
Abstract
Purpose:
The study aimed to evaluate the efficiency of the posterior-only approach using shaped titanium mesh cage for surgical treatment of spinal tuberculosis (TB) in children.
Methods:
Between January 2011 and July 2013, 22 children with a single motion spinal segment involved, including 10 with thoracic, 4 with thoracolumbar, and 8 with lumbar, were enrolled in the study. The patients were treated by the posterior-only approach using the shaped titanium mesh cages. Their medical records and radiographs were retrospectively analyzed.
Results:
The mean operating time was 163 min (ranging from 120 min to 200 min). Blood loss was 210–550 ml with an average of 300 ml. The mean follow-up period was 41.1 months. At the final follow-up, all patients showed a solid bony fusion without the infection recurrence. The average bone fusion time was 6.2 months. The average correction of the local segment kyphosis angle was 6.9° (from 9.2° preoperative to 2.3° postoperative). Minimal loss in correction angle was noted in these patients at the final follow-up (only 1.5°). Changes in erythrocyte sedimentation rate, local segment kyphosis angle, and neurological status demonstrated a significant clinical improvement in all children at their last follow-up.
Conclusion:
Children with spinal TB of a single motion spinal segment involved can be successfully treated by the posterior-only approach using shaped titanium mesh cage. It is a minimally invasive, safe, and effective surgical procedure.
Introduction
Spinal tuberculosis (TB) is the most common form of extrapulmonary TB and is one important cause of kyphosis in developing countries. It is estimated that 30 million people have active TB, and 2 million of these have spinal TB. 1 TB in children is reflected in a significant proportion (15–40%) of all TB cases since they are a susceptible population because of the combined effects of known risk factors such as malnutrition, human immunodeficiency virus infection, and immature immune systems. The plight of children with TB has been widely recognized and is increasingly becoming a priority for national TB control programs. 2
The thoracic and lumbar spine are often involved in both pediatric and adult spinal TB. The anterior and middle spinal columns of spine show wide destruction with paravertebral abscesses and narrowing of intervertebral spaces. However, different from the adult spinal TB, pediatric TB has its own characteristics involved with children’s growth and development. The normal growth of the posterior column is not usually involved, so the kyphosis may be constantly aggravated because of an imbalance in spinal growth. The deformity affects the appearance and is often accompanied by clinical manifestations, cardiopulmonary insufficiency, nerve compression, and paralysis, all of which have an effect on a patient’s physical and mental health. Although the administration of anti-TB drugs is critical to the treatment, the deformity when treated with chemotherapy alone may continue to progress and even develop into a serious rigid deformity. 3 Thus, the primary aim of the treatment, which may incorporate surgical intervention, should include attempts to prevent kyphosis. Various approaches have been reported for the treatment of children with spinal TB. These approaches include the anterior approach, single-stage anterior and posterior approaches, or staged anterior and posterior approaches. 4 –6 In recent years, due to the refinement of surgical techniques and rigid spinal instrumentation providing three column supports, now the posterior-only approach has now become more popular. 7 Another factor determining the success rate of the surgery is the proper choice of the bone graft. The debate concerning bone grafting options, including autograft, allograft, and titanium and stainless steel cages, is ongoing. This study aimed to evaluate the safety, feasibility, and efficacy of debridement, internal fixation, and reconstruction using shaped titanium mesh cages for a posterior-only approach for the treatment of spinal TB in the pediatric population.
Patients and methods
Population and clinical presentation
Between January 2011 and July 2013 at our spine center, a total of 22 consecutive pediatric thoracic and lumbar spinal TB cases were treated via the posterior-only approach using the shaped titanium mesh cage at our spine center. All surgical procedures were performed by the same surgeons. There were 8 males and 14 females with an average age of 9.5 years (range 4–16) with a minimum of 3-year follow-up. The cases included 10 thoracic TB, 4 thoracolumbar TB, and 12 lumbar TB. Only the children with a single motion spinal segment involved (two adjoining vertebrae and their intervening discs) were enrolled in the study (Table 1). This study was approved by the Ethics Committee. Written informed consent was acquired from the legal guardian of the patients to authorize treatment, image findings, and photographic documentation.
Clinical data of all patients.

ESR: erythrocyte sedimentation rate.
