
Abstract
Background:
In this study, we assessed functional outcomes among olecranon fixation techniques used following transolecranon approach in patients with comminuted fracture of distal humerus.
Methods:
The study included 37 elbows that underwent olecranon osteotomy due to distal humerus fracture. Functional outcomes were assessed among patients who underwent fixation via tension band technique, plate, or screw fixation.
Results:
The implant irritation was seen in 18% of patients who underwent K-wire plus tension band fixation, in 75% of patients who underwent olecranon plate plus screw fixation, and in 18% of patients who underwent cancellous screw fixation. The rate for implant removal was 2.6 folds lower in K-wire plus tension band fixation when compared to olecranon plate plus screw fixation.
Conclusion:
We concluded that K-wire plus tension band technique and cancellous screw fixation performed in accordance with technical principles caused less skin problem when compared to other techniques. In olecranon fixation, both methods with enhanced stability by tension band can be preferred.
Introduction
Elbow movements are highly important to achieve daily activities. Fractures involving elbow joint can cause severe functional loss if not treated appropriately.
Although preliminary papers regarding distal humerus fractures date back until Hippocrates, there is no publication until 17th century in this issue.
The first original work on elbow injuries was published by Desault in 1811. In that study, Desault emphasized that treatment is challenging in distal humerus fractures and that outcomes are not satisfactory. In 1910, Albin Lambotte emphasized the importance of internal fixation in the treatment of distal humerus fractures and described surgical techniques. 1 In 1969, Riseborough and Radin recommended not performing surgical treatment in these fractures, 2 leading an ongoing debate questioning surgical treatment regarding whether conservative or surgical treatment is more appropriate in the treatment. However, the poor outcomes by insufficient internal fixation ability in that era caused a negative approach to surgical treatment. 3,4
In recent years, surgical treatment is commonly recommended by advancing technology and better understanding of elbow anatomy and therapeutic approaches. 5 –7 In this study, it was aimed to compare tension band fixation and olecranon plate plus screw fixation regarding functional outcomes, pros and cons and superiority in patients treated for AO/ASIF type C (Association for Osteosynthesis/Association for the Study of Internal Fixation) intra-articular distal humerus fractures via transolecranon approach.
Material and methods
This research has been approved by the IRB (Institutional Review Board) of the authors. The study included 37 elbows from 36 patients with AO/ASIF type C distal humerus fracture who were treated with olecranon osteotomy and had minimum follow-up of 6 months between January 2010 and March 2015. The patients were reviewed retrospectively.
The data regarding age, gender, mechanism of injury, Gustilo–Anderson classification of open fractures, comorbid pathology, time to surgery, fixation method, olecranon fixation method, duration of immobilization, complications, and additional surgical intervention were extracted from patient files. In final control visit, pain, stability, range of motion in elbow, and daily activities (nutrition, personal hygiene, combing, wearing shirt, and wearing shoes) were questioned by using MAYO Elbow performance scoring system.
Surgical treatment
All patients were operated with fluoroscopy assistance under general anesthesia by using pneumatic tourniquet. The operation was performed at lateral decubitus position while elbow was at 90° flexion. The surgery site was cleansed. The open fractures were flushed by using minimum 5 l of normal saline and then cleansed by using antiseptic solutions. Antibiotic prophylaxis was given before the application of pneumatic tourniquet. At posterior aspect of elbow, a longitudinal incision was made beginning from 10 cm proximal until 5 cm distal to olecranon. Attention was given not crossing incision perpendicular to top of olecranon. The skin and subcutaneous tissues were dissected (Figure 1(a)).
