
Abstract
Infection is one of the commonest causes for megaprosthesis failure. The current treatment includes antibiotics but no surgery, debridement, prosthesis removal and joint fusion, prosthesis revision or amputation. Success in controlling infection may be less than 50% in implant revision. The overall risk of amputation is more than 20%. We believe that repeated debridement with antibiotic-laden cement wrap (ALCW) may be a reliable alternative for managing the megaprosthesis infection. The purposes of this article are to identify whether ALCW is an effective way of eradicating the megaprosthesis infection, the associated complications and the functional outcome after management by ALCW.
Methods:
This was a retrospective study of patients with megaprosthesis infection. From January 2014 to June 2016, there were five patients with tumour megaprosthesis infection who had undergone the ALCW procedure. Ages ranged from 17 to 59 years of age. Male to female ratio was 4:1. The patients studied had humeral (1), proximal femoral (1), distal femoral (1) and proximal tibial (2) prostheses. All patients had follow-ups more than 1 year (21–52 months) after treatment.
Results:
All patients recovered from their implant infection and the implants were retained in all patients. There was no sign of infection in the most recent follow-up. One patient died of osteosarcoma recurrence. One patient had a large block of cement causing plastic insert dislodgement in the shoulder joint 1 year after surgery. Another patient with a dislocated hip cup had revision carried out in the final debridement. The most recent Musculoskeletal Tumor society (MSTS) scores ranged from 21 to 30. All patients were satisfied with their treatment.
Conclusions:
In this preliminary report of a small number of patients, ALCW has achieved 100% infection control. ALCW may be an easy and effective alternative for managing the megasprosthesis infection. The complications associated can be avoidable. The functional outcome is excellent.
Introduction
Periprosthetic infection in megaprosthesis reconstruction after massive bone tumour resection is an enormous problem for orthopaedic tumour surgeons. Not only the risk of megaprosthesis infection is high (3–31%) due to multiple unfavourable factors such as a big wound, lengthy surgery, lack of soft tissue coverage and chemotherapy 1 –3 but also the management outcome is not very satisfactory. The megaprosthesis infections were categorized as ‘acute’ if they occurred within 4 weeks post-operatively, as ‘early’ if within 4 weeks to 2 years post-operatively or ‘late’ if more than 2 years. 3,4
Currently, the treatment options include antibiotics only, debridement with implant retention, one-stage or two-stage surgery, resection arthroplasty, arthrodesis and amputation. 2,3,5 –10 The overall infection control is only 75%. 3,8 Local treatment with lavage, debridement and antibiotics has been reported successfully in only 6% of patients. 8 Most of the patients’ infections have to be managed by implant removal or amputation. 3 The rate of amputation ranges from 21% to 87%. 3 For the one-stage revision, it is only advised for the acute infection. 3 For two-stage surgery (implant removal followed by second-stage reimplantation), the success rate for infection control is reported as 94% at 6 months, 91% at 1 year, 74% at 5 years and 65% at 10 years. 6
However, to remove a well-fixed infected implant in an emergency situation is not a complication-free procedure, especially as an emergency surgery. 11 Therefore, a more conservative approach with surgical debridement only is indicated in some patients in some situations. Because of this background, we have adopted a standard approach for megaprosthesis infection. If the soft tissue condition of the patient is satisfactory and the stem is stably fixed to the bone, the patient will be treated by repeated debridement with antibiotic-laden cement wrap (ALCW).
The primary aim of this study is to review our preliminary results of using this approach, which retains the implant. Specifically, we asked whether ALCW is an effective way in eradicating the megaprosthesis infection, the associated complications and the functional outcome after management by ALCW.
Patients and method
This study retrospectively reviewed patients with megaprosthesis managed by ALCW at our hospital. It has been approved by the institutional review board (reference number: UW15/414). The hospital records were retrieved and reviewed. No patient was called back for the review.
From January 2009 to December 2016, 58 patients underwent megaprosthesis reconstruction for limb tumour surgery. Of 58 patients, there were six prosthetic infections, demonstrating the risk of infection as being 10%. Of these six patients, there was one patient managed by staged surgery with implant removal and reimplantation. He was excluded from this report.