The diagnosis of pediatric spinal TB was first based on the clinical manifestations closely combined with laboratory parameters and radiologic findings (X-ray, computed tomography, and magnetic resonance imaging) and then was confirmed pathologically. The local kyphosis angle was measured on the lateral plain film taken using the Cobb method. All patients presented with anorexia, general malaise, loss of weight, back pain, muscular spasms, and limited motion of the spine. Low fever and night sweats were only seen in 14 cases, pulmonary TB in 6 cases, and neural function impairment in 18 cases. The images showed the destruction of the vertebral body and narrowing of intervertebral space, prevertebral abscess, and sequestration. The Frankel system was used to evaluate the neural function deficiency: (1) three cases were classified as grade B, (2) six cases were classified as grade C, (3) nine cases were classified as grade D, and (4) four cases were classified as grade E. The average erythrocyte sedimentation rate (ESR) was 50.8 mm/h (range 19–78).
The anti-TB drug treatment depended on individual drug dosing and lasted at least 2 weeks preoperatively. For the children weighing <10 kg, the rifampicin dose was 75 mg/day, isoniazid 75 mg/day, and ethambutol 200 mg/day. The doses were doubled, tripled, and quadrupled when the weight ranges were 10–17 kg, 18–25 kg, and > 25 kg, respectively. 8 It was advised that the doses be adjusted according to the weight range. The treatment plans were formed in consultation with pediatricians, and the side effects were monitored closely and carefully. When the ESR and temperature returned to normal or significantly decreased, surgery was done.
Surgical procedure
Under general anesthesia with somatosensory-evoked potential monitoring, the children were kept in a prone position. A midline incision was made, and an extraperiosteal dissection was performed. In thoracic TB, the exposure area included the costotransverse articulations and 3–5 cm of the medial ribs bilaterally. Under C-arm fluoroscopy guidance, pedicle screws or hooks were installed at one or two levels above and below to the level of decompression in order to provide short segmental fixation. The affected vertebrae were planted by the screw if the upper part had not been destroyed. The mild-side rod then was fixed temporarily in order to avoid the spinal cord injury and focal debridement during the decompression and focal debridement. The next step included lesion debridement to drain the prevertebral abscesses and expose the diseased vertebral bodies at the more worse side of the affected vertebrae. In the thoracic segment, we resected the facet joint and the lower costotransverse joints and a short fragment of adjoining rib but kept the contralateral structural integrity. After that, all lesions (sequestra, abscesses, and granulated tissues) would be removed using various sizes of spatulas and angles under the direct vision. Abscesses were drained using incubating the urethral catheter directly in the cavity thoroughly. The permanent rods were then placed to correct the deformity. One or two shaped titanium mesh cages filled with autogenous bone (healthy lamina, spinous process) on both sides and allograft bone in the middle according to the cavity width and length were installed into the interbody (Figures 1(e) and 2(d)). The two rods were compressed in order to tighten the cage and then fixed in position. The strip-sized autogenous or allograft bone was imbedded in the posterior body in order to fuse the segments of the defect; 1.0 g streptomycin and 0.3 g isoniazid were used locally. Drainage was performed properly. The specimen was sent for culture with chemosensitivity testing and histopathological examination.

A 9-year-old girl with spinal TB in T12–L1. (a) to (c) Preoperative images showing destruction and collapse of vertebral body resulted in the spine instability and angulation anomaly. (d) The shaped titanium mesh cage. (e) and (f) Postoperative X-ray demonstrating good internal fixation and the correction of the deformity. (h) to (j) Three-year follow-up images showing the good bone fusion and no loss of the corrective angle. TB: tuberculosis.
