
Abstract
Objective:
To evaluate the activity of wrist extensor muscle, correlating with wrist motion during gripping after flexor tendon repair.
Design:
Cross-sectional clinical measurement study.
Setting:
Laboratory for biomechanics and rehabilitation.
Subjects:
A total of 11 patients submitted to rehabilitation by early passive motion of the fingers with wrist flexion position were evaluated after 8 weeks of fingers flexor tendon repair and 11 healthy volunteers, all ranging from 20 to 37 years of age.
Intervention:
Volunteers performed an isometric standardized gripping task.
Main measures:
We used electrogoniometry to analyze wrist range of motion and surface electromyography, considering 100% maximum voluntary contraction to represent the amplitude of electromyographic activity of the extensor carpi radialis and flexor digitorum superficialis.
Results:
Patients with flexor tendon repair showed co-activation deficit between wrist extensor (extensor carpi radialis) and flexor finger muscles (flexor digitorum superficialis) during gripping in the intermediate phase of rehabilitation, despite some recovering mobility for wrist extension (p ≤ 0.05). A moderate correlation between range of motion and extensor carpi radialis was present only for injured group (r = 0.32). Total active motion score, which represents finger active excursion, was regular or poor in 65% of cases, all with nerve repair associated.
Conclusion:
Wrist extensors have an important synergist role at handgrip, although some imbalance can be present after flexor tendon repair. These preliminary findings suggest that emphasis could be directed to add synergistic wrist motion in rehabilitation protocols after flexor tendon repair. Future studies with early active rehabilitation are necessary.
Introduction
Restoration of function after traumatic injuries to the flexor tendons of the hand continues to be one of the greatest challenges in surgery and rehabilitation.1,2 In recent years, important advances in the understanding of the anatomy of tendons, biomechanics, nutrition, techniques of repair and formation of adhesions have led to improvements in postsurgical results. Despite these advances, functional deficit continues to be a concern for any team dealing with surgery and therapy of the hand.3,4 Loss of grip force has been frequently reported after tendon repair,5–7 related to a reduction in fingers flexion due to peritendinous adhesions, tendinous gap and ruptures that impair the sliding or tensile force of the tendon. 8
Grip force is not produced just by the action of the finger flexor muscles but also by the stabilization action of the wrist extensor muscles, which act simultaneously, demonstrating physiological muscular synergism. 9 Co-activation between wrist extensor muscles and finger flexor muscles has been reported by De Serres and Milner, 10 as a control strategy to increase joint stability in the hand and minimize deviations from the desired position during gripping.
Several protocols for rehabilitation after flexor tendon repair use early passive- or active-controlled mobilization combined with the use of orthosis to maintain the wrist and the metacarpophalangeal joints in flexion to reduce tension on the repaired tendon. 2 Many studies have observed changes in muscular activation patterns influenced by different hand positions.9,11–16 However, there is still no consensus on the ideal angle of wrist extension for the best grip strength performance. Co-activation between the wrist extensor and the flexor finger muscles has been studied in some pathologies of the upper limb.17,18 However, no study has evaluated this co-activation between these muscles after flexor tendon traumatic injury and repair.
The purpose of this study was to compare the muscular activation pattern between the extensor carpi radialis (ECR) and flexor digitorum superficialis (FDS) muscles and to correlate this activation with the wrist range of motion (ROM) during a gripping task. Values were compared between healthy individuals and individuals in the intermediate phase of rehabilitation after flexor tendon repair. Our hypothesis is that individuals in rehabilitation process after surgical repair of flexor tendons have an altered co-activation pattern of wrist stabilizing muscles, and therefore present difficulties positioning this joint correctly in order to perform hand grasping tasks.
Methods
Participants
From a convenience sample, 11 individuals (7 men and 4 women), 10 right-handed and 1 left-handed, with an average age of 26.27 ± 11.10 years and body mass index (BMI) of 22.25 ± 2.3 participated in the injured group. The participants were on average at 8.9 ± 0.7 weeks post primary repair of all the injured structures in Verdan zone V at wrist level, including tendons of the extrinsic muscles (flexor carpi ulnaris, flexor carpi radialis, flexor pollicis longus, flexor digitorum profundus, FDS and palmar longus, radial artery and ulnar and median nerves). All underwent modified Duran early passive motion rehabilitation program, consisting of passive mobilization with isolated and associated interphalangeal flexion exercises, with wrist protected in flexion position. 2 None of subjects had any associated fracture in the upper limb.