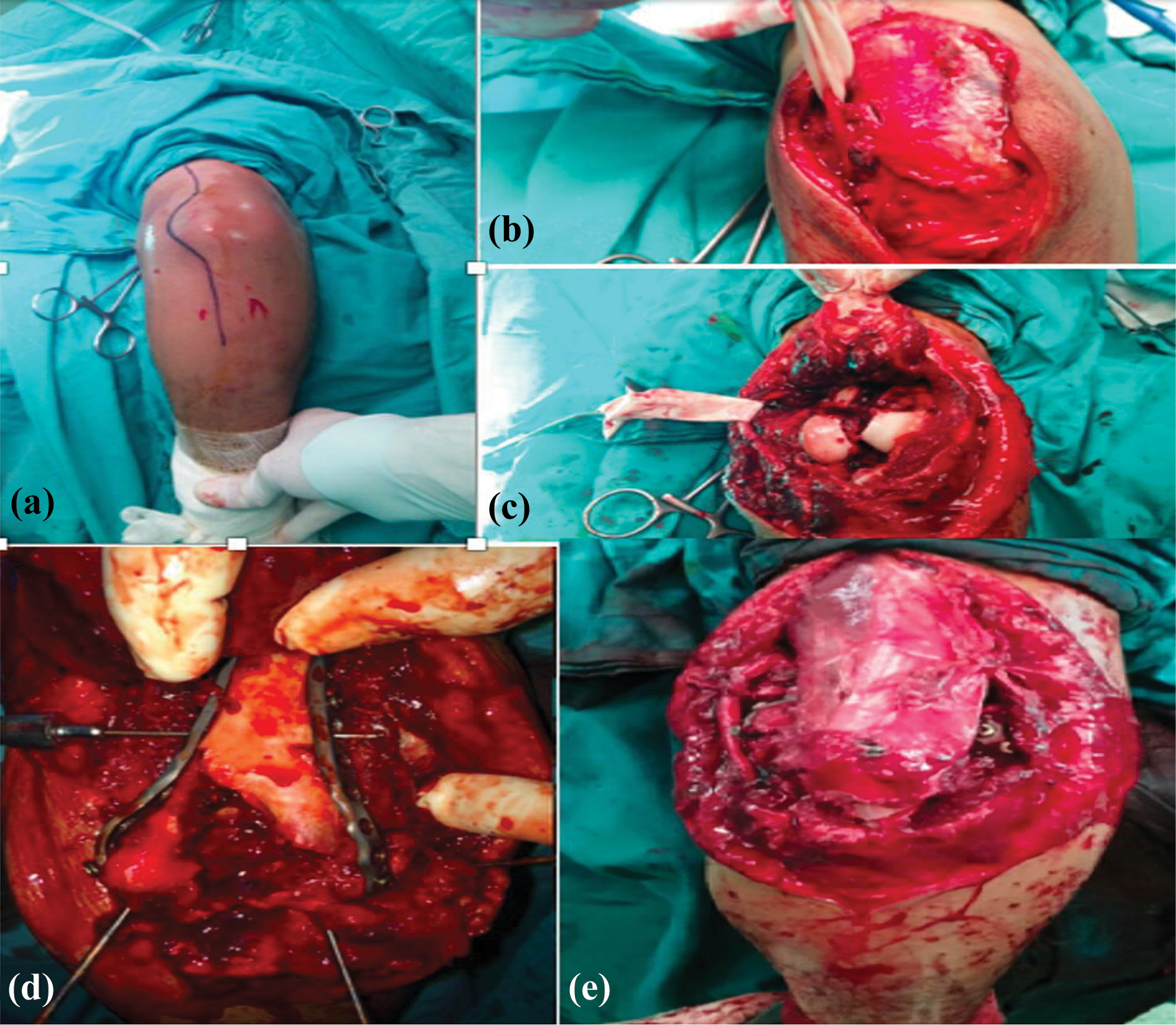
(a) Incision for posterior approach in elbow, (b) ulnar nerve exposure and dissection, (c) elbow joint following osteotomy, (d) articular restoration and fixation to proximal segment, and (e) olecranon osteotomy following re-fixation.
Then, ulnar nerve was exposed and dissection was performed at both proximal and distal parts of ulnar nerve. The ulnar nerve was suspended in order to preserve nerve (Figure 1(b)). Before osteotomy, an intramedullary drill was made and K-wire was inserted, providing reference for reduction after osteotomy. Osteotomy was performed by inverse V-type Chevron osteotomy technique (Figure 1(c)). To avoid bone loss at articular surface, we began osteotomy by a fine saw, which then completed by using a sharp osteotome.
