
Abstract
Purpose:
A stiff total knee replacement can severely limit a patient’s post-operative function, but there remain few prospective trials identifying those patients at risk, nor the efficacy of manipulation. We analysed our prospectively collected database to assess predictors of stiffness and outcomes following manipulation.
Methods:
Using prospectively collected knee arthroplasty data, including preoperative and post-operative range of knee movement, SF-12 (physical and mental) and The Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores, patients requiring manipulation were compared to a matched group of patients not requiring manipulation, with a detailed statistical analysis undertaken to assess potential risk factors and the post-manipulation outcome.
Results:
Of the 1313 arthroplasty patients, 69 required manipulation. Patients with less than 80° of flexion at discharge, diabetes or on warfarin were more likely to require manipulation, but flexion at discharge was the overwhelming predictive factor for stiffness. Forty per cent of the range of movement gained during manipulation was maintained at 1 year, with earlier manipulation deriving greater improvements. While the WOMAC scores improved post-manipulation, there was no significant difference in either of the SF12 scores.
Conclusion:
Flexion at discharge is the overwhelming predictive factor for the requirement for manipulation.
Introduction
Patient satisfaction following primary total knee replacement can be affected by numerous factors, including reduced post-operative range of movement in the knee which may compromise function and activities of daily living. Studies have shown that 83° of flexion is required for stair climbing, 93° to rise from a seated position without using arms to push and 106° for shoelace tying. 1
As there is no single cause, it can be difficult to predict which patients will be affected by stiffness following arthroplasty; however, a variety of factors have been attributed to or predispose to arthrofibrosis including poor movement both preoperatively and intraoperatively, 2 –6 intraoperative technical problems, 4,7,8 obesity, 9 extreme preoperative varus or valgus alignment, 10 poor patient rehabilitation post-surgery, 7,8,11 diabetes 12 and warfarin therapy 13 Many are therefore labelled as ‘idiopathic stiffness’. 5,7,11 As stiffness is a ‘negative’ outcome, it is unclear until it is clinically evident and indeed subjective in its definition; hence, it is difficult to perform a true prospective study. However, robust prospectively collected outcome data allow a retrospective review once those who have post-operative stiffness are identified and offer a control group to which to compare.
The definition of what constitutes stiffness remains controversial, resulting in a range of prevalence. 9,11,12,14,15 An arbitrary maximum flexion of less than 90°, a lesser value of less than 75° or a certain percentage of the preoperative range of movement have all been proposed. However, these are to some extent unsatisfactory, as there is significant variability in functional requirements among patients. An active individual with preoperative flexion of 130° may feel stiff if they lose 10° post-operatively although they still have a range of movement greater than that which is required for activities of daily living. A patient with a long-standing maximum flexion of 90° may not feel stiff if they lose 10°, even though they have lost a greater percentage of their preoperative movement. The focus in the literature tends to be on the range of movement, but this does not take into account the patient’s function or the psychological effect on them. Therefore, the purpose of this study was to assess the functional outcome of manipulation in patients after knee replacement and to investigate potential predictive factors for stiffness 12,13 using prospectively collected outcome data and a comparison control group. Our null hypothesis was that there were no predictive factors for the requirement of manipulation for stiffness after total knee replacement.