A total of 11 right-handed individuals (7 men and 4 women), with an average age of 22.54 ± 2.06 years and BMI of 22 ± 1.8, participated in the control group, matched by age and gender. None of the subjects complained of any pain or orthopedic and/or neurological disorder of the upper limbs. All the participants signed a consent form prior to evaluation, and an Institutional Ethics Committee approved the study.
Surface electromyography activity
Surface electromyography (SEMG) muscle activity was recorded by Miotool 400 System™, which has an analog-to-digital (A/D) converter of 14 bits of resolution, a data acquisition board of 2000 Hz and common

Subject’s position during the procedure.
Wrist and fingers ROM
The wrist ROM was measured using a Miotec™ electrogoniometer. The axis was positioned at the ulnar styloid process, and the arms were aligned at the lateral edge of the hand and forearm. The total active motion (TAM) method proposed by the American Society for Surgery of the Hand 20 was used to evaluate the ROM of the active fingers.
Procedure
For gripping, the subjects were positioned in standardized pattern21,22 and the measurements were performed using a hand dynamometer (Jamar Inc. Jackson, MI™) in position 2. The patient was asked to produce three maximum voluntary contractions during sustained grip with the injured hand for the injured group and with the dominant hand for the control healthy group. Each grip lasted for a period of 6 s, with 2 min of rest between each execution. The wrist could move freely during the task.
Data analysis
SEMG and electrogoniometry data were processed using Miograph™ software. Root mean square (RMS) values were normalized by maximal voluntary electrical activation determined separately through three trials. Wilcoxon test was used for comparison of the variables ECR, FDS and wrist ROM between the respective groups, and Pearson coefficient was used for correlation analysis. 23
The average of grip dynamometry and the TAM score were calculated only for the injured group to obtain functional descriptive data. The values were compared with pre-established parameters in the literature.20,24
Results
There was predominance at injury in the right side, and all patients had at least one associated nerve lesion and repair. No excellent TAM values were found. Active flexion and extension ROM were present, although with weak grip strength (Table 1).
TAM, ROM in degrees and grip strength in kilogram-force (mean) of the injured group after 8 weeks postoperation.

TAM: total active motion; ROM: range of motion.
Reference values for normal Brazilian population, dominant and nondominant side, respectively: men (44.2 and 40.5 kgf) and women (31.6 and 28.4 kgf). 24
SEMG analysis of ECR and FDS muscles showed significantly lower values for injured group (p ≤ 0.05) (Figure 2 and Table 2). The average proportion of co-activation between the FDS and ECR muscles was 1: 0.87 + 0.17 for the control group and 1: 0.56 + 0.23 for the injured group (p = 0.003). Mean extension wrist ROM during gripping for injured group was −1.37° ± 8.74° and for control group was 17.13° ± 9.18° (Figure 3). There was a slight linear tendency considered to be a moderate correlation (r = 0.32) between the ECR and wrist ROM when injured group was analyzed separately. When the groups were analyzed together, the correlation of the ECR and FDS with wrist ROM was higher (r = 0.57). However, due to the heterogeneity between the group members, no linear tendency was observed in the graphs (Figure 4).
