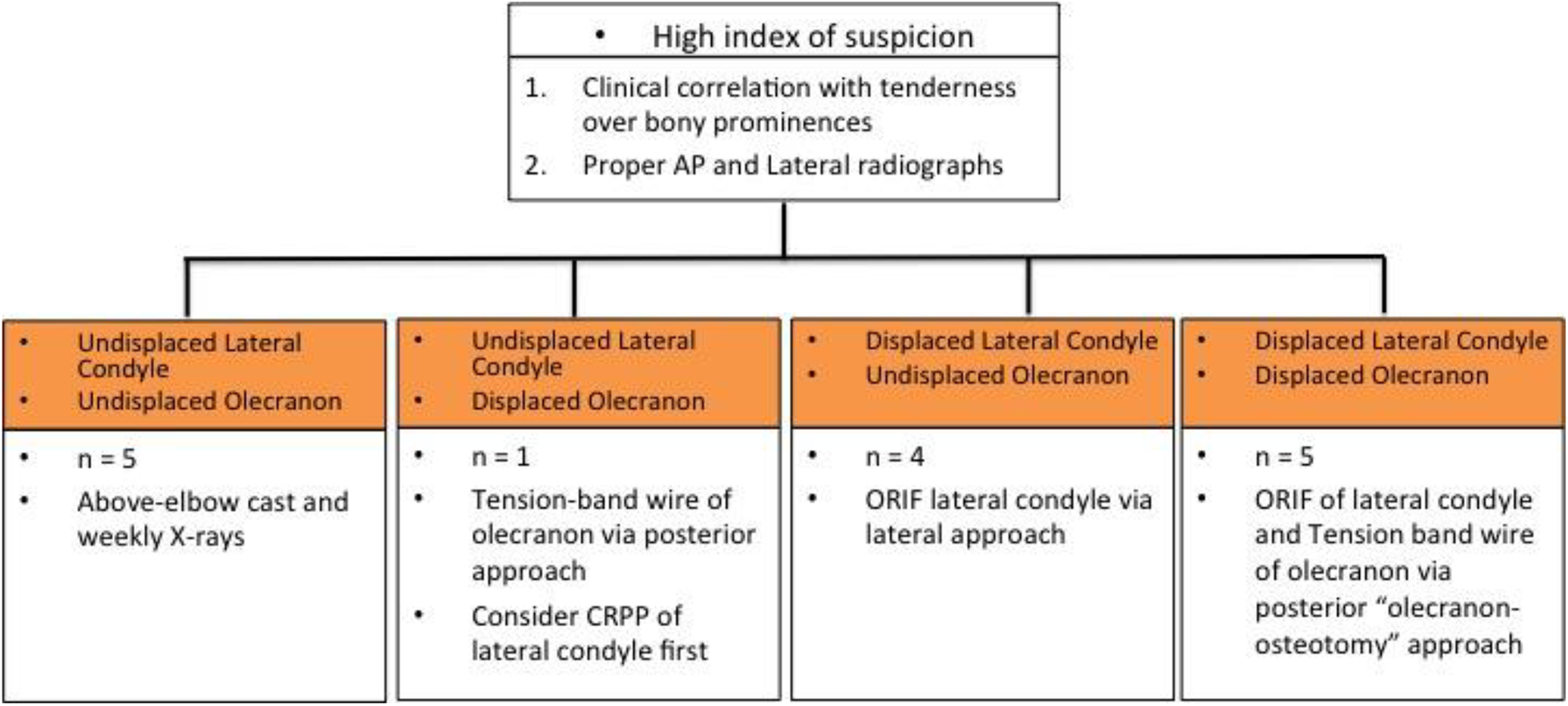
Treatment algorithm for combined lateral condyle humerus and olecranon fractures. ORIF: open reduction and internal fixation.
Where both the lateral condyle and olecranon fractures are undisplaced, these injuries can be safely treated in an above-elbow cast. We suggest weekly radiographs for the first 2 weeks to monitor for any subsequent fracture displacement.
The group consisting of an undisplaced lateral condyle fracture with a displaced olecranon fracture is the most infrequently seen. In the only known case to date, the olecranon was fixed surgically, but the patient presented with a 5° cubitus varus after 15 months. We propose a tension band wiring for the olecranon fracture via a posterior approach for these patients. We would also suggest percutaneous pinning of the lateral condyle fracture prior to the olecranon fixation. This is to prevent any late-onset lateral condyle fracture displacement.
For fracture patterns that have a displaced lateral condyle, and an undisplaced olecranon fracture, our treatment algorithm is to proceed with an open reduction and internal fixation with K-wires of the lateral condyle fracture via a lateral approach. The undisplaced olecranon fracture is then assessed for stability and may be left without any fixation as it is less prone to late displacement when compared to the lateral condyle.
The final group consists of displaced lateral condyle and displaced olecranon fractures. We propose an open reduction and internal fixation (with K-wires and tension band wiring) via a posterior ‘olecranon osteotomy’ approach as detailed in the case 1 report earlier in this article. This approach makes use of the existing olecranon fracture to gain access to the articular surface of the elbow joint, allowing anatomical reduction of both fractures under direct vision.
Summary
Despite increasing reports from across the world on this infrequent injury combination, our knowledge of these fractures is still quite limited. By collating the experience of all the previous authors, we hope that our proposed treatment algorithm can give guidance on the management of future cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.