
Abstract
Introduction:
Reduction in neuroforaminal height (FH) may diminish the indirect decompression benefit that lateral access surgery (LAS) provides. However, the relationship between postoperative FH reduction in LAS and health-related quality-of-life (HRQoL) outcomes remains unclear.
Objectives:
To determine whether FH reduction affects HRQoL outcomes at 2-year follow-up.
Methods:
A retrospective review of 45 patients who underwent LAS for degenerative lumbar spine conditions was performed. The cohort was divided into two groups: maintenance (A) and reduction (B) in FH. Outcome measures included numerical pain rating scale (NPRS back and leg pain), Oswestry Disability Index (ODI), Short Form 36 Health Survey (SF-36), North American Spine Society (NASS) score for neurogenic symptoms (NS), patient satisfaction, and expectation fulfilment for surgery. Mean disc height (DH), FH, and fusion were evaluated on plain radiographs. Radiological fusion was assessed with the Bridwell fusion classification. Unpaired student’s t-test was used to compare between groups and one-way ANOVA with Bonferroni post hoc correction was used to determine differences between time intervals within each group.
Results:
The average pre-op mean FH was 16.9 ± 3.5 mm. Group A had 25 patients showing postoperative maintenance of FH (19.4 ± 3.3 mm to 20.2 ± 3.2 mm; 4% increase) at 2-year postsurgery while group B had 20 patients showing decrease in FH (21.1 ± 3.3 mm to 18.7 ± 3.5 mm; 11% decrease). Group A mean DH improved from 7.0 ± 2.0 mm to 10.3 ± 1.6 mm (47% increase). Group B mean DH improved from 6.8 ± 2.3 mm to 11.0 ± 3.0 mm (62% increase). There were no significant differences in NPRS, ODI, NASS, SF-36, and SF-36 MCS/PCS between groups at 2 years (p > 0.05); 92% of group A and 85% of group B patients reported good satisfaction and fulfilment of expectations (p > 0.05).
Conclusion:
Despite an initial increase in FH after LAS surgery, 45% of patients had FH reduction at 2 years. However, FH reduction up to 11% did not affect short-term HRQoL outcomes.
Keywords
Introduction
Minimally invasive lateral access surgery (LAS), also known as lateral lumbar interbody fusion (LLIF), has been shown to be effective in the treatment of degenerative spinal conditions with multiple studies reporting excellent improvement in clinical outcomes. 1 –4 Recent studies have reported greater improvements in back and leg pain, as well as reduced peri-operative blood loss when comparing LLIF with minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF). 4,5 These advantages are postulated to be secondary to the superior correction of lumbar scoliosis and restoration of foramina height in LLIF surgery. 6 –8 LLIF has also been shown to confer an 80% increase in postoperative neuroforaminal height (FH). 9
Interbody cage subsidence is a potential complication of LLIF, which may compromise the indirect decompression benefit from disc and FH restoration. 7,8,10,11 Cage subsidence may occur in up to 14.3% of LLIF cases and may affect maintenance of FH postoperatively. 7,8,10,12 In theory, cage subsidence with concomitant FH reduction may compress exiting nerve roots and negatively impact patient outcomes.
However, Marchi et al. reported that radiographic cage subsidence does not impact patient outcomes in the short term (12 months). 13 Some studies have also reported good patient reported outcome measures (PROMs) despite FH reduction at 12 months. 7,8,10 However, the relationship between PROMs/health-related quality-of-life (HRQoL) and postoperative FH maintenance in LLIF remains unclear. The aim of this study is to determine whether changes in FH affect patient outcomes and QoL at 2-year follow-up. We hypothesize that postoperative FH reduction at 2 years may adversely affect outcomes.
Methods
Study design
Local institutional review board (IRB) waiver was obtained for this study, after the IRB committee decision that the study posed minimal risks to study subjects. A retrospective review of patient data at a single institution of all the LLIF surgeries performed by a single fellowship-trained spine surgeon was carried out. All consecutive LLIF surgeries performed from August 2010 to November 2014 were included in the study. The indication for LLIF was lumbar degenerative disc disease which did not respond to nonsurgical management. All patients had back pain and lower limb neurological symptoms such as radiculopathy, paresthesia, and numbness. These symptoms correlated to the level of foramina stenosis and all the patients were seen by a senior consultant spine surgeon. The inclusion criteria for this study included lumbar spinal stenosis secondary to degenerative disc disease and grade 1 or 2 spondylolisthesis, symptomatic clinical features of lumbar stenosis or radiculopathy, radiological evidence of lumbar stenosis on magnetic resonance imaging (MRI), and failure of a trial of conservative therapy of a minimum of 6 months. Exclusion criteria included patients with acute spinal trauma, spinal infections, spinal tumors/metastases, and previous spinal instrumentation to affected levels.
