
Abstract
Objective:
This study aimed to test the accuracy of the Synovasure®, α-defensin lateral flow test kit, in diagnosing periprosthetic joint infections (PJIs) in a predominantly Asian population and to evaluate whether other patient or disease factors may affect its results.
Methods:
61 Asian patients comprising 70 hip or knee prosthetic joints, performed between November 2015 and November 2018, were retrospectively evaluated. Cases were categorized as infected or not infected using Musculoskeletal Infection Society (MSIS) Criteria. Synovial fluid was tested for α-defensin using a commercially available kit. .
Results:
The Synovasure test had a sensitivity of 73.7% (95% confidence interval (CI): 48.8–90.9%) and specificity of 92.2% (95% CI: 81.1–97.8%) in an Asian population, which was slightly lower compared to previously reported studies in a predominantly Caucasian population. The positive predictive value was 77.8% (95% CI: 56.8–90.3%) and the negative predictive value was 90.4% (95% CI: 81.5–95.2%). The test had an area under curve (AUC) of the receiver operating characteristic (ROC) graph of 0.938, which represents an accuracy that is similar to synovial white blood cells (WBCs) and almost equivalent to that of synovial polymorphonuclear cells (PMNs). The presence of diabetes (p = 0.26), systemic inflammatory joint disease (p = 0.33), other metallic implants (p = 0.53), immunosuppression (p = 0.13), prior antibiotic usage (p = 0.99), and chronicity of symptoms (p = 0.34) was not significantly associated with a positive test in patients with PJI.
Conclusion:
The α-defensin lateral flow test kit is highly accurate in the diagnosis of PJI but with slightly lower sensitivity and specificity in an Asian population when compared with previous studies. The test should be used in conjunction with other MSIS criteria to provide clinically relevant and meaningful results for the diagnosis of PJI.
Introduction
Periprosthetic joint infection (PJI) is the most dreaded complication after successful arthroplasty surgery that can have profound medical and financial consequences on the patient, their support networks and health-care services. 1,2 While PJIs may be treated using a standardized algorithm and cutting edge implants, the diagnosis of PJI remains a challenge to most orthopedic surgeons and infectious disease specialists alike. 3 With increasing incidence, the length of hospitalizations and costs projected to exceed US$1.62 billion by 2020, 4,5 it becomes imperative to integrate new technologies to reduce the burden on the health-care system.
The updated Musculoskeletal Infection Society (MSIS) consensus criteria is widely utilized to diagnose PJI in an effort to standardize the definition of PJI. 6 It is based on a combination of preoperative and intraoperative markers (Table 1) that requires prolonged incubation in a laboratory setting and histopathological review by an experienced pathology specialist, frequently providing clinically meaningful results in a retrospective manner. 7 A single test nearing 100% accuracy that provides timely information for the surgeon could potentially negate the need for unnecessary hospitalizations, antibiotics, and delays to surgery.
The updated MSIS consensus criteria for the diagnosis of PJI.

CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cell; MSIS: Musculoskeletal Infection Society; PJI: prosthetic joint infection.
Interest in utilizing intrasynovial fluid biomarkers to diagnose PJI has increased after synovial white blood cells (WBCs) were found to have unique gene expression profiles in response to bacterial infections. 8 –11 Deirmengian screened 43 biomarkers based on previous studies and found five biomarkers to be 100% sensitive and specific for diagnosis of PJI utilizing MSIS criteria. 10,12,13
Defensins are antimicrobial peptides that are expressed by polymorphonuclear cells (PMNs), monocytes, lymphocytes, epithelial cells, and natural killer as part of the innate immune system to neutralize invading pathogens without prior sensitisation. 14 Defensin production is regulated by IL-1, IL-6, and TNF-α 15 and they exhibit antimicrobial activity against a wide spectrum of microorganisms including gram positive and gram negative bacteria, mycobacteria, and fungi. 16 –18 It has been shown to be elevated in patients with diabetes mellitus, 19 inflammatory joint disease, 20 and metallosis. 21
In vitro studies have shown that neutrophils release α-defensin as early as 4 h after stimulation and reach a peak after neutrophil apoptosis occurs. 22 The initial neutrophilic response attracts monocytes that differentiate into macrophage and converts the pro-inflammatory response into a proresolution response through an adaptive antimicrobial response. 23,24 The eventual result is the apoptosis of neutrophils and inhibition of α-defensin production and function. 22
The Zimmer Biomet Synovasure® lateral flow assay (Figure 1) is an intraoperative test kit that was originally developed by Citrano Laboratories for the diagnosis of PJI. 25 It utilizes a reagent strip with all of the critical components for the assay and can provide a diagnosis of PJI within 10 min. 26 The α-defensin lateral flow assay has been found to have sensitivities ranging from 67% to 92% and specificities ranging from 93% to 100% 21,25,26 and has been shown to have a pooled sensitivity and specificity that was lower than those of the laboratory-based immunoassay test. 27
Zimmer biomet Synovasure® lateral flow assay.