The diagnosis of infection was confirmed by both clinical presentation and bacteriology study. All patients signed an informed consent form for debridement and ALCW. They also agreed to implant removal if intraoperative condition deemed it necessary.
Surgical procedure
Before surgery, all patients had a full assessment, including white cell count (WCC), C-reactive protein (CRP) and the erythrocyte sedimentary rate (ESR). Bacteriology study by blood culture and local tapping under aseptic technique was performed. Antibiotics were then started empirically according to each individual’s medical background.
During the first surgery, the soft tissue condition and the implant status were assessed. The prerequisite for ALCW was relatively healthy soft tissue coverage. In addition, there should be no skin tension in the wound closure after the cement had been added onto the implant. Moreover, the stem should be stably fixed to the bone; otherwise, the surgeon would remove the implant and staged revision should be implemented.
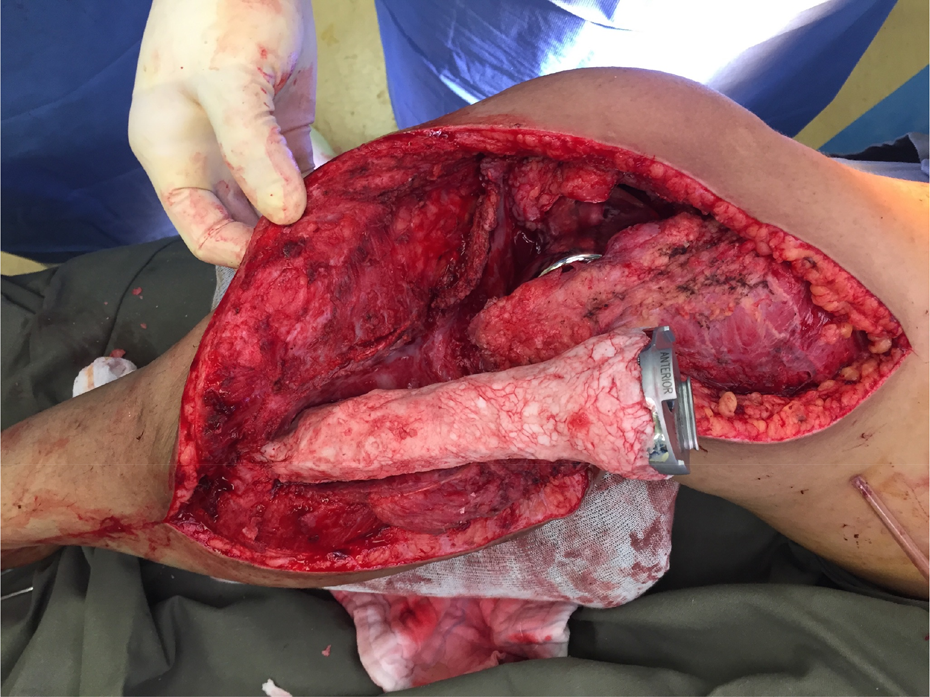
The debridement began with the removal of the detachable parts of the implant. Then the infected implant was thoroughly cleansed with antiseptics. At the same time, a radical debridement was carried out. All loose granulation tissue was removed; however, the scarred fibrous wall was left behind to avoid any neurovascular bundle injury. Following that, the detachable parts would be put back or replaced by new components. The implant was then subsequently wrapped with a layer of antibiotic-laden cement (Figures 1 to 4). The choice of antibiotics in the cement depended on the bacteriology and the antibiotics must be heat stable to avoid change in chemical properties and drug efficacy due to exothermic reaction during cement curing. For a typical patient, we added 3 g of vancomycin into the commercially available 40 g of tobramycin cement. The kind of antibiotics may be modified according to our microbiologist’s advice. In most of the patients, one and a half packs of cement were good enough to cover the exposed implant. After surgery, patients were only allowed full motion after drain removal.

Intraoperative photograph of ALCW (patient 3). ALCW: antibiotic-laden cement wrap.

Post-operative X-ray of ALCW (patient 3). ALCW: antibiotic-laden cement wrap.
Proximal tibia megaprosthesis infection managed with ALCW (patient 4). ALCW: antibiotic-laden cement wrap.

Proximal humerus ALCW (patient 2). ALCW: antibiotic-laden cement wrap.