The joint was exposed following osteotomy. After intensive debridement of intra-articular area, distal fragments were combined in accordance to AO principles. Then, the combined fragments were temporarily fixed to proximal segment by using K-wire. The fixation was completed by using plates (and 3–5 mm screws) compatible to distal humerus (Figure 1(d)). After reduction of distal humerus, transolecranon osteotomy was fixed by using tension band plus K-wire or plate plus screw (Figure 1(e)). In all patients, elbow radiographs were obtained after surgery (Figures 2 to 4). No routine anterior transfer was used for ulnar nerve; rather, it was used if there was contusion or implant that might cause compression. Finally, tourniquet was removed and hemostasis was achieved. All subcutaneous and cutaneous layers were completed. A long-arm splint was applied.

Screw fixation of olecranon osteotomy.

Tension band fixation of olecranon osteotomy.
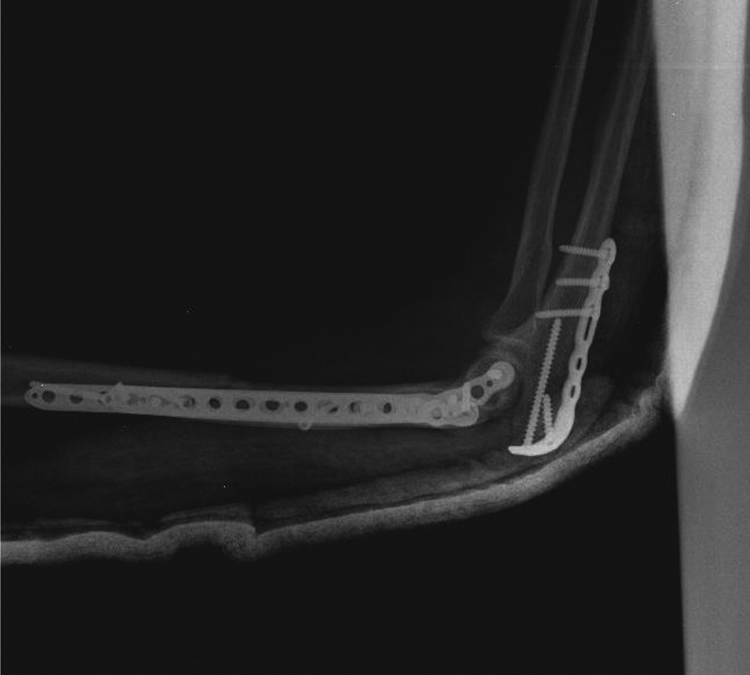
Plate fixation of olecranon osteotomy.
Statistical analysis
Regression analysis and χ2 test were used to assess relationships between categorical variables. Fisher’s exact and Yates and Pearson χ2 test were used when expected frequencies were <5, 5–25, or >25 in χ2 independent test, respectively. The likelihood ratio values were included when expected frequencies were disproportional. Descriptive statistics are expressed as mean ± standard deviation for numerical variables and count (%) for categorical variables. All statistical analyses were performed by SPSS for Windows version 22.0. A p value <0.05 was considered as statistically significant.
Results
In our clinic, 36 patients with distal humerus fracture involving elbow were treated by open reduction plus internal fixation via transolecranon approach between 2010 and 2015. Of the patients, 12 (32.4%) were women whereas 25 (67.6%) were men. The fracture was in right elbow in 21 (56.8%) and in left elbow in 14 (40.5%) while there was bilateral fracture in 1 patient (2.7%). Of the patients, 12 (32%) were aged 18–29 years whereas 11 (29%) aged 30–41 years, 6 (16%) aged 42–53 years, 4 (10%) aged 54–65 years, and 4 (10%) aged ≥65 years.
There was closed fracture in 25 patients (67.6%) and open fracture in 12 patients (32.4%). According to Gustilo–Anderson classification, there was type 1 open fracture in seven patients (18%), type 2 open fracture in four patients (10%), and type 3 open fracture in one patient (2.7%).
The fracture was caused by traffic accident in 13 patients (35.1%), fall from height in 9 patients (24.3%), firearm injury in 8 patients (21.6%), and simple fall in 7 patients (18.9%). According to AO/ASIF classification for distal humerus fractures, there were 6 type C1 fractures (16.2%), 10 type C2 fractures, and 21 (56.8%) type C3 fractures.