All patients (n = 45) were followed up for a minimum duration of 2 years postoperatively. Patients underwent either LLIF (n = 35) or hybrid LLIF (LLIF in combination with MIS-TLIF, n = 10). The patients who underwent hybrid LLIF had L5/S1 pathology which was addressed by a single-level, posterior MIS-TLIF procedure. LLIF was performed for all caudal levels above L5/S1 for our patients and this study included both single-level and multilevel LLIF procedures.
Surgical procedure
For the LLIF procedure, patients were placed in a lateral position with the convex side of the lumbar curvature facing superiorly. A lateral transpsoas approach was used to access the desired disc space. NuVasive XLIF® system instruments were used for all cases. Intra-operative radiography was used to guide instruments to the correct spinal level. Discectomy, trial of LLIF interbody cages, followed by insertion of the actual interbody cage implants (packed with autograft and/or allograft) was performed. Radiographs were obtained to confirm optimal position of the cages followed by wound closure. For patients undergoing hybrid LLIF, they would be turned prone and the surgeon would continue with the MIS-TLIF procedure. Percutaneous posterior instrumentation with pedicle screws and rods was performed for all levels of LLIF and MIS-TLIF. Hemostasis and wound irrigation are performed prior to wound closure. Postoperative rehabilitation was in accordance with our institution’s standardized lumbar spine surgery integrated care pathway.
Clinical outcome assessment using patient reported and HRQoL outcome measures
Preoperative patient demographics including age, gender, and body mass index (BMI) were recorded. Patients were reviewed preoperatively and postoperatively at 6 and 24 months. During each visit, patients were assessed with validated spine-specific scores such as the Numerical Pain Rating Scale (NPRS) for back and leg pain, Oswestry Disability Index (ODI), North American Spine Society (NASS) lumbar spine outcome score for neurogenic symptoms (NS), patient-rating for overall result of surgery, and expectations met for surgery.
The NPRS was used to specifically score back and leg pain in lumbar spine disease and has been shown to be highly correlated with the Visual Analogue Scale (VAS) with high test–retest reliability in both literate and illiterate patients and is easily comprehended. 14,15 The ODI addresses a broader concept of disability that is not directly related to pain intensity. 16 In addition, its sensitivity as a measure of treatment success has been validated. 17 The NASS outcome scoring for NS has been proven to have high internal consistency, test–retest reliability, and good validity in distinguishing operative success from operative failure. 18
The Short-Form 36 Health Survey (SF-36) was utilized and its summative physical component summary (PCS) and mental component summary (MCS) were calculated. The transformed PCS and MCS scores possess the advantage of a smaller confidence interval and elimination of both floor and ceiling effects. 19 All outcome measures were collected by blinded observers.
Radiological evaluation
All patients had radiographs (anterior–posterior and lateral) of the lumbar spine preoperatively, postoperatively, and at 2 years. Disc heights (DHs), adjacent-level disc heights (ADHs), and FH were measured on lateral radiographs for all LLIF levels. Based on the levels of LLIF performed, mean values of DH, ADH, and FH were calculated for each patient. Global lumbar lordosis was also recorded for each patient. Subsidence was calculated using mean DH and classified according to the grading system proposed by Marchi et al. 13 FH was measured on the lateral radiograph from inferior pedicle wall to superior pedicle wall of the level below (Figure 1) as described by Hsieh et al. 20 DH was similarly measured, but the average of the anterior and posterior disc height was taken instead (Figure 2). Patients were divided into group A (<0.5 mm decrease in FH) and group B (>0.5 mm decrease in FH). There is likely a critical amount of FH decrease before outcomes are affected; however, there is currently no known literature describing that to our knowledge, and hence the FH of 0.5 mm was chosen to dichotomize the group of patients. Fusion rates based on the grading system by Bridwell et al. were assessed at 2 years. 21 All measurements were done by two independent investigators not involved in the surgery. Figures 3 to 5 represent the preoperative, postoperative, and 2 year postoperative imaging for an XLIF patient.

Example of measurement of foraminal height on lateral lumbar spine radiograph.

Example of measurement of anterior and posterior interbody disc height.