Materials and methods
A database has been prospectively populated on all knee replacements in the senior authors’ institution since 2003, to include standard demographic data, goniometer measured preoperative and post-operative range of movement, detailed preoperative medical history, medications, preoperative and post-operative outcome scores (SF12 physical, SF12 mental and WOMAC) and any post-operative complications. We assessed 1313 consecutive cemented cruciate retaining Profix® Total Knee Replacements (Smith and Nephew, Memphis, Tennessee, USA), performed using a standard trivector approach, either by the two senior authors themselves or under their direct supervision and under spinal or general anaesthesia. None had the patella resurfaced at primary surgery. All patients had full extension at the end of the procedure and flexion to at least their preoperative range. A standard intra-articular analgesic cocktail of 20 ml, 0.5% chirocaine plus 5 ml 1 in 10,000 adrenaline and diluted to 150 ml with normal saline was injected into all layers of the knee towards the end of the procedure. Post-operatively patients had varying analgesic regimens depending on their needs including Patient-Controlled Analgesia (PCA), intravenous and oral medications prescribed by the anaesthetist. Post-operatively patients were entered into our physiotherapy protocol of early active and passive mobilization. Thromboprophylaxis was with Thrombo-Embolic Deterrent (TED) stockings only according to hospital protocol at that time. Patients with significant previous thromboembolic disease or with a high-risk thrombotic tendency were warfarinized post-operatively following preoperative consultation with the haematology department. Patients on warfarin preoperatively had it stopped 5 days prior to surgery with bridging therapy of subcutaneous heparin, warfarin was restarted on day 1 and heparin was continued until the international normalized ratio reached the required target range.
Patients underwent standard assessments preoperatively, at the time of discharge, at 3 months and 1 year. Patients who required manipulation also had the assessment recorded at the time of admission, which was at a variable time post-operatively and had further regular post-operative reviews.
Decision to undergo manipulation was made jointly between the consultant and the patient based on a pragmatic philosophy of symptoms, functional requirements and clinical examination. No formal degree of flexion was used, rather patients offered manipulation if clinically indicated for their needs and hence was subjective in nature but represented what patients required rather than what surgeons felt they required. The manipulation was performed under general anaesthesia with a standard technique – manipulation into extension was performed with the hip in extension on all patients with any loss of extension; and manipulation into flexion with the hip at 90° of flexion. As much movement as possible was gained, and all of the patients were commenced on a standard physiotherapy regime starting on the day of manipulation involving active and passive mobilization and 24 h of continuous passive motion therapy.
From the database, we identified all patients who had undergone manipulation and assessed them in a nested case–control study design with 1:1 matched samples to assess the relationship between exposure in certain factors and the risk of requiring manipulation after their knee replacement. A nesting model allowed analysis of individual factors while taking into account potential influences from other factors, such as age, although these were minimalized as much as possible with 1:1 matching. Patients who were deemed by the operating surgeon to have infection, significantly malaligned components or loosening were excluded as were those patients who may be defined as stiff by a single angle definition but did not require manipulation due to patient perceived good function. Hence, this left a cohort of 69 patients who felt their knee to be functionally ‘stiff’ for their requirements of daily living. For every patient who was allocated to the manipulation group, a control patient was identified who had had surgery at a similar time by the same surgeon; hence, cases and controls were matched for two important confounding factors, the surgeon who performed the operation and the timing of operation. The median difference in the date of operation within each matched pair was 17 days (interquartile range 62 days), indicating that the confounding effect of time was adequately controlled.
To assess the possible contribution of warfarin to arthrofibrosis and to assess whether any association was due to thromboprophylaxis rather than other medical co-morbidities, patients prescribed statins were identified and analysed separately on the basis that statin prescription is a surrogate marker of vascular and cardiac co-morbidity and that microvascular disease is associated with poor wound healing and maturation problems causing increased scar tissue and stiffness. 16,17 Statins were used over the recorded American Society of Anaesthesiologists (ASA) grading, as the latter indicates general pathology rather than specifically vascular co-morbidities.