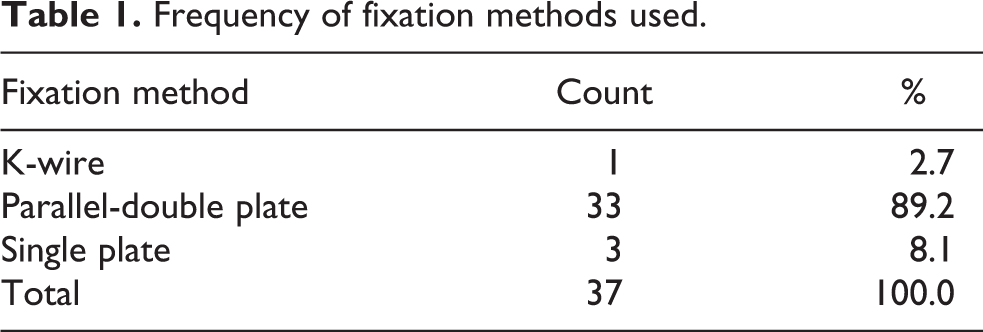
There were comorbid injuries in eight patients (21.6%). Fifteen patients (40.5%) underwent surgery within first day whereas 4 patients (10.8%) within first 3 days, 10 patients (27%) within 7 days, and 8 patients (21.6%) within 10 days. For fixation, parallel-double plate was used in 33 patients (89.2%), single plate in 3 patients (8.1%), and K-wire in 1 patient (2.7%) (Table 1).
Frequency of fixation methods used.
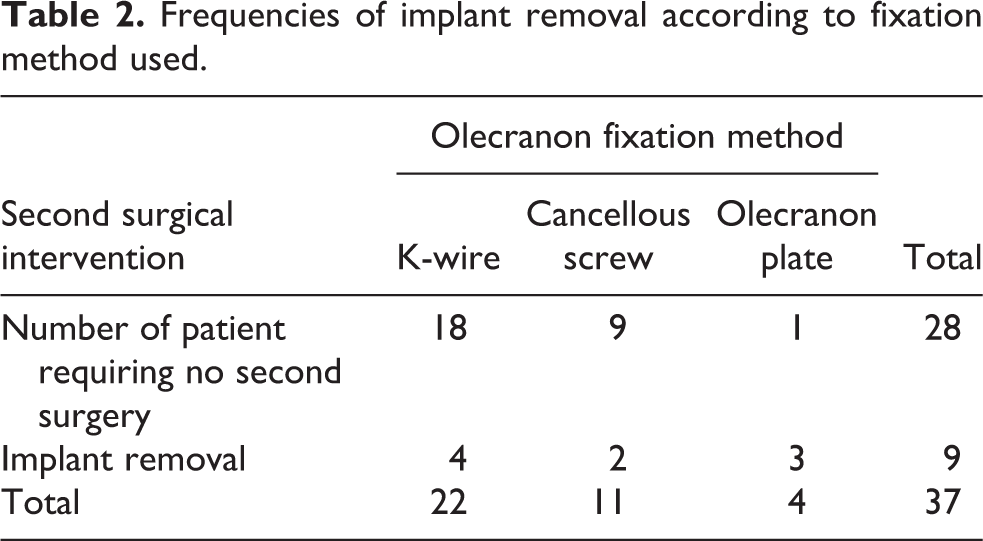
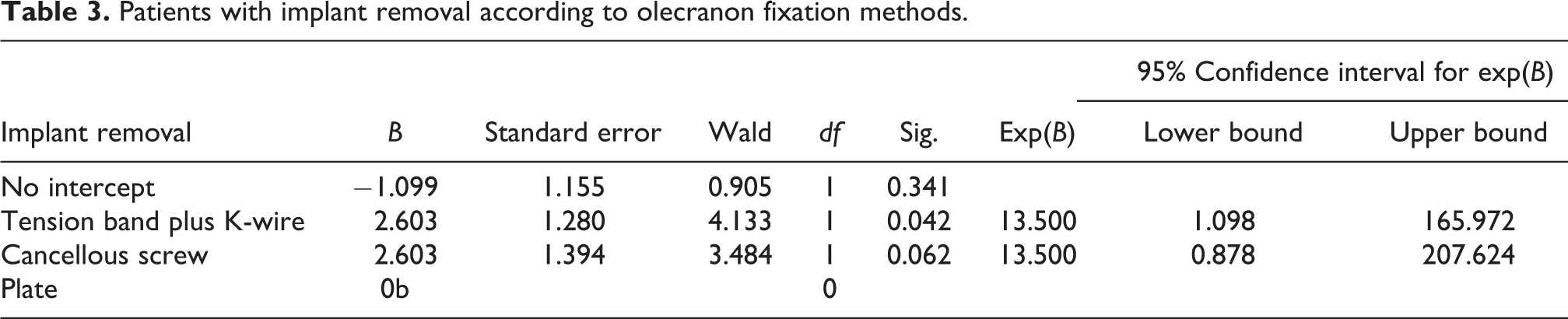
Olecranon osteotomy re-fixation was performed by using tension band technique in 22 patients (59.5%), screws in 11 patients (29.7%), and olecranon plate in 4 patients (10.8%). No additional surgical intervention was performed in 28 patients (75.7%). Implant was removed in nine patients (24%) 4–9 months after surgery as olecranon implants caused skin irritation. Implant was removed in 4 (18%) of 22 patients who underwent tension band plus K-wire fixation, in 3 (75%) of 4 patients who underwent plate fixation, and in 2 (18%) of 11 patients who underwent screw fixation because of skin irritation by material used for olecranon fixation. It was found that the need for implant removal was 2.6 folds lower in K-wire plus tension band fixation when compared to olecranon plate fixation, indicating