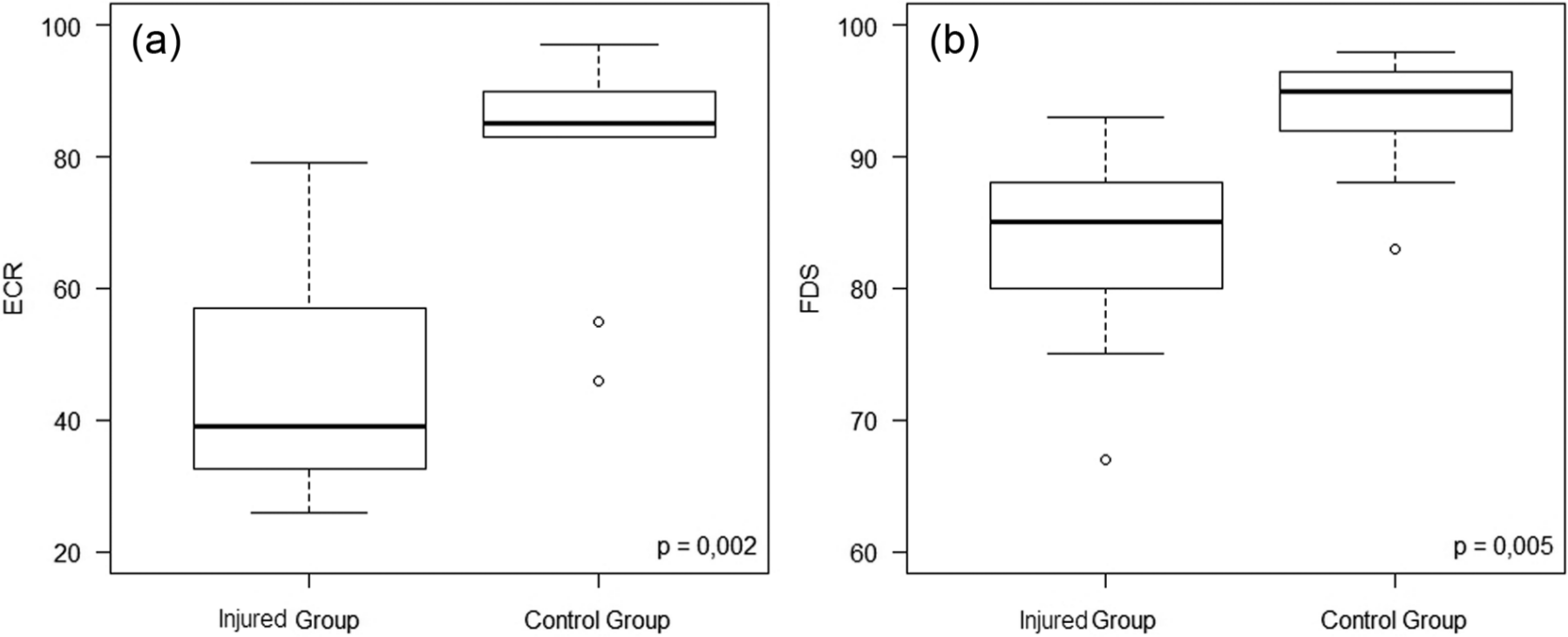
SEMG activity during gripping: (a) ECR muscle by group and (b) FDS muscle by group.
Mean values for the SEMG for the groups during the grip task.

SEMG: surface electromyography; ECR: extensor carpi radialis; FDS: flexor digitorum superficialis.

Wrist extension ROM during gripping by group.

Correlation between wrist extension ROM and the electromyographic activity by group of (a) the ECR muscle and (b) the FDS muscle during gripping.
Discussion
This study evaluated the wrist extensor muscles by SEMG in patients after flexor tendon repair, as well as the wrist angle during gripping. There was an important reduction in the electromyographic activity of the ECR and FDS muscles in the injured group compared to the control group, as well a significant decrease of the co-activation between these muscles. Concomitantly, during gripping, the wrist joint was in a flexion position, while for the control group, this angle was significantly more to extension position. However, our results showed that despite some recovering mobility for the extension (25.83° ± 13.81° of wrist extension after 8.9 ± 0.7 weeks postoperation), the individuals in the injured group did not manage to sustain this angle during the task (Figure 5).