Frequencies and percentages were used to summarize and present results for categorical variables with means and standard deviations for continuous variables. Mantel–Haenszel odds ratios were calculated, and McNemar’s exact test used to identify risk factors associated with the requirement of manipulation after a knee replacement. Conditional logistic regression for matched pairs and stepwise model selection process were used to identify factors independently associated with the requirement of manipulation. Wilcoxon’s signed ranks test was used to identify significant differences in the basic knee movement measures between groups at various time points preoperatively and post-operatively. Linear mixed effects modelling was performed to describe how knee movement measurements changed from the time of discharge after arthroplasty until the final follow-up assessment separately for each group and identified factors associated to the patient’s recovery. Stepwise model selection process and the Akaike’s information criterion were used to identify the optimal models. Finally, Wilcoxon’s signed ranks test was used to identify significant differences in critical pain and health outcome measures between groups and within pairs preoperatively and at the final follow-up assessment. The analysis was performed using software R version 3.0.1 18 with all statistical tests were performed at the significance level a = 0.05. The prospective population of the database had been agreed by the hospital under their code of ethics.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. Ethical approval for the database containing patient data obtained locally through the Liverpool Research Trials Centre (ref 1893 and 2060); early data were held on a database in Scotland requiring ethical approval through the Multi-Centre Research Ethics Committee for Scotland (ref MREC/04/10/004), who felt this was audit data and did not require a formal review by the ethics committee.
Informed consent
The individual participants in this study gave consent for their data to be reviewed for scientific assessment.
Results
In the study period, 1313 primary total knee replacements were performed under the care of the two senior authors with 121 patients considered by the operating surgeon to have a degree of post-operative stiffness. Following consultation with the patients concerned, 69 went on to have manipulation (5.3%), of which 1 patient was lost to follow-up. The mean age of this group was 63.78 years (range 43–81 years) with 36 males and 33 females. Forty (59%) patients had a right-sided replacement. There were no complications as a result of manipulation in any patient. The comparison control group contained 69 patients with a mean age of 67.28 years (range 48–86 years), of which 31 (45%) were male and 34 (49%) had a right-sided replacement. The median time to manipulation was 16 weeks. There was no statistically significant age or gender difference between the two groups, although there were significantly less patients of age over 75 years in the manipulation group.
Identifying risk factors for the requirement of manipulation