significant difference (p = 0.042). We also found that the need for implant removal was 2.6 folds higher in plate fixation when compared to screw fixation but the difference did not reach statistical significance (p = 0.062) (Tables 2 and 3).
Frequencies of implant removal according to fixation method used.
Patients with implant removal according to olecranon fixation methods.
No early or delayed complication was seen in 34 patients (91.9%). However, soft tissue infection was developed in two patients (5.4%) while radial nerve injury was observed in two patients (5.4%).
In final control visit, mean range of motion for elbow was 105.1°. No extension limitation was detected in 12 patients (32.4%). There was 20° of extension limitation in 15 patients (43.2%), 30° of extension limitation in 8 patients (21.6%), and 40° of extension limitation in 1 patient (2.7%). No flexion limitation was detected in 17 patients (45.9%). There was 20° of flexion limitation in 15 patients (40.5%), 30° of flexion limitation in 4 patients (10.8%), and 40° of flexion limitation in 1 patient (2.7%). The outcome was excellent in 22 patients (59.5%), good in 7 patients (18.9%), and moderate in 8 patients (22.6%) according to MAYO Elbow performance scoring system (Figure 5).
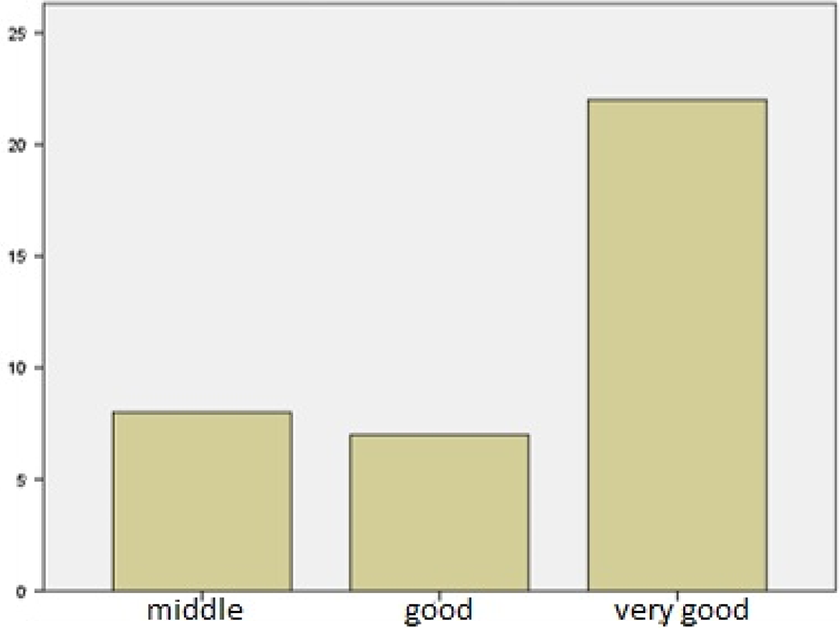
MAYO Elbow performance scores.