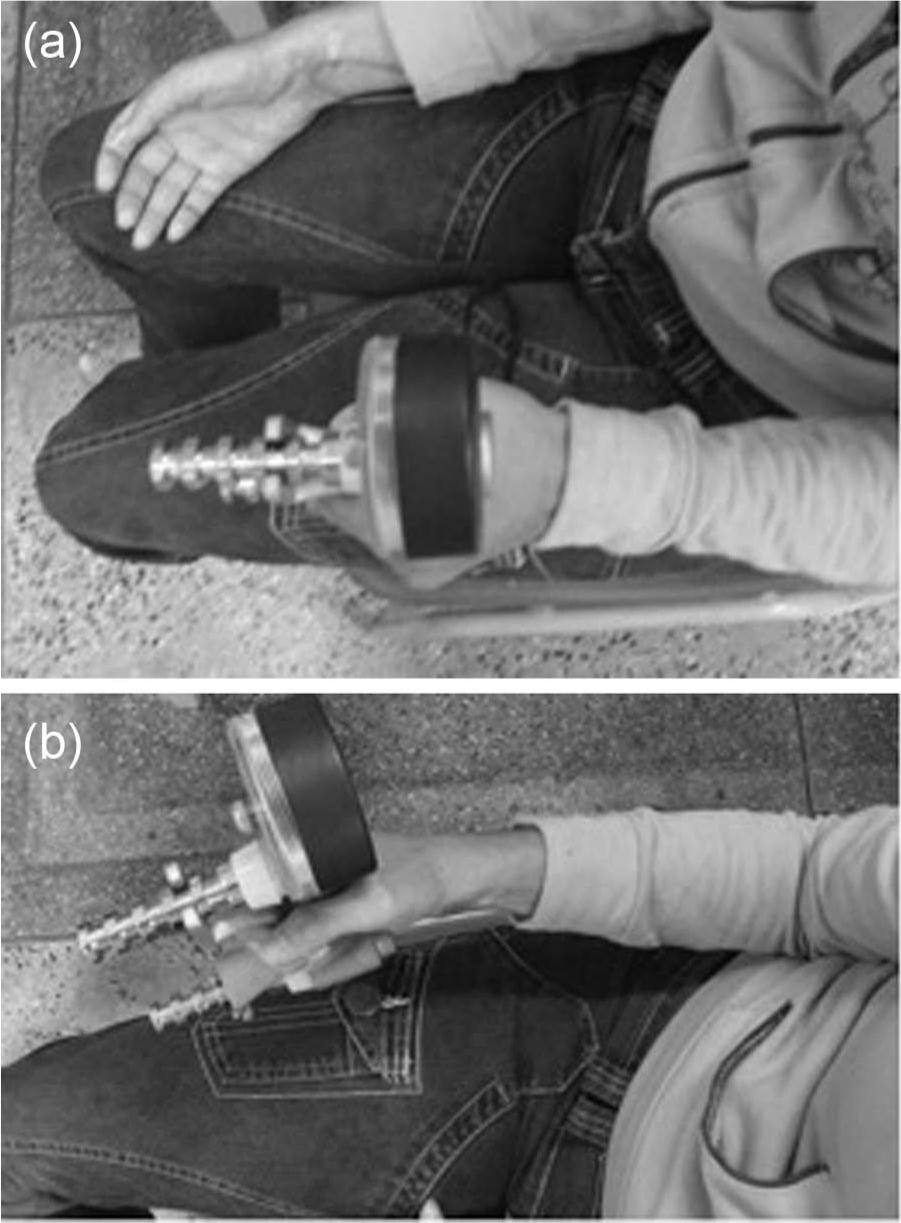
Visual comparison of wrist position during the gripping task between (a) injured and (b) noninjured hand of a patient after 8 weeks of flexor tendon repair.
The correlation was observed between ECR electromyographic activity and wrist ROM in the injured group. However, it was not observed in the control group. This supports the idea that extension of the wrist joint is necessary for better performance of the stabilizing muscles, but the optimal length–tension relationship of extensor muscle does not match a relevant wrist extension. The control group showed similar rate of muscle activation between FDS and ECR (1:0.87). In the injured group, this activation was much lower (1:0.56). This unusual predominance of one of the pairs of synergistic muscles during the extension movement may impair the proper muscular balance and joint alignment. 17
The grip strength of the sample showed values considerably lower than normal reference population, 24 even at an intermediate rehabilitation phase, just before starting strengthening training. There is a consensus in the literature that greater grip strength is achieved with the wrist joint in extension;9,11–15,25 however, there is a variation of the ideal angle between studies. Shimose et al. 9 have also showed the importance of study of the wrist extensor muscles by SEMG analysis in a hand strengthening training program.
Savage 26 showed that when the wrist is in an extension position, less force is required from the finger flexors muscles to overcome the passive tension of the extensor tendons of the hand (passive insufficiency). With the hand in neutral position, the resistance of the flexor tendons increases; however, it is still less than that achieved with the hand at 45° flexion. This supports the tendency to immobilize the wrist joint in a neutral or slightly extended position during the initial healing period after flexor tendon repairs.2,25 In the present study all patients used postoperative flexion wrist orthoses.