Table 1 lists that warfarin, diabetes, flexion less than 80° at discharge and a total range of movement less than 60° at the time of discharge was significantly associated with an increased probability of requiring manipulation. Furthermore, the odds of requiring manipulation were significantly decreased when a patient was older than 75 years of age. While the latter may indicate an increased reluctance in undertaking further treatment after knee replacement in older patients, one has to control for this imbalance when analysing these factors in a multivariate setting.
Univariate analysis of potential risk factors associated with the requirement of manipulation.
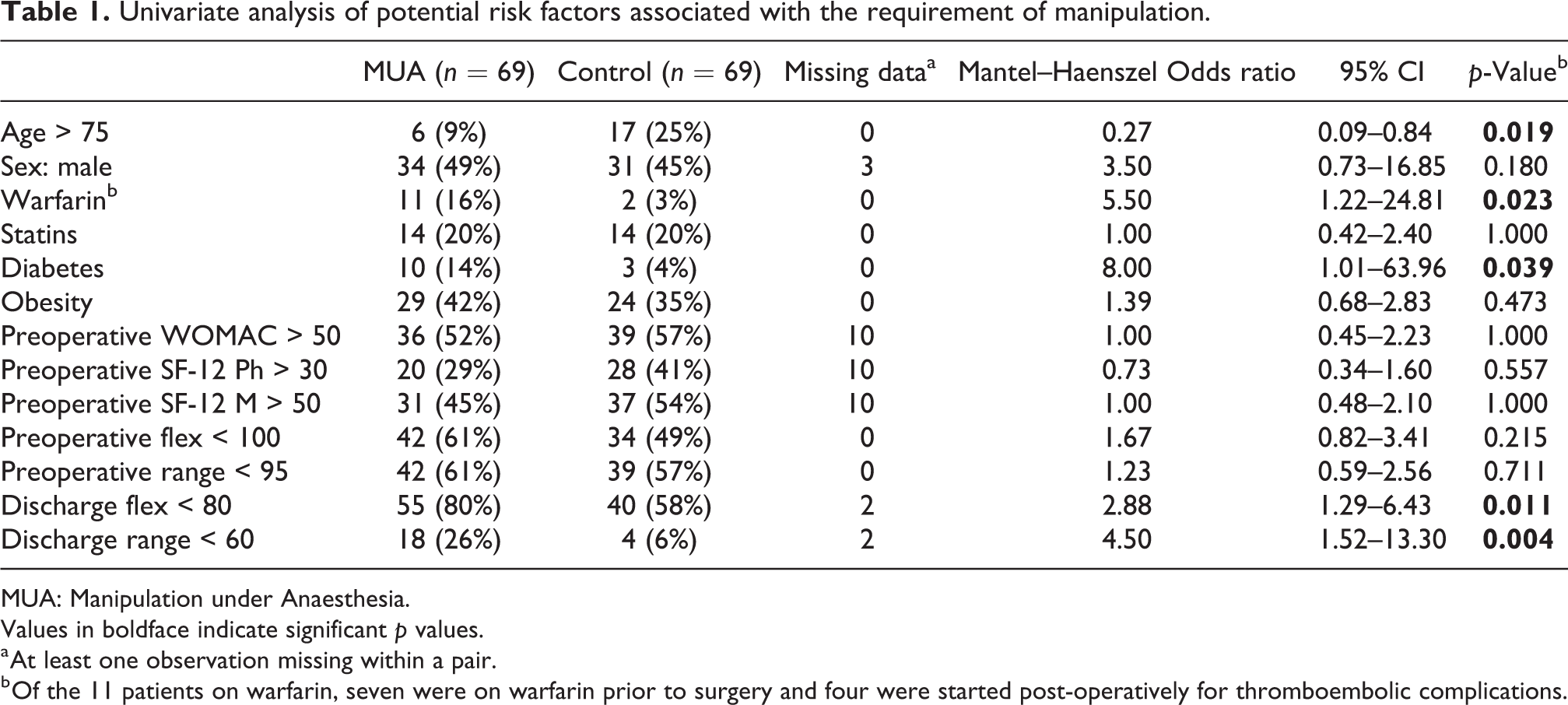
MUA: Manipulation under Anaesthesia.
Values in boldface indicate significant p values.
a At least one observation missing within a pair.
b Of the 11 patients on warfarin, seven were on warfarin prior to surgery and four were started post-operatively for thromboembolic complications.
To assess that these factors were independently associated with the risk of requiring manipulation within a multivariate analysis framework adjusting for the observed age imbalance, conditional logistic regression analysis was used to account for the matched pairs of patients. A stepwise model selection process was used to determine the final model; initially every variable from Table 1 with a p-value of less than 0.05 was added into the model and the non-significant ones (p > 0.05) removed sequentially with age always staying in the model to adjust for the previously observed imbalance.
After adjusting for ‘age’, flexion at the time of discharge was the only significant factor for predicting of requirement of manipulation. Hence, patients who have less than 80° of flexion at the time of discharge are more likely to require manipulation (odds ratio (OR): 3.03) independently of any other factor such as warfarin therapy or diabetes. The last factor that was excluded from the final model was ‘warfarin’ which showed a p-value of 0.072 although the amount of available information regarding to ‘warfarin status’ was very limited as only 11 patients were treated with the drug. The results show that if post-arthroplasty flexion and extension measures are not included in the model, then the presence of warfarin would have been the only independent significant factor (OR: 6.68, 95% CI: 1.33–33.66, p-value: 0.021); however, when these measures are taken into account, flexion at the time of discharge is the dominating factor that carries all the information to predict the requirement for manipulation.
Change of movement measurements over time
Linear mixed-effects models were used to describe how extension, flexion and range of motion changed over time and to assess factors associated with the patient’s recovery. This model was used rather than simple comparisons between groups for various time points because the measurements are highly correlated within patient; a patient who preoperatively measures well for any factor is more likely to be better post-operative (and improve faster) than a patient with a poorer preoperative measure for the same factor.