Nonunion was observed in 1 (2.7%) of 37 distal humerus fractures while union was achieved in 36 patients (97.3%). Nonunion in olecranon osteotomy was observed in one patient (2.7%). Following surgery, radial nerve injury was observed in two patients (5.4%). Of these, radial nerve was recovered after 3 months in one patient (2.7%) while tendon transfer was performed in the other patient as no recovery was achieved in radial nerve at year 1.
Discussion
It depends on success of articular restoration and fixation stability to achieve effective outcome in the surgical treatment of intra-articular fractures of distal humerus. A clear, perioperative articular visualization is of importance for success of articular restoration. Thus, transolecranon approach is the most frequently used technique today.
In our clinic, transolecranon approach was used in all patients with intra-articular fracture of distal humerus. The major advantages of this approach include better visualization of elbow joint, allowing surgeon to access fragments and facilitation of articular restoration. In a cadaver study, rate for visualization of articular surface was reported as 35% by triceps splitting, 46% by triceps-reflecting anconeus pedicle approach, and 57% by transolecranon approach.
In transolecranon approach, another advantage is sparing triceps muscle, resulting in lack of weakness in triceps muscle; thus, no triceps rupture during physical therapy process after surgery. This allows active or assisted-active movements immediately after surgery. No weakness or rupture of triceps muscle was seen in our study population. Active or assisted-active movements could be initiated earlier after achieving stable fixation in our patients.
Transolecranon approach is also associated with some disadvantages including implant-related pain due to materials used for olecranon re-fixation, skin irritation, and superficial infections. Removal of implant after union is usually sufficient for management of these complications. In our study, implant removal was warranted in 9 (24.8%) of 37 intra-articular fracture of distal humerus treated with transolecranon approach. The implant was removed due to superficial infection in two patients (5.4%) and implant-related pain in seven patients (19.4%). Although implant removal seems as a complication, it could be omitted due to excellent articular control and facilitated articular restoration. Without achieving control on fracture, surgical interventions targeting not to remove implant can result in non-stable elbow with poor articular restoration. No additional intervention could be required if osteotomy and fixation are performed in accordance to principles of technique used. In transolecranon approach, several osteotomy techniques including transverse osteotomy, Müller osteotomy, MacAusland osteotomy or Chevron osteotomy are used. Among these, Chevron osteotomy using inverse-T pattern is the most commonly used technique, which is also the choice of osteotomy in our clinic. It has some advantages including greater contact area for spongious bone, enhanced intrinsic stability, and readily reduction. Nonunion, malunion, or delayed union may be seen in olecranon when an additional fracture is formed. In the literature, union problems were linked to transverse osteotomy. Sane et al. performed olecranon fixation in 14 patients who underwent transverse osteotomy by using tension band and K-wire. The authors reported malunion in nine patients (64%). 8 -10 The higher malunion rate is associated to more challenging anatomical reduction and lesser intrinsic stability in transverse osteotomy when compared to Chevron osteotomy. In our study, nonunion was observed in only one patient (2.7%) who underwent olecranon re-fixation by using cancellous screw. We think that the nonunion in this patient was due to insufficient stability by cancellous screw rather than osteotomy technique.
Müller osteotomy allows more stable fixation than transverse osteotomy as it also provides wide contact area of spongious bone. However, Müller osteotomy does not allow sufficient visualization when compared to Chevron osteotomy. 11 –17 Thus, in our clinic, we preferred Chevron osteotomy given high nonunion rates in transverse osteotomy and insufficient visualization in Müller osteotomy. In our study, fixation was achieved by using tension band plus K-wire in 22 (59.5), plate in 4 (10.8%), cancellous screw in 11 (29.7%) of 37 elbows. Of 11 patients who underwent fixation with cancellous screw, tension band was combined with cancellous screw in 4 patients (10.8%) while cancellous screw alone was used in 7 patients (18.9%).