Zhao et al.’s 27 study was based on a comparison of the sliding of sutured flexor tendons in canine paws between the synergistic protocol (passive extension of the wrist with flexion of the fingers and vice versa) and the conventional passive mobilization protocol with the wrist joint kept in flexion by an orthosis. The results showed that the synergistic protocol produced greater sliding and excursion of the tendons at 1 week postoperation and thus reduced the risk of tendinous blockage within the sheath. Another study by the same group showed that this protocol yielded a lower frequency of tendinous adherence compared to the conventional protocol. There was a greater tendinous gap in the synergistic protocol group, but this did not lead to an increase in ruptures of the tendon compared to the prevalence in the conventional passive mobilization group. It is important to emphasize that the tendons in these studies were partially lacerated (80%). 28
Diminished TAM values have been cited as one of the factors related to reduced grip force 8 and function. 29 In this study, 65% of the fingers were classified as regular or poor in the injured group, at the time of evaluation, between 8 and 10 weeks postoperation. Bal et al. 6 analyzed subjects with flexor tendons injuries in zone V after 55 weeks postoperation, using the modified Kleinert protocol. The TAM score at that group showed 83% of the excellent and good results, however, still with a significant deficit in grip strength.
Sensory deficits and function impairment of hand intrinsic muscles caused by nerve damage, commonly associated with flexor tendons lesions in zone V, and some degree of adhesion are also some of the factors that may cause decrease in grip strength. 30 In this study, all subjects had nerve damage. We believe that initial immobilization keeping the wrist joint in a flexion postion, as prescript at the protocol used in this study, may be one of the factors aggravating this pattern of alteration of the co-activation expected between wrist extensor and finger flexor muscles during gripping in the course of the rehabilitation process, inhibiting the activation of the wrist extensor.
Groth 31 proposed an interesting model of progressive exercises after flexor tendon repair. These exercises are represented as a pyramid, with the base indicating the lowest level of force through the suture as well as exercises that are performed more frequently. At this level, there are exercises that combine movement with synergistic wrist extension and finger flexion, and according to this proposal, they should be introduced from the first week after surgery. Our results corroborate with other researchers, 32 suggesting that the increased activity of wrist extensors should be emphasized early in the rehabilitation process and may thus contribute to functional improvement performance of the grip without jeopardizing the sutured tendon. In addition to knowledge regarding anatomy and physiopathology of flexor tendons repair, the choice of early rehabilitation protocols depends on many factors, such as the extent of the injury, associated injuries, surgery, age and patient motivation, among others.2–4,32 Muscle synergism imbalance after flexor tendon repair seems to be thus related to a deficit at extension wrist joint stabilization during pretension, which is critical for proper grip strength performance.
Limitations of our study
There is no previous study related to test the wrist electrogoniometer reliability. We used dominant hands of healthy volunteers as a control group with the aim to standardize the measure because some patients had injured the dominant one. In addition, there is a theory describing that some muscle changes could occur during training and detraining on the contralateral limb, as a contralateral effect of unilateral training. 33 Nevertheless, prospective studies comparing injured to the healthy side of the same patient can bring different results.
We have to also consider that the analysis of a single pair of extrinsic muscles, including wrist extensor and finger flexor, cannot by itself describe a functional grip. EMG analysis with more pairs of extensor and flexor muscles is mandatory, taking into consideration the cross talk issues related to forearm electrodes placement. 34
Early active rehabilitative protocols in clinical trials emphasizing finger flexion exercises associated with wrist extension, with larger sample size, are necessary to verify the outcome of all wrist extensor muscle activation during grip task in a synergistic pattern after flexor tendon repair in longer follow-ups.
Clinical messages
Wrist extensor muscles are essential to stabilize pretension task.
Early flexor tendon repair protocols could include exercises that combine movement of synergistic wrist extension and finger flexion, aiming to improve muscle activation and tendon gliding without jeopardizing the sutured tendon.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest related to this manuscript.
Funding
This work was supported by Sao Paulo Research Foundation (FAPESP- Brazil) (grant number 2008/00881-9).