The study was designed to determine 1 the accuracy of the lateral flow assay for diagnosis of PJI in an Asian population and 2 to analyze the effects of diabetes, systemic inflammatory disease, presence of other metallic implants, immunosuppression, prior antibiotic usage, and chronicity of symptoms on the results of Synovasure.
Materials and methods
A retrospective review of 70 cases of suspected PJI utilizing the Synovasure lateral flow assay between November 2015 and November 2018 was performed. Institutional review board approval was granted for this study and patient’s clinical notes, perioperative radiographs, laboratory, and histopathological test results were reviewed.
All patients who were worked up for pain after a total hip or knee arthroplasty and utilized the Synovasure lateral flow assay as part of their work-up were considered for inclusion in this study. The cases were further subcategorized into first-stage, single-stage revisions and second-stage revision surgeries after explantation of cement spacers.
Patients were classified into either an infected group if they had either one major or three of five minor MSIS criteria or a non-infected group if they did not meet any of the MSIS major criteria and met 2 or less minor criteria. 6 Major criteria included two positive periprosthetic cultures with phenotypically identical organisms or a sinus tract communicating with the joint. Minor criteria included elevated serum C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), elevated synovial fluid white blood cell (WBC) count or ++ change on leukocyte esterase test strip, elevated synovial fluid PMN percentage, and positive histological analysis of periprosthetic tissue or a single positive culture. Cases where divided into acute or chronic PJI dependent on the acuity of the symptoms from date of index surgery. Acute PJI was determined if the symptoms occurred within 90 days of index surgery and the acceptable threshold for values utilized was based on the MSIS consensus criteria. 28
All synovial fluid was collected preoperatively or intraoperatively via needle aspiration or arthrotomy under aseptic conditions in the operating theatre by experienced surgeons who were trained by the distributor in utilization of the Synovasure lateral flow assay. A predefined volume of synovial fluid was collected by the provided Microsafe® pipetting tube and added to a premeasured dilution buffer in a dropper bottle. The contents of the bottle were mixed by gentle inversions and three full drops of the diluted sample were added to the immunoassay. Cellular material was removed by the first pad and test results were read after 10 min. The control line (“C”) was checked to confirm validity of the results and a test was determined to be positive if the α-defensin band (“a-D”) was visible on the same immunoassay.
Multiple fluid and tissue specimens were obtained and processed for aerobic and anaerobic bacteria, mycobacteria, and fungal cultures. Intraoperative fluid and tissue specimens were sent for cytology, to look for elevated synovial WBC count, and histologic analysis, with five or more PMNs in each of five or more high-power fields (×400) classified as a minor criterion for PJI. Patients with high suspicion of PJI were further tested with prosthesis sonication or bacteria genome polymerase chain reaction (PCR) testing whether initial results returned negative and cultures were kept for extended periods, up to 2 weeks, if initial culture results came back negative after 1 week.
For the purpose of analyzing the effects of different factors on Synovasure results, patients with PJI were categorized based on whether they had known diabetes, systemic inflammatory joint diseases, and presence of other metallic implants from clinical record review. Patients were classified as having prior antibiotic usage if they had antibiotics administered within 2 weeks of the diagnostic workup and were classified as immunosuppressed if they had been on chronic immunosuppressive medication such as steroids and cytotoxic medications for at least 3 months prior to work up. The chronicity of symptoms was calculated based on the time when the symptoms first started and median values of each category were calculated for purpose of the study.
Statistical analysis
Statistical analysis was performed via SPSS v20. The utility of Synovasure in predicting infection status was analyzed using sensitivities, specificities, positive predictive value, negative predictive value, receiver operator curves (ROC), and the area under the curve (AUC). The AUC was obtained from the ROC analysis to ascertain the discriminative ability of the Synovasure lateral flow assay diagnostic test kit. Statistical significance of AUC analysis was reached if the area of the calculated test is significantly different to 0.5.