Based on clinical and infection parameters (latest intraoperative tissue culture must be negative), the patient may undergo further debridement surgery. Each time, the outer layer of cement would be removed and replaced by a new layer of cement. Patients were discharged after infection was under control, evidenced by the clinical and laboratory findings. The antibiotics would continue for a longer term, based on the latest positive culture and sensitivity result. If necessary, we would ask for the microbiologist’s advice. The duration of antibiotics treatment was assessed on an individual basis. Meanwhile, patients had a course of physiotherapy to improve the functional outcome.
Patients then received regular follow-up in our outpatient clinic with regular X-ray and blood investigations including WCC, CRP and ESR. Functional assessment by the Musculoskeletal Tumor society (MSTS) system 12 was performed when the functional status was optimized. The minimum follow-up was conducted at 21months (median 43 months, ranging from 21 months to 52 months).
Results
The hospital records were retrieved in order to assess the outcome of the treatment, including infection status, complication and functional outcome. There were five patients with tumour megaprosthesis infection who had undergone the procedure. Ages ranged from 17 to 59 years of age. Male to female ratio was 4:1. The implants involved included humeral (1), proximal femoral (1), distal femoral (1) and proximal tibial (2) prostheses. One was acute infection; one was late infection, while the others were early infection. The bacteriology included methicillin-resistant coagulase-negative staphylococci (1), methicillin-sensitive coagulase-sensitive staphylococci (1), methicillin-resistant Staphylococcus aureus (1), methicillin-sensitive S. aureus (1), group G streptococci (1), diphtheroid bacilli (1) and extended-spectrum beta-lactamase Escherichia coli (1; Tables 1 and 2).
Patients with megaprosthesis infection managed by ALCW.

ALCW: antibiotic-laden cement wrap; MRSA: methicillin-resistant Staphylococcus aureus; ESBL: extended-spectrum beta-lactamase.
Outcome of the patients with ALCW treatment.

ALCW: antibiotic-laden cement wrap; FU: follow-up.
There were no intraoperative or early post-operative complications. One patient recovered after one debridement and ALCW. The other three recovered after three debridements and ALCW. The last patient recovered after six debridements and ALCW. The implants were retained in all patients. One patient died of osteosarcoma recurrence 21 months after control of infection.
In the most recent follow-up, there was no sign of infection clinically, radiologically or by blood parameters. Three patients had reopening surgery and culture swabs were taken, all being negative. The latest median functional (MSTS) score was 25/30 and it ranged from 21 to 30 (21, 22, 25, 30, 30). All patients accepted the ALCW treatment according to the MSTS score ‘emotional acceptance’ assessment.
There was one patient who had a cement block at the axilla of the total shoulder replacement, causing plastic insert dislodgement in the shoulder joint 1 year after surgery (Figure 5). The cement was trimmed down by open surgery.

Dislocation of plastic insert in reversed shoulder replacement due to the cement block (patient 2).
Another patient suffered from plastic hip cup dislocation (Figures 6 and 7). At the first debridement surgery, the bipolar hemiarthroplasty of hip was converted to cemented total hip replacement without removal of cartilage of acetabulum in order to avoid spreading infection into the acetabulum. The initial plan was to have the formal conversion in 3 months post infection. Unfortunately, the dislocation of the cup was at 8 weeks post infection and formal conversion was then performed.

X-ray hip and the proximal femur after ALCW (patient 1). ALCW: antibiotic-laden cement wrap.

Revision to a standard cup implantation after cup dislocation (patient 1).
Discussion
Periprosthetic megaprosthesis infection is a very serious event in limb-sparing surgery compromising functional outcome of the patients and their quality of life. 6
The knowledge we have in total joint prosthesis infection may be applicable to tumour megaprosthesis infection. To define a total joint prosthesis infection, both clinical and laboratory results are taken into consideration. Conditions such as (1) sinus tract, (2) positive culture in intraoperative tissue or synovial fluid, (3) ≥5 neutrophils/high power field of intraoperative specimen, (4) >1700 leukocytes/μL and/or >65% neutrophils in the joint fluid, (5) sign of infection clinically or by laboratory finding and (6) sign of infection radiologically are considered as prosthetic infection. 13 Four of our patients were confirmed as being infected by positive bacterial culture in both intraoperative tissue and synovial fluid. The other patient was confirmed by perianal abscess, local clinical sign of infection in shoulder and positive blood culture.