The implant removal rate due to implant-related pain is rather high, reaching up to 20–70%. 18,19 The implant was removed in 4 (18%) of 22 patients who underwent tension band plus K-wire fixation, in 3 (75%) 4 of patients who underwent plate fixation, and in 2 (18%) of 11 patients who underwent screw fixation 4–9 months after surgery. It was found that the need for implant removal was 2.6 folds lower in K-wire plus tension band fixation when compared to olecranon plate fixation, indicating significant difference (p = 0.042). We also found that the need for implant removal was 2.6 folds lower in plate fixation when compared to screw fixation but the difference did not reach statistical significance (p = 0.062). We think that such undesired conditions are associated to incorrect or incomplete application of olecranon fixation technique. We believed that skin incision moving around top of olecranon without crossing will prevent skin irritation after surgery. In fixation using K-wire plus tension band, two K-wires are bended and cleaved before final insertion. External tips are rotated toward olecranon. Tension band is passed from posterior aspect of K-wires and tension is achieved by pulling and wrapping. One must care attention to leave stump of tension band in a manner that does not cause skin irritation. Tension band is removed after stretching. We believe that such fixation with K-wire plus tension band will cause less skin irritation. Local flaps can be considered as an alternative in cases with extensive soft tissue and skin damage associated with problems in skin closure. In addition, we observed that lean patients are more susceptible to skin irritation in our clinical practice. We think that this is associated to lesser subcutaneous fat tissue. Further studies may be helpful in this issue.
There are a few biomechanics study on stability of olecranon fixation techniques. 20,21 Hutchinson et al. developed four different models including transverse osteotomy plus tension band plus intramedullary K-wire, tension band plus bicortical K-wire, tension band plus cancellous screw, and cancellous screw alone. The authors assessed mean gap in osteotomy site, showing that tension band plus cancellous screw fixation was more stable. 11 In a similar study, Wagener et al. showed that re-fixation with cancellous screw became more stable when combined with tension band. In the re-fixation using cancellous screw alone, forces ≥350 N can cause rotation or translation in proximal segment. 20 However, there is no study investigating forces influencing on elbow in daily life. In our study, nonunion in olecranon osteotomy was seen in only 1 (2.7%) of 37 elbows treated with transolecranon approach. In this patient, cancellous screw alone was used for re-fixation. Although it could not be supported by statistical data, we think that re-fixation stability is insufficient than other techniques when cancellous screw was used alone. If cancellous screw will be used for fixation, tension band use may improve stability.
Either K-wire or cancellous screw supported by tension band can be preferred in transolecranon approach. It should be suggested that cancellous screw application is easier than K-wire. Either cancellous screw or K-wire can be used by combining tension band depending on surgeon’s experience and available materials.
We initiated active and assisted-active movements immediately after achieving stable fixation. Passive movements should be avoided as they cause heterotopic ossification. 22,23 We failed to initiate physical therapy in patients requiring intensive care. Prophylactic indomethacin was used to prevent heterotopic ossification, particularly in patients with head injury. No heterotopic ossification was observed in our patients.
Conclusions
In the treatment of intra-articular fractures of distal humerus, primary aim is to achieve stable, painless elbow with complete or near-complete range of motion. Transolecranon approach provides better visualization to surgeon when compared to other techniques. In particular, transolecranon approach should be preferred in comminuted, intra-articular fractures.
In transolecranon approach, inverse-T Chevron osteotomy should be preferred due to better visualization of joint, greater intrinsic stability, and low nonunion rates. In olecranon re-fixation, either K-wire or cancellous screw supported by tension band can be used. It should be suggested that cancellous screw application is easier than K-wire. Either cancellous screw or K-wire can be used by combining tension band depending on surgeon’s experience and available materials. Plate fixation is not recommended as it more commonly leads to implant removal due to implant-related pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.