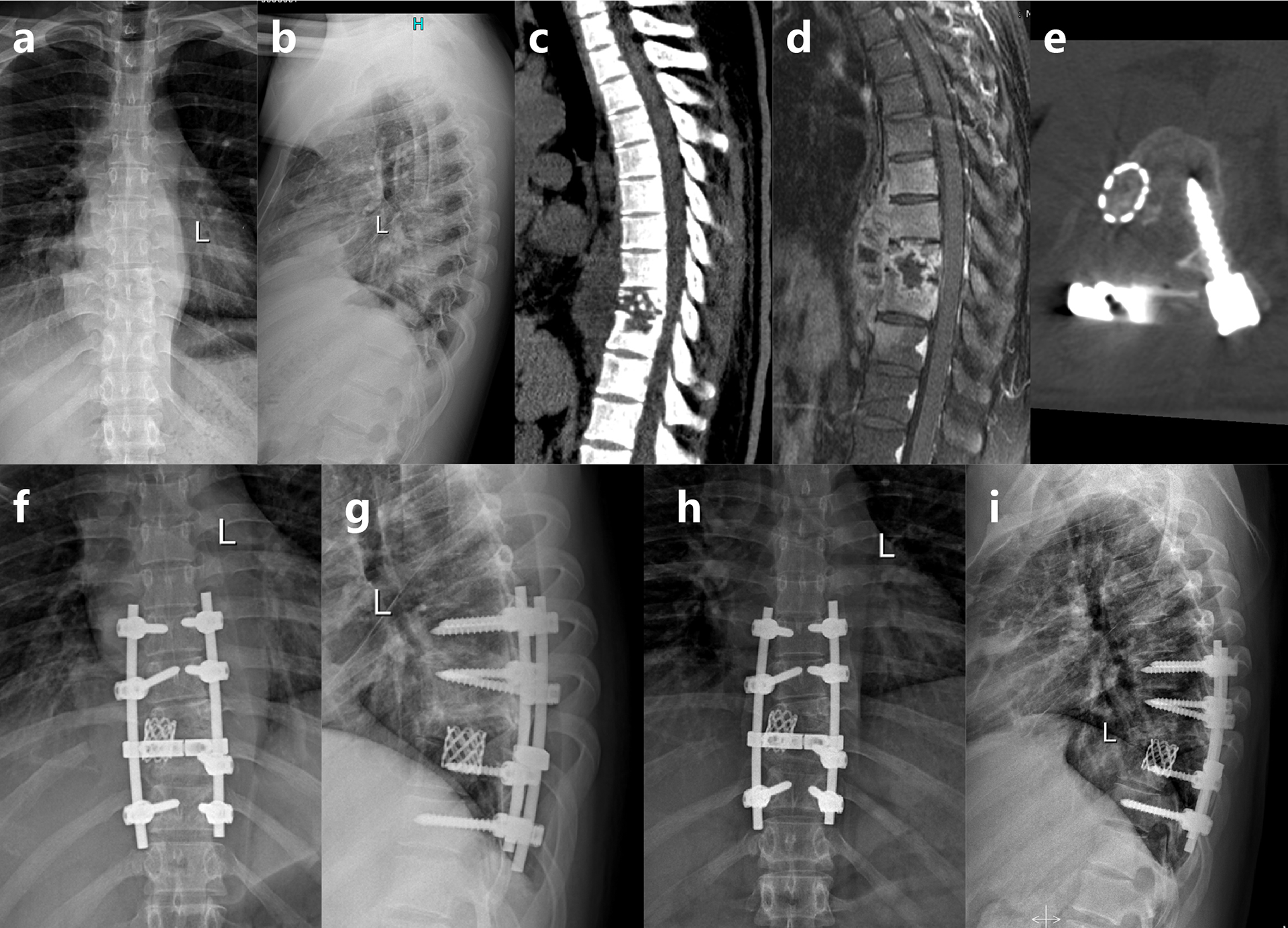
A 16-year-old boy with spinal TB in T9–T10. (a) to (d) Preoperative images showing disease involving T9–T10 and intervertebral space, leading to the formation of dead bone and paravertebral abscess. (e) The shaped titanium mesh cage. (f) and (g) Postoperative X-ray demonstrating good internal fixation. (h) and (i) Four-year follow-up images showing the good intervertebral fusion and maintenance of the correction. TB: tuberculosis.
Postoperative management and follow-up
Because of children with low compliance and weakened bones, all patients were directed to stay in bed and wear the external brace in order to prevent spine overactivity, which could result in the internal fixation loosening and screw cutting. The drainage tubes were removed when the drainage volume was <30 ml/24 h. We adopted an anti-TB chemotherapy regimen of 2HRE/9-12HR. Other postoperative treatments which included strengthening of nutrient intake, nutrition for nerves, and functional rehabilitation exercises were added. Regular follow-ups were performed until skeletal maturity was achieved. Frankel grade, ESR, and local kyphosis angle were determined and evaluated. The average follow-up period was 41.1 months (range 36–50 months).