Table 2 and Figure 1 demonstrate a significant difference between the two groups with regards flexion and range of movement at discharge and thereafter. The same was also true for extension at 3 months and 1-year follow-up. Patients had similar mean values for all outcome measures between the groups preoperatively but they changed dramatically at the first follow-up. It can be seen that for the manipulation group, while the preoperative correction of extension is partly maintained at discharge, this is lost at follow-up and deteriorates to worse than the preoperative level. Although over half of the flexion and range of motion gained after manipulation is lost after 1 year, these measurements are still 20–30% higher when compared to the first follow-up and hence manipulation does improve the flexion (and hence range of movement) of those patients.
Mean (SD) of extension, flexion and range of movement over time.

Values in boldface indicate significant p values.
a Wilcoxon signed ranks test for matched pairs.

Change in flexion, extension and range or movement over time.
Manipulation group
Extension
Patients who have manipulation more than 3 months after a knee replacement experience significantly lower extension levels 3 months after the manipulation and 50% reduction at the 1-year follow-up (Table 3). In addition, there is a strong positive correlation in recovery rates between these two follow-up times (0.67). Therefore, a patient improving substantially at 3 months is very likely to observe further improvement at the 1-year follow-up. Similarly, a patient having lost extension at the first follow-up is very likely to lose extension rather than see any improvement in the later stages of rehabilitation.
Parameter estimates for optimal linear mixed effect models for MUA group.

BMI: body mass index.
Values in boldface indicate significant p values.
a Variables investigated: sex, age, statins, warfarin, BMI, diabetes, preoperative WOMAC score, preoperative movement outcomes and time of MUA.
Flexion
Treatment with statins is associated with some recovery of normal flexion as these patients follow the same declining trend but at a significantly lower rate. On average patients lose 25° of flexion at the first assessment after the manipulation, while patients treated with statins lose 12°. There is some evidence that warfarin is also associated with recovery of normal flexion but this is not very strong due to the small number of patients on the drug. Warfarin is associated with worse short-term recovery rates which fade out by the time of follow-up and that the combination of statins and warfarin produces significantly worse long-term outcomes. There is a very strong positive correlation in recovery rates between the two follow-up time points (0.88).
Range of motion
Flexion is the major contributory component to range of movement; hence, the results are very similar to flexion although the effect of warfarin is slightly stronger while the interaction between warfarin and statins is more evident. The correlation between the two follow-up time points is still very strong (0.85). Overall the patients gain an average of 17° of movement after manipulation compared to their pre-manipulation range of movement, which accounts for 43% of the gain from manipulation; this settles to 40% at 1 year.
Control group
Extension
Statins are associated with recovery but, unlike the manipulation group, patients treated with statins experience a significantly greater loss of extension (Table 4). There is a very strong positive correlation in recovery rates between the two follow-up time points (0.95). There is a strong negative correlation between patients’ starting point and recovery rates until the first follow-up (−0.75); hence, the worse the discharge extension level, the faster the loss of extension at the first follow-up.
Parameter estimates for optimal linear mixed effect models for comparison group.

BMI: body mass index.
Values in boldface indicate significant p values.
a Variables investigated: sex, age, statins, warfarin, BMI, diabetes, preoperative WOMAC score, preoperative movement outcomes and time of MUA.
Flexion and range of motion
There is no significant factor associated with flexion or range of motion recovery rates and there is a very strong positive correlation in recovery rates between the two follow-up time points (0.88 and 0.85, respectively).
Comparing pain and health outcome measures
Figure 2 shows that patients in both groups have similar preoperative scores and there is no change in SF12 mental score neither between groups nor between time points. There is no improvement in SF12 physical score for the manipulation group, but there is a significant improvement in WOMAC score. The control group shows much greater improvement in both scores.
