
Abstract
A bizarre parosteal osteochondromatous proliferation (BPOP) is a rare, benign, osseous tumor that presents as an exophytic cortical growth consisting of bone, cartilage, and fibrous tissue. However, the identification of BPOP by preoperative imaging along with appropriate diagnosis and treatment without recurrence is challenging, particularly for BPOPs that rarely develop in certain parts of the body. Herein, we report a rare case involving a BPOP at the sesamoid bone of the hallux that was first suspected on preoperative computed tomography imaging. There has been no recurrence 3 years after surgical resection.
Introduction
A bizarre parosteal osteochondromatous proliferation (BPOP), also known as Nora’s lesion, is a rare, benign, osseous tumor that presents as an exophytic cortical growth consisting of bone, cartilage, and fibrous tissue. 1 –3 BPOPs predominantly develop in the short bones of the hands and feet, eventually presenting as a parosteal mass. 4 –6 To the best of our knowledge, only three cases of BPOP involving the sesamoid of the hallux have been reported in the literature. 7 –9 For the diagnosis to be confirmed, a BPOP must be differentiated from a benign osteochondroma, as well as from malignant tumors, such as an osteosarcoma with malignant transformation, a parosteal osteosarcoma, and a periosteal osteosarcoma. 7,10 The recurrence rate of BPOP is very high; the rate of initial recurrence is 51%, while the rate of second recurrence is 22%. 3,11 The majority of recurrences occur within 2 years of excision. 11 In this report, we describe a case of BPOP involving the sesamoid bone of the hallux that was first suspected on preoperative computed tomography (CT) imaging.
No surgical recurrence has occurred 3 years after resection.
Case report
A 46-year-old man visited our hospital with a mass on the plantar aspect of his left hallux that caused him discomfort and some pain during walking. He reported that the mass first developed 23 years ago and was slowly enlarging. Over the past 6 years, he felt increasing discomfort and some pain in the area.
Clinical examination revealed a large callus formation under the metatarsophalangeal (MTP) joint of the left hallux, which was non-tender and firm on palpation. A bone-like mass could be palpated under the callus, which measured approximately 5.0 × 4.0 cm2 (Figure 1(a)) and was adherent to the underlying bone. The patient had a full range of active and passive motion of the MTP joint, with no neurovascular symptoms and no hallux valgus deformity.

(a) Image showing the large callus formed at the level of the metatarsophalangeal joint of the left hallux and (b, c) plain radiographs of the left foot.
Plain radiographs of the left foot revealed a bony mass of the internal sesamoid bone of the hallux (Figure 1(b)). Computed tomography (CT) confirmed a calcified and ossified lesion on the medial side of the sesamoid bone, with no continuity between the mass and the medullary canal of the host sesamoid bone (Figure 2). The size of the mass on the CT image measured 4.5 × 4.2 × 2.4 cm3, but no other radiological abnormality was identified. Magnetic resonance (MR) imaging revealed a lesion with low intensity on T1-weighted and heterogeneous intensity on T2-weighted imaging (Figure 3), with no evidence of a cartilaginous cap on either T1- or T2-weighted images. The boundary between the mass and the host medial sesamoid bone was difficult to distinguish.

(a) CT and (b, c) three-dimensional CT images at the level of the MTP joint of the left hallux. CT: computed tomography; MTP: metatarsophalangeal