Results
The mean operative time was 163 min (range 120–200 min), and the blood loss was between 210 ml and 550 ml with an average of 300 ml. There were statistically significant differences between preoperative ESR and 3-month follow-up ESR (p < 0.05). The image showed the correct implant placement. There were no nerve palsies or infection. No damage to blood vessels occurred. All wounds healed without chronic sinus formation. The average correction of the local kyphosis angle was 6.9° indicating a decrease from 9.2° preoperative to 2.3° postoperative (p < 0.05). Minimal loss of correction angle was noted in these patients at the final follow-up (only 1.5°). It was still significantly improved in comparison with the preoperative measurements (p < 0.05). Neurological deficits of the children had improved to a significant degree based on the Frankel classification. At the last visit, three cases were classified as grade D, and the others were all grade E. In all patients, the ESR returned to normal within 3 months in all the patients. No obvious side effects were found. Bone fusion was achieved within 3–7 months (average 6.2 months; Table 1). No complications related to instrumentation and titanium mesh cages occurred (Figures 1 and 2).
This study was approved by Xiangya Hospital Ethics Committee of Xiangya Hospital Central South University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Written informed consent was acquired from the guardian of each patient to authorize treatment, image findings, and photographic documentation. All the authors have reviewed the manuscript, agree with its contents, and consent to its publication.
Discussion
Spinal TB, known as Pott’s disease, is regarded as a destructive form of TB, accounting for about half of the osteoarticular TB cases. The sites that are usually involved are the thoracic and lumbar spine. It is a disease of poverty that also affects children in developing countries and has an adverse impact on these children and their families. 9 However, there are limited reports concerning pediatric spinal TB. Children with great susceptibility are both anatomically and physiologically different from adults. Pediatric mycobacterium which also results in bone loss mainly causes damage to the vertebral body. The anterior growth potential is disturbed. The posterior growth potential remains normal. Kyphosis and gibbus can occur in conjunction with spinal growth during a child’s rapid growth and development period. With an increasingly unstable spine, the spinal cord and nerve root will be compressed and the symptoms such as abnormal sensation, staggering, and paralysis are produced. Early diagnosis and effective treatment can minimize sequelae and improve clinical outcomes; however, spinal TB is still a great challenge to physicians because of the nonspecific and wide spectrum of clinical presentations. 10 The children have immature immune systems combined with poor nutrition, so the TB poisoning symptom is not typical and children merely present with comorbid night crying, growth retardation, and/or anorexia, so that it is easy to overlook the actual cause of these signs and symptoms. Anti-TB chemotherapy remains the cornerstone for management of childhood spinal TB, yet it cannot effectively prevent the progression of kyphosis. Adult spinal TB, which is treated conservatively, has a mean 15° increase in kyphosis, and 5% of these patients eventually develop over a 60° deformity. 11,12 The risk for children is even higher with severe deformities of >90° in 10% of patients. Kyphosis may proceed to increase even after healing of the tubercular disease. 13 It has been reported that children’s deformities could be corrected spontaneously during the growth spurt if the apophyseal ring cartilage and end plate still existed. In addition, the altered biomechanics could affect the children’s deformed spine morphology. 3,14 –16
Surgical treatment aims for decompression, debridement, and fusion. Limited indication for the surgical interventions after adequate conservative treatment (bed rest, anti-TB chemotherapy) includes several factors: (1) formation of numerous cold abscesses and large sequestra, (2) spinal stenosis because of the sequestra or the abscesses, (3) spinal instability or the severe deformities, and/or (4) the onset or progression of significant neurological deficits. A detailed and carefully prepared preoperative program can improve the success rate of surgery and reduce complications. If the abscess is easy to puncture and drainage, we can also treat the children with percutaneous catheter drainage. During drainage, the catheters are irrigated with small doses of saline solution (20 ml) containing isoniazid (0.2 g).