Concerning the management, total joint prosthesis infection and tumour megaprosthesis infection are considered as two different disease entities even though there are some similarities. For tumour megaprosthesis infection, there is a higher chance of management failure resulting in limb amputation. 3,8 Differing from total joint prosthesis infection, there are only a few reports on the tumour megaprosthesis infection to advise us on the best treatment option and to guide our management because the incidence of megaprosthesis infection is much lower. The Royal Orthopaedic Hospital Oncology Service, one of the biggest orthopaedic tumour centres, had only 136 patients within 37 years of hospital records. 8 In addition, background variation among different tumour patients makes interpretation of the results much more difficult than the joint prosthesis infection.
The current management of tumour megaprosthesis infection includes conservative management with long-term antibiotics suppression, conservative surgery (exchange of modular part or the plastic bearing), amputation, implant removal and joint fusion, resection arthroplasty and one- or two-stage revision. 3 Partial two-stage exchange may be another option in managing these infections with a well-fixed stem. 11 It is not clear which treatment solution is the best at the moment. 5
Debridement, antibiotics, implant retention (DAIR) in total joint prosthesis infection is one of the standard treatments. However, the success in controlling the infection varies from 31% to 100%. 13,14 –17 Although the term DAIR is not used in megaprosthesis infection papers, the outcome of debridement and implant retention in this group of patients has been very poor. Jeys et al. reported that there were 68 patients of 136 patients treated with local debridement. Of these patients, only four patients recovered. 8 Overall, 37% (50/136) of their patients had limb amputation.
The main difference between the ALCW and the DAIR in the management of megaprosthesis infection is the layer of cement wrapping on the metallic implant in ALCW leaving minimal exposed surface. Although antibiotic-laden cement beads can provide a local high concentration of antibiotics, the metal surface is still completely exposed in the bacteria-bearing body fluid. By such small modification of DAIR (cement wrap), we have achieved 100% infection control.
Mavrogenis et al. 3 reported 100 megaprosthesis infections in 1161 patients. Only 11 patients had acute infection and 16 patients had early infection, whereas 73 patients had late infection; 83 patients underwent two-stage revision. In addition, five patients required amputation. The overall implant retention after definitive management of infection was 88% at 10 years and 84% at 20 years. Unfortunately, the overall infection control was only 75% and the other 25% of the patients had recurrent infection.
All of our patients were diagnosed as infected in the early phase of infection. Four of the five had infection diagnosed clinically on the same day when there was onset of symptom. The other patient (patient 5) presented slightly delayed and it was on day 3. Whether ALCW could be applicable to delayed presentation patient is not certain in this small series.
Hardes et al. found that using silver-coated megaprostheses in bone sarcoma reconstruction surgery reduced infection rate from 17.6% to 5.9% 1 and from 16.7% to 8.9% in tibia megaprosthesis reconstruction. 18 However, if the silver-coated megaprostheses was used for stage 2 reimplantation in two-stage revision, the result was not promising. Zajonz et al. 19 reported that the silver-coated megaprosthesis reimplantation in cured infection carried a high reinfection rate of 40%. The average time for reinfection was 14 months.
Before the practice of ALCW in our hospital, all these infection patients were managed by DAIR or two-staged revision if DAIR had failed once, or if they had implant loosening or associated poor soft tissue condition. Unfortunately, removal of stably fixed implant and intramedullary cement was a painstaking, prolonged and risky procedure. In this ALCW series, only one patient was excluded from ALCW because of unfavourable soft tissue condition and he, therefore, had staged revision. The other five patients were treated with a less aggressive approach by ALCW, although the number of debridement surgeries was more than the conventional practice in some patients. For these patients, we could achieve 100% infection control and 0% recurrence with 43 months median follow-up (21, 23, 43, 47, 52).
‘Cure’ in total joint infection is defined as absence of clinical, radiological sign of infection and normal laboratory findings 13 at a follow-up visit more than or equal to 2 years post antibiotics treatment. The CRP should be less than 10 mg/L and erythrocyte sedimentation rate should be less than 20 mm/h. If it is less than 2 years, it is defined as ‘probable cure’.