Axial magnetic resonance images of the left foot, which fail to show the cartilaginous cap on T1- and T2-weighted images (a to d) and present a difficult-to-distinguish boundary between the mass and host medial sesamoid.
The mass was surgically resected under spinal anesthesia. A 6-cm straight skin incision was made, with the center of the axial incision placed on the medial aspect of the MTP joint of the hallux, thus saving the abductor hallucis muscle. The surface of the lesion was covered with the fibrous tissue. The mass was resected, along with its fibrous tissue and the adjacent host medial sesamoid bone. The resected mass had irregularly shaped cartilage-like edges and measured 5.0 × 3.2 × 2.2 cm3 (Figure 4). The tendon of the medial head of the flexor hallucis brevis muscle possessed a defect caused by the mass. The tendons of the flexor hallucis longus muscle and of the lateral head of flexor hallucis brevis muscle, located over the lateral sesamoid bone of the hallux, were intact.
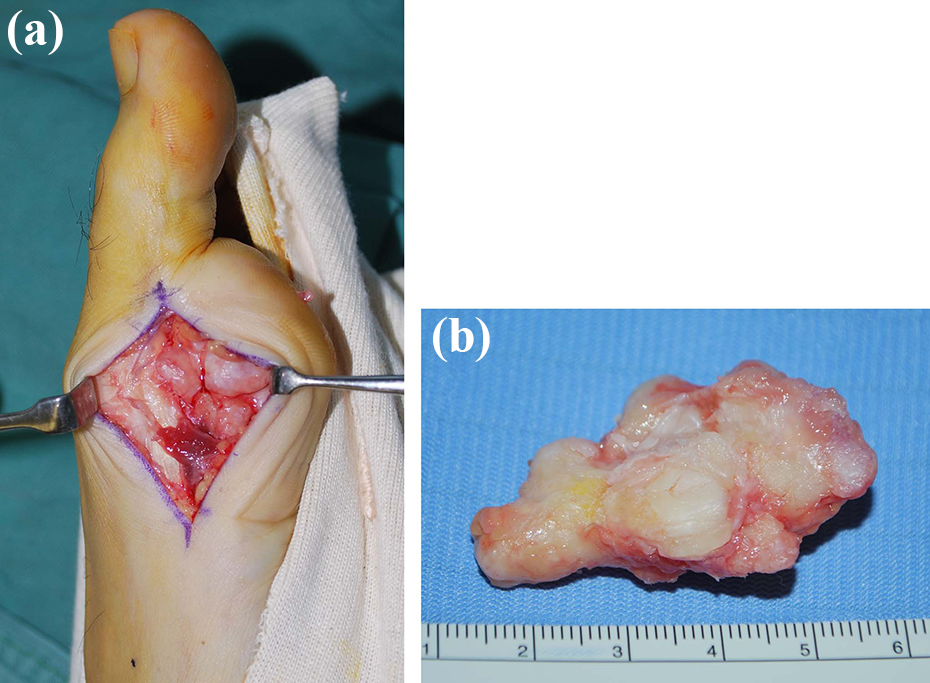
(a) Mass with irregularly shaped cartilage-like edges, measuring (b) 5.0 × 3.2 × 2.2 cm3.
Histopathological examination of the mass revealed an irregular osseous–cartilaginous interface, with slightly bizarre nuclei and intertrabecular fibroblastic proliferation. The cartilage was undergoing endochondral ossification, with new bone lined by benign, activated appearing osteoblasts (Figure 5).

Histopathological images showing (a) irregular osseous–cartilaginous interfaces and intertrabecular fibroblastic proliferation (hematoxylin and eosin staining; ×100) and (b) the basal area of cartilage composed of immature bony trabeculae with high osteoblastic activity (hematoxylin and eosin staining, ×400).
A final diagnosis of BPOP was confirmed based on these histopathological findings and the absence of continuity between the mass and the medullary canal of the host sesamoid bone on computed tomography (CT) imaging. The patient was followed up for 3 years, and no recurrence of the lesion was observed (Figure 6). The patient remains asymptomatic.