Example of patient preoperative radiograph.

Example of patient postoperative radiograph.

Example of patient 2-year postoperative radiograph.
Statistical analysis
A power analysis was conducted with type-I error set at 0.05 (α < 0.05) and the type-II error at 0.15 (85% power). A minimum sample size of 20 patients was required to detect a significant difference in FH between the two groups based on two-sample test of proportions and a two-sided test hypothesis. All continuous data were expressed in terms of mean and standard deviation of mean. Unpaired student’s t-test was used to compare between groups, and repeated measures ANOVA using Bonferroni post hoc correction was used to determine any differences at preoperative and postoperative time intervals within each group. Intra-observer and interobserver reliability was calculated using the interclass correlation coefficient (ICC). Statistical analysis was performed using SPSS 20.0 software (SPSS Inc, Chicago, Illinois, USA).
Results
Patient demographics are described in Table 1. All patients demonstrated significant improvements in NPRS, ODI, NASS (NS), SF-36, and SF physical component summary (PCS) scores (p < 0.05; Table 2). There was no significant improvement in SF-36 mental component summary (MCS) scores at 2 years postoperatively; 89% of patients reported good/very good/excellent satisfaction and felt that the surgery met their expectations.
Patient cohort characteristics.

BMI: body mass index.
Overall outcome scores.

VIS: Visual Analogue Scale; NASS: North American Spine Society; ODI: Oswestry Disability Index; SF-36: Short-Form 36 Health Survey; PCS: physical component summary; MCS: mental component summary.
Of the 45 patients, 25 patients (group A) did not demonstrate FH decrease (<0.5 mm) at 2 years postoperatively when compared to immediate postoperatively radiographs, whereas 20 patients (group B) demonstrated a FH decrease (>0.5 mm). Both groups demonstrated improvements in outcome measures at 2 years postoperatively (Table 4). However, there were no significant differences between groups A and B for VAS back pain, leg pain, ODI, NASS, and SF-36 (p > 0.05) at 2 years postoperatively (Table 4); 92% of group A patients felt that their expectations of surgery were met and the overall result was at least “good,” whereas 85% of group B patients felt that way. There was no significant difference in satisfaction or expectation fulfilment between groups A and B (Table 3). Mean BMI for group A was 25.3 ± 3.9 and for group B, 27.1 ± 4.2. There was no significant difference in BMI between the groups (p = 0.13).
Patient satisfaction and expectations.

Comparison of outcomes between foraminal height groups.
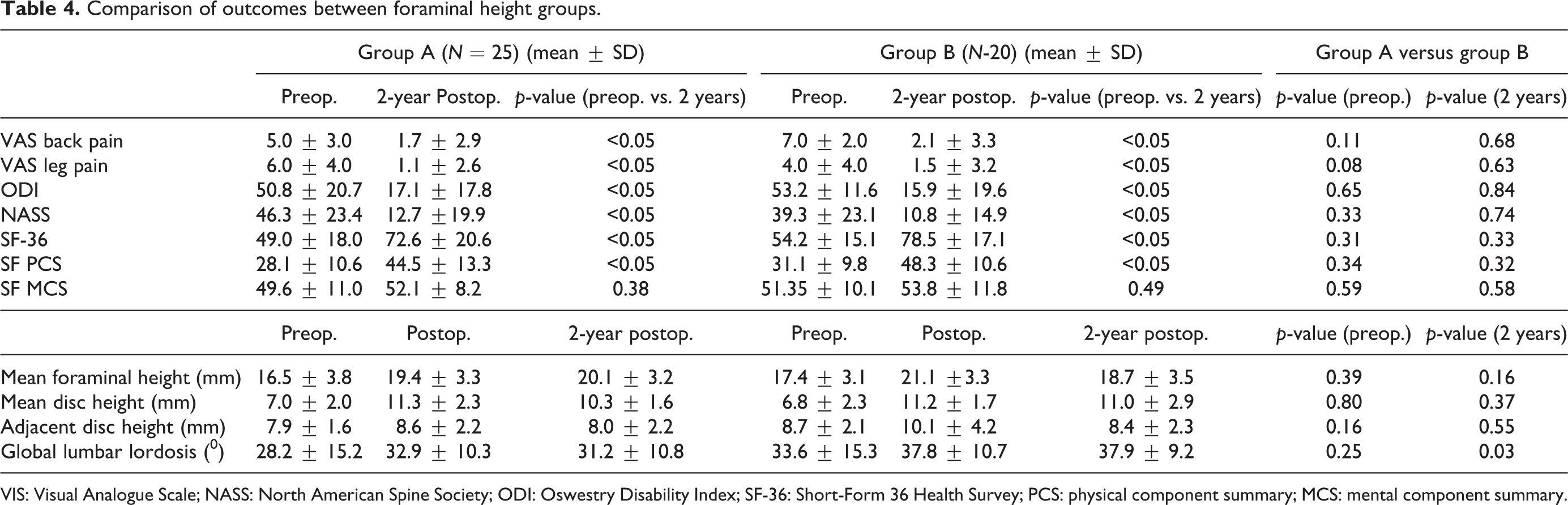
VIS: Visual Analogue Scale; NASS: North American Spine Society; ODI: Oswestry Disability Index; SF-36: Short-Form 36 Health Survey; PCS: physical component summary; MCS: mental component summary.