Our patients did not have any sign of infection at the most recent follow-up. If we apply the term ‘cure’ and ‘probable cure’ of total joint infection in our patients, three were in ‘cure’, while the other two were in ‘probable cure’ at the latest follow-up. Three patients had their wounds reopened; one was for shoulder plastic insert relocation, one was for acetabular revision and the other had hindquarter amputation for symptomatic regional osteosarcoma in the pelvis. Intraoperatively, we had taken culture swabs for bacteriologies. All were negative. Whether these implants were sterilized by the layer of ALCW, or the bacteria were suppressed, is yet to be ascertained and this may form an area for future study.
The ALCW procedure is simple. The layer of cement is wrapped around the implant before wound closure. Therefore, there is some increase in the diameter and the final volume of the implant. Hence, the prerequisite of this procedure is having relatively healthy soft tissue around the implant especially for those with late infection. Otherwise, upon closure, the skin will be under tension and without a doubt the infection will persist.
Various treatment methods had been advised for managing the megaprosthesis infection. However, there is not any one that is considered more superior than the others. 5 If all implanted parts can be removed in the two-stage revision, we can presume that the infection focus no longer exists. To remove a well-fixed stem may be a disaster. Hence, there are reports on the partial implant removal. 3,11 In our patients, we would also advise exchange for all detachable parts, in order to minimize the bacterial load and remove the biofilm, 20 if any. This may not be possible for the custom-made prostheses.
The cost of ALCW is low. Merollini et al. 21 stated that the average cost of the debridement and implant retention was AUS$13,187, which should be much lower than the traditional two-stage implant exchange of megaprosthesis. However, the exact amount of two-stage implant exchange will vary according to the kind of megaprosthesis to reimplant.
We had two delayed complications. The first was in a young lady with total shoulder custom-made megaprosthesis for extra-articular resection of the shoulder joint with proximal humerus for extensive osteosarcoma. The axilla of the shoulder prosthesis was rather spacious and in order to fill the dead space, a large piece of cement was placed in the cavity. Unfortunately, it served as a hinge to dislodge the plastic insert from the linked implant when the cement block kissed the scapular component 1 year after the infection had been controlled. The patient required relocation of the plastic insert and trimming of the cement block.
For the other patient, who had megaprosthesis bipolar hip, we understood that the cartilage was avascular and it might be a focus of persistent infection. On the other hand, removal of cartilage might spread the infection into the acetabular cancellous bone. This might result in softening of the acetabular bone, early acetabular bone collapse and subsequent protrusio. We left the cartilage untouched as in Kazimoglu et al.’s report. 15
We deliberately changed the bipolar hip component into a total hip component in order to leave a big piece of antibiotic-laden cement inside the acetabulum. As the cartilage of acetabulum still looked healthy and intact at that time, the intraoperative decision was to have cartilage removal in the second-stage formal cup reconstruction. Instead, the cup was cemented onto the intact cartilage. The formal conversion was planned at 3 months after infection was under control. Unfortunately, the cup dislocation from the acetabulum happened at 8 weeks post-operatively when the infection was under control. At the time, the patient became more active as he was totally asymptomatic. Eventually, the cup was revised to a standard total hip acetabular cup implantation. We believe that these complications may be avoidable if we can be more meticulous in handling cement wrap.
The patients’ function was assessed by the MSTS system. 11 The median score was 25/30 (21, 22, 25, 30, 30). The overall functional status was excellent. However, we could not find any large case series on the functional outcome after management of megaprosthesis infection. We believe that the heterogeneous nature, the variation in pre-infection functional status and the rarity of this disease make the analysis of functional outcome very difficult to conclude. Nevertheless, our patients’ functional outcome appears quite promising (Table 3).
MSTS scoring of ALCW patient.