Positive and negative predictive values were also calculated. A higher positive predictive value signifies a higher probability that the disease is present when the test is positive and a higher negative predictive value signifies a higher probability that a disease is not present when the test is negative. Relationships between Synovasure results and categorical variables were calculated using the Fisher’s exact test and t-test for continuous variables in testing for significance. A p-value of 0.05 or less was considered significant.
Results
Synovasure was performed on 69 patients and 78 joints. Of the 78 joints, eight were performed on native joints erroneously rather than prosthetic joints and were excluded. About 63 tests were performed diagnostically as joint aspirations to rule out PJI, prior to first or single-stage revision surgeries and before surgical procedures for debridement of superficial and deep abscesses. Seven tests were performed prior to cement spacer explantation and revision joint replacement to ascertain that PJI had been eradicated.
Of the 70 joints with suspected PJI, 47 were ethnic Chinese, 15 were Indian, and 8 were Malay patients with an average age of 67 years; 19 patients were diagnosed to have PJI according to MSIS criteria with 14 positive Synovasure results. Of the remaining 51 patients who tested negative for PJI according to MSIS criteria, 4 patients had positive Synovasure results. Seven patients had at least two phenotypically positive cultures taken on two different occasions and one patient had a sinus tract communicating with the infected joint. Of the patients who were diagnosed as PJI by having ≥3 MSIS criteria, three had one positive culture and seven were culture negative.
Sensitivity and specificity results
After statistical analysis, the overall sensitivity of the Synovasure test with lateral flow device was 73.7% (95% CI: 48.8–90.9%), the specificity was 92.2% (95% CI: 81.1–97.8%), the positive predictive value was 77.8% (95% CI: 56.8–90.3%), and the negative predictive value was 90.4% (95% CI: 81.5–95.3%). The overall accuracy of the Synovasure test was 87.1% (95% CI: 77.0–94.0%).
Sensitivity and specificity comparison with other MSIS criteria
When compared with other minor MSIS criteria, Synovasure had better sensitivity than having one positive culture, 57.9% (33.5%–79.8), but was less sensitive than synovial WBC, 89.0% (65.3–98.6%), serum CRP, 94.7% (74.0–99.9%), serum ESR, 100% (66.4–100%), and synovial PMN 100% (80.5–100%).
Synovasure had better specificity than serum ESR, 54.6% (36.4%–71.9%), serum CRP 77.6% (63.4%–88.2%), and synovial WBC, 83.3% (51.6%–97.9%) but had lower specificity than having one positive culture, 98.0% (89.6%–100%) and synovial PMN, 100% (73.5%–100%).
As a diagnostic test, Synvoasure had better positive predictive value than serum ESR, 37.5% (29.2–46.6%) and serum CRP, 62.1% (49.0–73.6%) but had lesser positive predictive value than synovial WBC, 88.9% (69.1–96.6%), having one positive culture, 91.7% (60.3–98.8%) and synovial PMN, 100%. It had better negative predictive value than synovial WBC, 83.3% (56.9–95.0%) and having one positive culture, 86.2% (78.7–91.4%) but had lower negative predictive value than serum CRP, 97.4% (84.9–99.6%), serum ESR, 100% and synovial PMN, 100%. Table 2 shows the sensitivity, specificity, and positive and negative predictive values of the Synovasure test in comparison to other minor diagnostic criteria.
Comparison of sensitivity and specificity of Synovasure and minor criteria.

PMN: polymorphonuclear cell; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cell; CI: confidence interval.
Accuracy results using ROC curve
Synovasure accuracy was determined by comparing the sensitivity and specificity of the test against other diagnostic criterion using the ROC curve and calculating the AUC. Synovasure (0.938) was more accurate than serum ESR (0.750) and serum CRP (0.819). It was as accurate as synovial WBC (0.938) and was marginally less accurate than having one positive culture (0.944) and synovial PMN (1.00). Figure 2 shows the ROC curves of all the evaluated minor criteria and Table 3 shows the AUC values with standard error and 95% confidence intervals.

ROC curves of Synovasure and other MSIS minor diagnostic criteria. the ROC: receiver operating characteristic; MSIS: Musculoskeletal Infection Society.