Mean FH, DH, and global lumbar lordosis increased immediately postoperatively in both groups A and B (Table 4). Overall, mean postoperative FH was 20.1 ± 3.4 mm, decreasing to 19.5 ± 3.4 mm at 2 years. Intra-observer reliability ICC for mean foramina height was 0.874 (95% confidence interval (CI): 0.638–0.960), mean disc height 0.913 (95% CI: 0.740–0.973), mean adjacent disc height 0.86 (95% CI:- 0.479–0.936), and lumbar lordosis 0.981 (95% CI: 0.939–00.994). Interobserver reliability ICC for mean foramina height was 0.825 (5% CI: 0.522–0.943), mean disc height 0.874 (95% CI: 0.639–0.960), mean adjacent disc height 0.806 (95% CI: 0.480–0.937), and lumbar lordosis 0.962 (95% CI: 0.880–0.988).
Subgroup analysis of single-, two-, and three-level LLIF procedures demonstrated significant improvements in functional outcome scores at 2 years (Table 5). Of all 95 levels of LLIF performed, 86% of cases had minimal or no cage subsidence (grade 0 or 1) and 14% showed higher grades of cage subsidence (grade 3 or 4) (Table 6). These patients with higher grades of subsidence still improved significantly postoperatively, demonstrating similar outcomes to patents with no cage subsidence.
Outcomes for different levels LLIF.