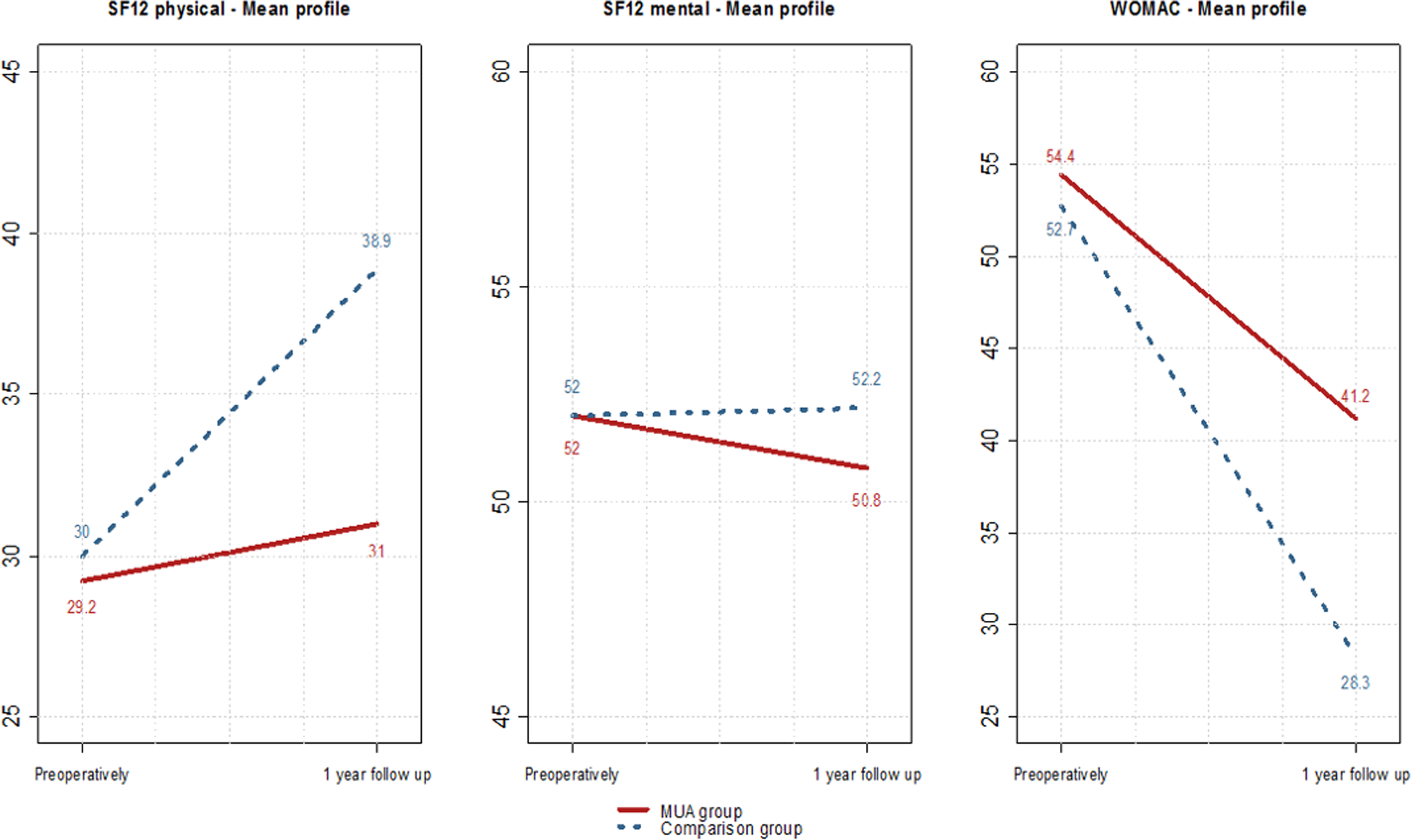
Mean and standard deviation of pain and health scores at different time points separated by group. At 1 year: SF-12 Ph, p < 0.001; SF-12 M, p = 0.531; WOMAC, p = 0.002.