AUC values of Synovasure and other MSIS minor diagnostic criteria.
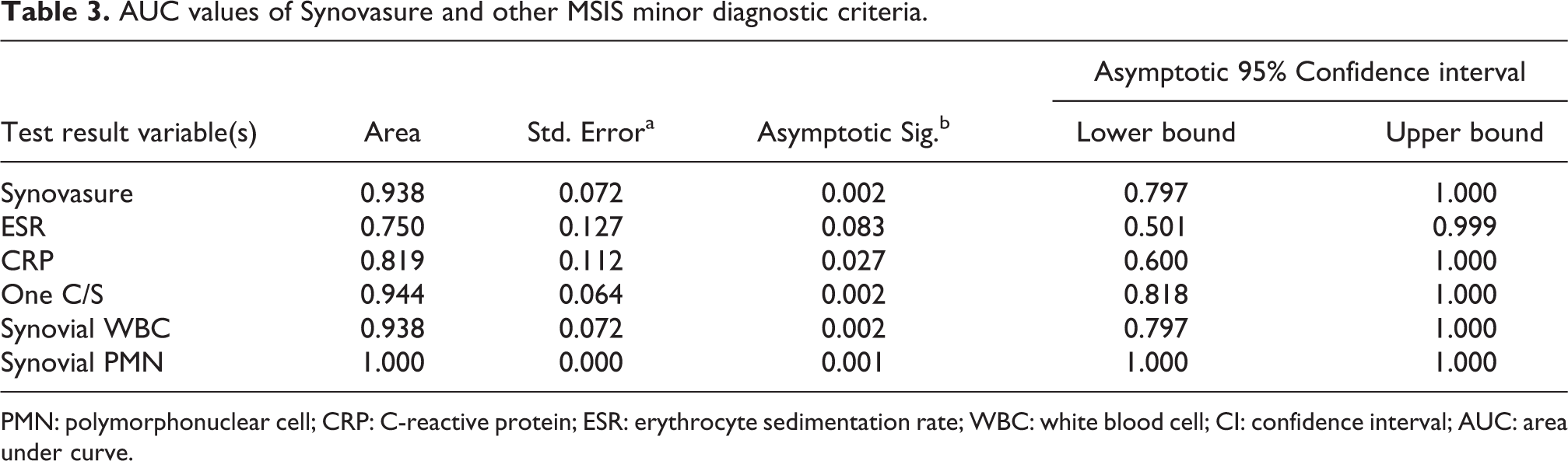
PMN: polymorphonuclear cell; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cell; CI: confidence interval; AUC: area under curve.
Effect of variables on Synovasure results in patients with PJI
Table 4 shows a comparison of variables and their correlation with Synovasure results. Diabetes (p = 0.26), inflammatory joint disease (p = 0.33), and presence of other metallic implants (p = 0.53) did not seem to be significantly correlated with Synovasure results. Prior administration of antibiotics (p = 0.99) and immunosuppresion (p = 0.13) also did not appear to be significantly associated with Synovasure results. Patients with a positive Synovasure test appeared to have a shorter median duration of symptoms, 3 days, compared to 3.5 days in patients with a negative test, but the results were not statistically significant (p = 0.34).
Comparison of variables with Synovasure result in patients with PJI.

PJI: prosthetic joint infection.
Results of microbiological cultures
Out of 19 patients with confirmed PJI by MSIS criteria, the most common pathogen was Staphylococcus aureus, 4, followed by Streptococcus pyogenes, 2. One patient had Enterobacter cloacae from intraoperative cultures but was not considered a PJI as none of the other MSIS criteria were positive. Eight patients were culture negative but diagnosed with PJI by other minor criteria and results of microbiological cultures are as shown in Table 5.
Results of microbiological cultures.a

MSIS: Musculoskeletal Infection Society; PJI: prosthetic joint infection.
aPositive culture in patients without PJI by MSIS criteria.
Ethical approval
The study was approved by institutional review board with process number 2017/00967.
Informed consent
Informed consent requirement was waived for the purpose of this retrospective study.