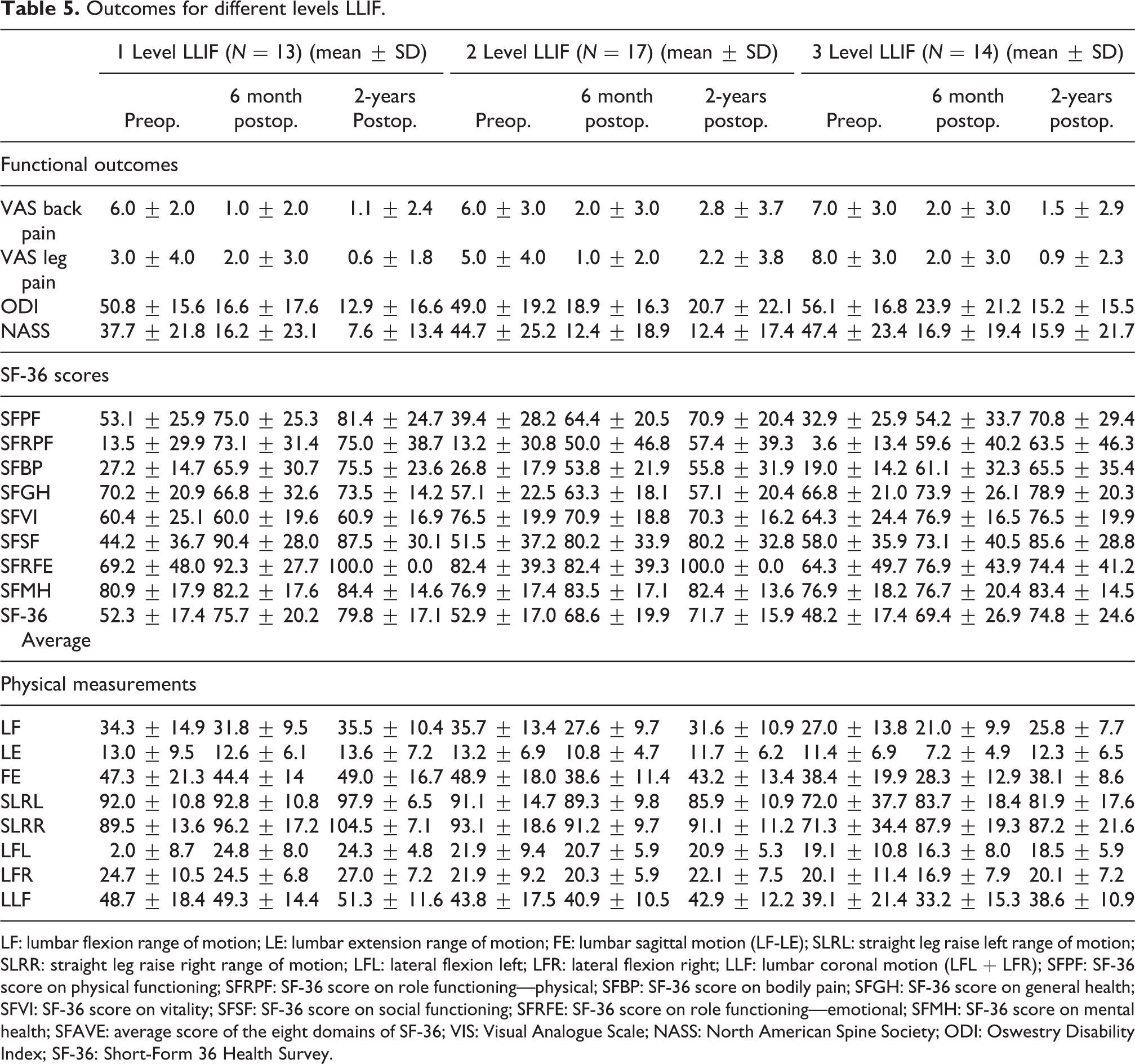
LF: lumbar flexion range of motion; LE: lumbar extension range of motion; FE: lumbar sagittal motion (LF-LE); SLRL: straight leg raise left range of motion; SLRR: straight leg raise right range of motion; LFL: lateral flexion left; LFR: lateral flexion right; LLF: lumbar coronal motion (LFL + LFR); SFPF: SF-36 score on physical functioning; SFRPF: SF-36 score on role functioning—physical; SFBP: SF-36 score on bodily pain; SFGH: SF-36 score on general health; SFVI: SF-36 score on vitality; SFSF: SF-36 score on social functioning; SFRFE: SF-36 score on role functioning—emotional; SFMH: SF-36 score on mental health; SFAVE: average score of the eight domains of SF-36; VIS: Visual Analogue Scale; NASS: North American Spine Society; ODI: Oswestry Disability Index; SF-36: Short-Form 36 Health Survey.
Rate of cage subsidence in all 95 levels of LLIF.
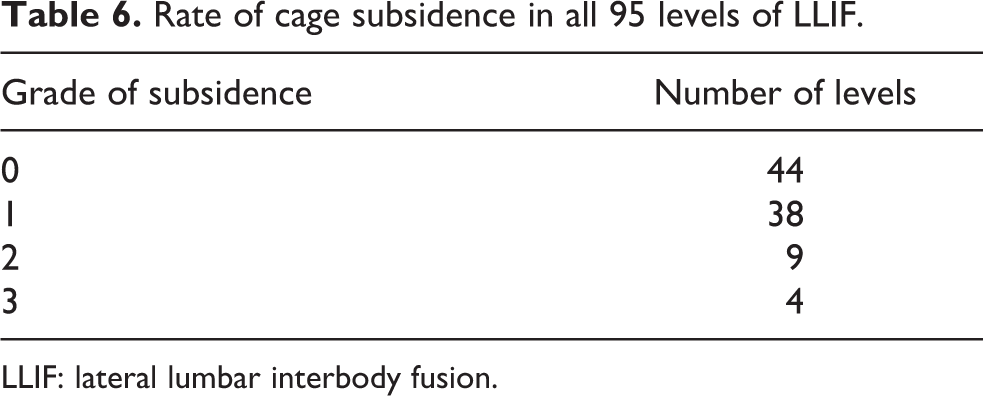
LLIF: lateral lumbar interbody fusion.
Fusion rates were shown to be high, with 97% of cases achieving Bridwell 21 grade 1 fusion; 3% achieved Bridwell grade 2 fusion out of the 95 level of LLIF fused. These were evaluated on erect lumbar lateral radiographs.