The therapeutic purpose of pediatric spinal surgery is to remove the focus, decompress nerves, correct the spinal deformity, and help to retain spinal stability with full consideration of the growth characteristics and unique anatomical characteristics of children. Many operative approaches have been adopted in childhood spinal TB, but to our knowledge, few studies in the literature on the use of posterior debridement, internal fixation, and interbody fusion using shaped titanium mesh cages for the surgical treatment of spinal TB in pediatric patients have been reported. Since the lesions are located in the vertebral bodies, the anterior approach has been recommended by some scholars. The anterior approach gives direct and wide access to the diseased area. Through this approach, it is possible to remove all pathological foci and to make an accurate diagnosis. 17 Rajasekaran and Soundarapandian studied 81 patients for 8 years and found that the anterior arthrodesis could not prevent the long-term progression of the kyphosis in the long time. 18 Schulitz reported the anterior approach destroyed the anterior growth and limited the capacity for spinal remodeling. 19 Progressive kyphosis from posterior element overgrowth was an initial concern regarding children with spinal TB who underwent anterior fusion. 20 Some surgeons then suggested that an additional posterior fusion in one or two stages could be applied to correct kyphotic deformity and prevent correction loss and graft failure. 21,22 However, this approach did not prove to be successful in treating the kyphosis as reported by some studies. 17,20 An additional posterior intervention was then applied in the combined approach. 4,6 This combined approach, however, has the disadvantage of longer operating times, more blood loss, longer healing periods, and more extensive surgical trauma for the children. In this study, we adopted a posterior debridement, internal fixation, and interbody fusion using shaped titanium mesh cages. With a minimum amount of trauma during treatment, it is the purpose of the current international trend in surgical developments for the treatment of this disease, especially with regard to children. This approach is an effective and safe therapy which has been indicated in adult by the mid-term follow-up. 23 –25 It avoids complex anatomical structures in the abdominal or thoracic cavities and reduces the possibility of large vessels and vital organs injuries. Through only one incision in the posterior spine, we can remove the focus and abscess as completely as possible on or around the vertebral body at a 270° angle under direct visualization without the injury to the spinal cord. Complete, in this situation, is a relative, not an absolute concept. The range of debridement range includes dead bone and abscess, necrotic, and granulated tissues. Concurrently, the kyphosis can be corrected by using a suitable pedicle screw in order to keep healthy bone tissue as much as possible and fix segments as short as possible in order to avoid interference with the spinal growth. Neurological functions of 18 children had significantly improved at their last visits. No dissemination of TB or TB-associated meningitis occurred in our study. This approach partially destroys the posterior column and some are worried about that it may cause iatrogenic spinal instability. However, no implant or fusion failures occurred in our study. This appears to be due to several reasons: (1) the strong suitable pedicle screw, (2) adequate bone grafts (the shaped titanium mesh cage and posterior bone graft), and (3) strict operative indication (less than two vertebral body affection with small paravertebral abscess).
Various kinds of graft materials such as autogenous rib, iliac crest, and allograft have been used for interbody fusion. Some researchers once argued against the use of metal materials because of the adherence of Staphylococcus epidermidis to orthopedic biomaterials and the possibility of bacterial infection. 26,27 Autogenous bone grafting is considered as the standard in bone defect management. For children, the source of the autogenous bone is limited; the graft can also fail because of future slippage, fracture, absorption, or subsidence. Recently, several researchers have confirmed the safety of titanium cages for the treatment of vertebral osteomyelitis. 28 –30 In this study, we used shaped titanium mesh cages filled with autogenous bone and allogeneic bone (if necessary) and obtained satisfactory results. Bone fusion was seen in all cases, and no looseness, displacement, dislocation, or subsidence of the bone grafts were found. The use of shaped titanium mesh cage has several benefits over other bone struts. The shaped titanium mesh cages with their bearing strength play a vital and rigid supporting role in combination with the pedicle screw. We can implant the shaped titanium mesh cage to ensure that the enough contact area between the surface of bone grove and bone graft area is achieved in order to avoid the subsidence of the titanium mesh cage and satisfy the requirements for bone fusion. The device reduces the trauma and complications caused by autogenous iliac bone and resolves the problem of the bone graft absorption in the long term. What is more important, the titanium mesh cages can be shaped based on the intraoperative conditions and can thus meet the needs of individualization treatment. In our study, the shaped titanium mesh cage anteriorly has no negative influence on the course of infection healing, and additionally, it stabilizes the affected segment with valid support.
There are a few limitations in the preliminary study. First, the follow-up time is short especially for the children with bone growth potential. We recommend the frequent follow-ups till skeletal maturity is reached. Second, a large and randomized sample size is needed to elucidate the benefits and risks of the method. The data here may serve as a preliminary evidence that debridement, internal fixation, and reconstruction using shaped titanium mesh cage via a posterior-only approach are a minimally invasive, safe, effective surgical treatment for spinal TB in children.
Footnotes
Authors’ contribution
Hongqi Zhang is the principal investigator of this trial. Qiang Guo, Chaofeng Guo, and Mingxing Tang were responsible for the recruitment and treatment of patients.
Qiang Guo and Yunjia Wang contributed to the drafting of the manuscript; Mingxing Tang, Chaofeng Guo, and Hongqi Zhang edited the final manuscript. Qiang Guo and Yunjia Wang were involved in analysis and interpretation of data. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81401818). The supporting organizations were not involved in the collection of data, analysis, interpretation, or drafting of the manuscript.