X-Ray of the affected area acquired 3 years after surgery.
Discussion
BPOP was originally reported by Nora et al. in 1983, and all 35 cases described in this first report involved the hands and feet, with occurrences in the proximal phalanges, metatarsals, or metacarpals. 3 Since then, cases of BPOP involving the skull, 12,13 long bones, 1,13 and, in rare cases, the anterior maxilla, nasal dorsum, and zygoma, 13 –15 have also been reported.
Although BPOP is usually identified in the third or fourth decade of life, the condition can occur at any age, with no sex predilection. 3,5,7 The cause of BPOP remains unknown, although in some cases, it might be associated with a bone reparative process after trauma to the periosteum, as was noted by Meneses et al. in 30% of cases reported. 11,12 However, there was no history of trauma in our current case.
Excision is the recommended treatment for symptomatic BPOP. Wide excision can be curative, but there is a likelihood of local recurrence when BPOP is treated using intralesional excision. 5,11 In addition, resection of the capsule of the lesion, and decortication of the underlying cortical bone, have been recommended as a means of reducing the rate of recurrence. 10,16 The recurrence rate of BPOP was reported to range between 27% and 55%, with inappropriate resection being associated with a higher rate of second recurrence. 3,5,7,11 –13,16,17 Furthermore, the majority of recurrences occur within 2 years of excision. 11 As we completely excised the mass in our current case, including the adjacent host medial sesamoid bone and the fibrous tissue surrounding the mass and the injured flexor hallucis brevis, there was no recurrence of the BPOP lesion. Three cases of BPOP involving the sesamoid of the hallux have been reported, 7 –9 and two cases were reported in detail. 8,9 They stated no recurrence within 15 months.
In general, osteochondroma is the most important differential diagnosis of BPOP, with other differential diagnoses including periosteal chondroma, parosteal osteosarcoma, multiple exostoses, and florid reactive periostitis ossificans. 3,6,7,10,18 In our current case, BPOP was suspected on the basis of preoperative CT findings. Preoperative CT can therefore be useful for careful surgical planning when considering complete excision, which can also lower the risk of recurrence, which is higher in BPOP compared to the recurrence rate for osteochondroma. 3,12,17
BPOP lesions normally expand broadly in continuity with the cortical bone, producing a mushroom-shaped mass. The lesion is often confused with an osteochondroma as it is occasionally covered by a cartilage cap, with no accompanying bone destruction. 10 Preoperative CT imaging can confirm the absence of continuity between the lesion and the medullary cavity, compared to an osteochondroma, which is continuous with the medullary cavity of the bone. 11 Two previous case reports and our case did not have medullary continuity in plane X-ray and CT. 8,9 In one of these two previous cases, distinguishing the boundary between the mass and host medial sesamoid was difficult, similar to our case, and the mass in the other case was separated from the sesamoid. Although Matsui et al. reported the usefulness of preoperative MR imaging for arriving at a primary diagnosis, 4 in our case, it was difficult to distinguish the boundary between the mass and the host medial sesamoid and to confirm the absence or presence of continuity. In another study, Torreggiani et al. described the features of BPOP by MRI, specifically on low-signal intensity T1-weighted images and high-signal intensity T2-weighted and Short T1 Inversion Recovery (STIR) sequences in all cases. 18 In our case, the lesion presented with a low intensity signal on T1-weighted images and with heterogeneous intensity on T2-weighted and STIR images. Although we cannot specifically explain the difference between our findings on T2-weighted and STIR imaging and those previously described by Torreggiani et al., it is likely that these differences might have resulted from the long interval of continuous loading on the surface of the lesion, between its development and imaging (23 years). We did not investigate cytogenetic data in our case, which has been previously reported for BPOP, including t(1;17) (q32;q21) translocation and t(1;17) (q42;q23) translocation identified using chromosome banding and fluorescence in situ hybridization (FISH) analyses. 4,19
Conclusion
Here, we reported a case of BPOP involving the internal sesamoid of the hallux. Cases of BPOP involving the hallux sesamoid are exceedingly rare. Considering the high rate of BPOP recurrence after surgical excision, we performed complete resection of the lesion, and of the surrounding peripheral tissue, to reduce the risk of recurrence. Three years after surgery, the patient remains asymptomatic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.