Discussion
This study represents the first report of the accuracy of the Synovasure lateral flow assay in a predominantly Asian cohort. The defensins are categorized into α-defensins, human neutrophil peptides (HNP) 1-3, and β-defensins based on their structure. 29 The defensins are encoded by genes located on chromosome 8p22-23, 29,30 with five known α-defensin genes in humans, DEFA1, DEFA3, DEFA 4, DEFA5, and DEFA6. DEFA1 and DEFA3 sharing a common locus, termed DEFA1A3, a site of frequent chromosomal rearrangements, resulting in the gene cluster displaying copy number variations (CNVs). 31
CNVs have a major role in the variation in human genome and significantly impact the allelic phenotype through coding sequence disruption, gene dosage, or long-range gene regulation. 32 Previous studies have found that the frequency and distribution of copy numbers among Asian vary significantly when compared with Caucasian and African populations and may have a profound impact on the way we utilize and interpret tests that measure defensin levels. 33 In addition, the effect of CNVs of DEFA1A3 and its impact on diseases such as inflammatory bowel disease, 34 inflammatory renal disease, 31,35 rheumatoid arthritis, 36 diabetes mellitus, 19 and susceptibility to severe sepsis 37 has been shown to be significant but still poorly understood.
The results of our study show that the sensitivity and specificity of the Synovasure lateral flow assay in Asians is slightly lower than the results from that in studies from the American and European populace. Gehrke et al., 21 Suda et al., 38 Sigmund et al., 26 and Kasparek et al. 25 reported a sensitivity of the lateral flow assay of 92.1, 81.2, 76.5, and 75%, respectively, which is similar to our findings of 73.7% sensitivity. Our study showed that the test had a higher specificity of 92.2%, which is similar to the results shown by Suda et al., 85%, 38 Sigmund et al., 94.7%, 26 and Kasparek et al., 93.3%. 25 Only Gehrke et al. reported a specificity of 100%, 21 which has not been replicated by other studies utilizing either the α-defensin laboratory-based immunoassay or lateral flow test. There were five false negatives in our series, with one patient having a sinus tract communicating with the joint, and the other four patients having elevated ESR, CRP, synovial WBC, and synovial PMN counts. All the patients had negative bacterial cultures and presented acutely, within 3 weeks of the symptom onset. There were four patients with false positive results. Two patients had chronic, progressive pain for more than 3 years and were tested prior to revision arthroplasty for implant loosening. The other two false positives presented acutely with pain of less than 2 days associated with elevated ESR and CRP levels. Cultures were, however, negative and there were no other positive MSIS criteria.
The high specificity of the test 7,27 underlines its utility in ruling out PJI when the index of suspicion is low, but the physician would like to rule out the prosthetic joint as a source of infection or prior to revision arthroplasty. Very few normal subjects would have a positive Synovasure lateral flow assay test, and hence the specificity (NIH—negative in health) would be very high. 39 As such, in a positive highly specific test, the probability of having a PJI would be high and clinicians should consider treating the patient as for PJI even if other readily available biomarkers such as ESR and CRP are equivocal at time of testing.
The sensitivity of the test from our study and previous literature is relatively lower 7,27 and may preclude its utility in the diagnoses of PJI, unless used in conjunction with other relevant biomarkers. A negative Synovasure lateral flow assay test would rule out PJI as very few diseased subjects would be expected to test negative on a highly sensitive test (PID—positive in disease). 39
When compared against other biomarkers utilizing the MSIS criteria, the Synovasure lateral flow assay appears to have good sensitivity and high specificity as well. 25,26 Utilizing the ROC curve, the test has an AUC of 0.938, which is similar to synovial WBC, and is only inferior in accuracy as a diagnostic test, to synovial PMN and having at least one positive culture. The Synovasure lateral flow assay measures the levels of α-defensin, which are produced by the synovial PMNs prior to sensitization and conversion to an adaptive immune response. 14,40 While the sensitivity of the test may not be as high as synovial PMNs, we believe the test may be useful as a surrogate marker and should be considered for inclusion as one of the minor MSIS criteria.
Prompt exclusion of PJI can benefit patients by allowing for less radical debridement and prosthesis retention. The leukocyte esterase (LE) test (Chemstrip 7 urine test strip; Roche Diagnostics) was recently reported to have a pooled sensitivity and specificity of 81% and 79%, respectively, in a meta-analysis of 545 patients. 41 The test measures the level of esterase enzyme produced by WBCs recruited to areas of infection and has now been included into the MSIS criteria as an alternative to measuring synovial WBCs. 6 For patients without a sinus tract and also have negative ESR and CRP levels, Leukocyte esterase strip test (surrogate for synovial WBC), α-defensin (surrogate for synovial PMN), and frozen section examination, the risk of having PJI would be extremely low and the need for single- or two-stage revision arthroplasties could potentially be avoided. The surgeon may be able to effectively rule out PJI at time of surgery through prior serological markers, highly accurate point-of-care tests and judicious examination of the joint.