In terms of overall outcomes for our whole cohort of patients, the results were largely satisfactory. The outcome scores for the ODI, VAS back, and leg pain exceeded the minimum clinically important difference (MCID) in lumbar spine patients as described by Copay et al. 22
Postoperative complications
There was one patient who had postoperative wound infection and had to undergo wound debridement with retention of implants. Two patients had subsequent compression fractures at the level of surgery and were treated conservatively. Two patients developed adjacent segment disease at L5/S1 and underwent a MIS-TLIF procedure.
Discussion
The most important finding of this study was that a reduction in FH did not result in poorer functional outcomes in patients undergoing lateral access surgery. Failure to maintain FH improvements postoperatively may theoretically compromise the benefits of indirect decompression from LLIF. LLIF cage subsidence can potentially lead to loss of indirect compression and contribute to poorer functional outcomes. However, interestingly, it has been shown that clinical outcomes do not necessarily correlate with cage subsidence. 13 Our results concur with these findings, demonstrating that FH reduction did not adversely affect clinical outcomes or quality-of-life scores. There is a paucity of literature examining the relationship between postoperative FH maintenance in LLIF, clinical outcomes, and QoL scores. To the best of our knowledge, our study is the first to show that postoperative FH maintenance does not adversely affect outcomes at 2-year follow-up.
FH subsidence occurred in approximately 45% of our patients at short-term follow (2 years). Previous studies on LLIF have measured FH preoperatively and postoperatively with measurements up to 1 year postoperatively. Alimi et al. reported that their postoperative mean FH was 18.1 mm which decreased to 17.1 mm at last follow-up (average 11 months). Tohmeh et al. also reported similar results at 12 months postoperatively, highlighting similar degrees of FH reduction in cases without cage subsidence (10.9–9.6 mm) and in cases with cage subsidence (10.0–8.4 mm). 7,8 However, these studies did not correlate these findings with clinical outcomes. Similarly, our study demonstrated a reduction in FH (21.1 ± 3.3 mm to 18.7 ± 3.5 mm). In addition, we observed that FH subsidence did not adversely affect outcomes in our cohort.
Previous studies on LLIF have examined the relationship between cage subsidence and influence on clinical outcomes. Lang et al. demonstrated a mean subsidence of cage height of 0.34 mm between postoperative and follow-up (average 239 days) imaging. 23 They noted that cage subsidence was less when using a wider cage; however, clinical outcomes between groups showed no significant differences. Likewise, Malham et al. did a study on lateral lumbar interbody fusions showing that radiographic cages subsidence did not impact clinical outcomes. 24 They found that 10% of their cohort of 128 patients showed delayed cage subsidence depth of subsidence ranging from 1.6 mm to 6.0 mm. Our results are comparable with immediate postoperative average disc heights of 11.3 mm and decreasing at 2 years, to an average of 10.6 mm.
This study has to be interpreted in light of its potential limitations. Firstly, there is a small number of patients in our study. However, one of its strengths was that all surgeries were performed by a single experienced senior spine surgeon (fellowship trained) at a single center. Secondly, a lumbar spine CT scan would have been more accurate for the assessment of FH and fusion. A study by Isaacs et al. 6 reported that overlap of pedicles on the lateral view of a radiograph may lead to difficulties in interpretation of the FH. A CT scan would also allow calculation of the foramina area. The authors realize that a CT scan would have been more accurate and ideal for assessment of fusion; however, this would lead to extra costs and increased radiation risks to our patients which is unnecessary. Khajavi et al. did a study on anterior lumbar interbody fusion and measured their radiological outcomes using only plain radiographs. They acknowledged that although fusion outcomes would be better assessed on CT scans, doing routine follow-up CT scans without a strong clinical indication was a deviation from their local practice. 25 Similarly, for our purposes, using a lumbar spine radiograph was sufficient to assess foramina heights.
Conclusion
This study provides valuable information regarding the relationship between FH maintenance and clinical outcomes. Postoperative maintenance of FH was demonstrated in 55% of patients at 2-years and reduction in FH was not associated with poorer functional outcomes. LLIF patients who experience FH subsidence postoperatively can still have satisfactory clinical outcomes and QoL in the short term. Future research can focus on identifying the critical foraminal height that predicts poorer outcomes in LLIF.
Footnotes
Authors’ note
Local institutional review board (IRB) waiver was obtained for this study.
Author contribution
Keng Meng Jeremy Goh and Ming Han Lincoln Liow contributed equally as first authors of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors declare that they have no conflict of interest except Author Guo Chang Ming (paid speaker for Nuvasive).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.