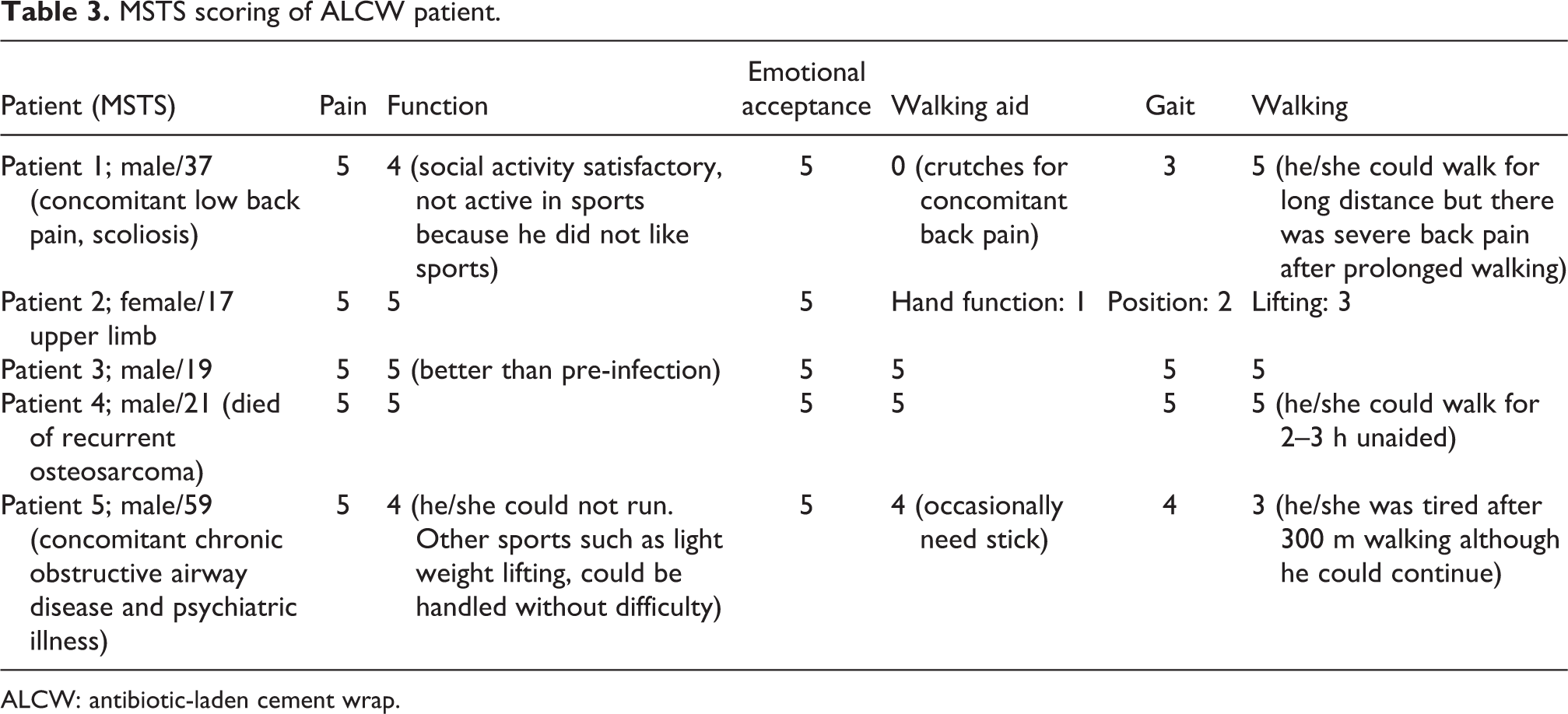
ALCW: antibiotic-laden cement wrap.
There are a few limitations to this study. (a) This is a retrospective review. (b) In addition, the number of patients is small and heterogeneous, although they are managed by a single surgical method. A literature search through Medline shows that there had been only three larger case series reports of 31, 100 and 136 patients. 3,5,8 Jeys et al.’s report has already included 37 years of the hospital records. 8 However, they reported different types of surgical treatment with each type only having a few patients. Other than these three reports, the others were small patient-number case reports. 7,22 (c) The antibiotics treatment based on the sensitivity of microbacteria also varies from patient to patient. (d) The follow-up is relatively short. Longer follow-up and further study are required.
Conclusion
This simple but efficient procedure has shown promising results in managing megaprosthesis infection in our small patient series. There was 100% infection control, 100% implant retention for the non-detachable parts and 100% limb sparing. The complications associated may be avoidable and the functional outcome is excellent. If we have a longer follow-up and if excellent outcome is replicated by others, it may be the first surgical option for the megaprosthesis infection.
Footnotes
Acknowledgement
The authors thank Ms Carol Anne Higgins for her contribution in proofreading the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.