While other studies have demonstrated a significantly higher level of synovial α-defensin in patients with rheumatoid arthritis, 13 this does not appear to be the case in patients with PJI. This could be due to the much higher levels of α-defensin required for the Synovasure lateral flow assay to have a positive test resulting in a nonstatistically significant correlation. Our study is also the first to show that the usage of immunosuppression did not appear to be statistically significant with the Synovasure results. This may be due to the defensins being produced as an initial response to infections, by a pathway that is not inhibited by conventional immunosuppressives such as steroids and methotrexate.
Metallosis has been shown in previous studies to be positively correlated with false-positive results. 21,42 Patients with diabetic nephropathy have also been shown to correlate with higher levels of serum α-defensin. 19 Our study shows that diabetes and presence of other systemic metallic implants were not correlated with higher synovial levels. As per previous studies done on lab based α-defensin immunoassays, 27,43 our results also show that prior antibiotic administration did not affect the results of the lateral flow assay.
The median duration of symptoms also does not appear to affect the synovial α-defensin levels. Ihi et al. showed that plasma human neutrophil peptides 1–3 were elevated at the onset of infection, with a gradual decrease in levels as the patient returned to recovery phase. 44 We hypothesized that this could be due to the innate immune system being sensitized to the pathogen and conversion from a pro-inflammatory response to a pro-resolution response, with an end result of decreased neutrophils and natural killer (NK) cells and an increase in macrophages. 23,24 Further studies that quantify the exact levels of synovial defensin using the lab based immunoassay may be useful in determining the half-life of the defensins and at which duration they may fall below the threshold for lateral flow assay testing.
Our study also shows that the Synovasure test responds to a wide variety of micro-organisms and is sensitive even for culture negative PJIs. The only false positive culture was in a patient with E. cloacae, which has relatively high virulence 3 and accounts for the majority of gram negative bacilli infections after Escherichia coli. 45 –47 It is possible that the result may have been a contaminant as the patient underwent primary revision arthroplasty without the need for long-term antibiotics or any complications.
Limitations
We appreciate that our study has several limitations. First, incomplete data for the classification of patients according to MSIS criteria could result in inaccurate results. Only 12 (15%) patients underwent histological testing and reporting either due to inadequate samples, inability to obtain synovial biopsies from joint aspiration alone, inconsequential testing as the patient was already deemed to have PJI from major or minor criteria or could not have PJI due to insufficient minor criteria. Second, the indication, duration, and type of antibiotics administered to the patients prior to surgery could not be ascertained for a small minority of patients as oral antibiotics were sometimes prescribed by general practitioners. Third, the sample sizes were small especially in the subgroup analyses of patients with risk factors such as diabetes, immunosuppression, and inflammatory joint disease. Larger numbers may be required to determine the true effect of such factors on the results of the Synovasure lateral flow assay.
Despite the acknowledged limitations of our study, we have demonstrated that the Synovasure lateral flow assay test is almost comparable in sensitivity and specificity when utilized in an Asian population. By comparing the accuracy of the test to other know MSIS parameters, we have shown that the test may serve to be a surrogate point-of-care marker for the current standards and should be considered for inclusion into the MSIS criteria, similar to the LE test. Our study, to the best of our knowledge, also demonstrates the first study to try and evaluate the effects of immunosuppression on the results of the Synovasure test.
Previous studies that utilized the Synvoasure lateral flow assay were supported by Zimmer Biomet, through supply of the lateral flow test kits or had unspecified funding sources. While there may be concern about bias and industry sponsorship in these studies, our study represents an unbiased reporting of the results.
Conclusion
In conclusion, the Synovasure lateral flow assay is a highly accurate test that has good utility when used in conjunction with other MSIS parameters for the diagnosis of PJI. The sensitivity and specificity of the test in our Asian population appears to be slightly decreased when compared to previous studies in Caucasian populations and may warrant further investigation in larger prospective cohort trials. Further studies may be required to determine whether it can be a surrogate marker for Synovial PMNs and to determine the effect of diabetes, inflammatory joint disease, and immunosuppression on the results of the test.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.