Discussion
There are various treatment options available for the stiff total knee replacement including arthroscopic or open arthrolysis, polyethylene insert downsizing and full revision, with good results documented in the medical literature from manipulation under anaesthesia, with or without additional arthroscopic arthrolysis. 16,19,20 In this study, the manipulation rate of 5.3% was lower than in other studies, which may be related to the indication for such a procedure being based on symptomatology and patient requirement rather than an arbitrary range of movement or degree of flexion.
The results indicate that the need for manipulation can be predicted within a few days of surgery as flexion of less than 80° was the overwhelming statistically significant predictor. At the time of the study, the unit’s mean length of stay was 4.5 days; hence, one can conclude that flexion of less than 80° on day 4 means that manipulation is more likely to be required in the future, suggesting that patients not attaining this level have an early clinic review and potentially more intense physiotherapy though this was not specifically investigated in the study. The literature suggests that the preoperative range of movement is the most accurate predictor of the post-operative range of movement, 2,3,21,22 and the data from this study support this. In addition, we can conclude that even after manipulation patients maintain only 40% of their achieved flexion but don’t regain more movement than the level they had prior to their knee replacement.
There are numerous reported associations with post-operative stiffness including female gender, 7 anticoagulation therapy, 13,23 component malalignment 24 and preoperative patient education. 25 The possible correlation between anticoagulant therapy and arthrofibrosis is hypothesised due to bleeding causing excessive scar tissue, intra-articular adhesions or simply due to difficulty in moving the subsequently painful knee. Keays et al. suggested prophylactic enoxaparin reduces post-operative range of movement in the short term but not the long term 23 and Walton et al. highlighted the relationship between warfarin therapy and the increased need for manipulation following arthroplasty. 13 In our study, 11 patients were treated with warfarin therapy post-operatively – four patients for post-operative deep vein thrombosis and seven patients for preoperative pathology. Although the results support Walton et al.’s findings, statistically this is just outside the significant level, but this may be due to the small number of patients requiring warfarin. Female association with stiffness was not borne out in our data. We did not specifically look at component malalignment and preoperative patient education; the latter of which has been shown to decrease the risk of arthrofibrosis. 25
Patients over 75 years had a significantly reduced risk of requiring manipulation, although this is likely to be, at least in part, related to patient reluctance to undergo further surgery due to lesser functional demands in this age group and an acceptance of less flexion.
While Keating et al. 26 concluded that there was no difference in outcome of manipulation with regard to timing after the initial knee replacement, this finding was not in keeping with the majority of the literature which favours manipulation within 3 months for increasing flexion although not for extension. However, as flexion is the bigger contributor to the range of movement, this measurement also improves with early intervention. 12,15 We agree with Keating et al. showing that timing had no effect on flexion, but earlier manipulation also improved extension.
There are some limitations within this study; we used a symptom-based rather than an arbitrary angle cut-off for manipulation which may have introduced a subjective bias where some with a poorer range of movement did not undergo manipulation, although the arbitrary cut-off also can introduce a different element of bias, with more patients offered manipulation than may require it for their needs. The early improvement in the range of movement following manipulation in this study is similar to the published literature; however, the longer term results are poorer than other studies. Final improvement in the mean range of movement in other studies varies from 32° to 47° with better outcomes with earlier manipulation. 12,15,20,22,26 –28 Our indication for manipulation differs from previous studies, and therefore, our time to manipulation also differed which may explain any differences. This study concludes that patients are likely to maintain 40% of their flexion obtained during the manipulation but not to maintain more than their preoperative flexion level; SF-12 physical scores marginally improve but mental scores do not; however, there was a significant improvement in WOMAC scores suggesting that although the average 40% gain in movement was moderate this represented a functional improvement for the patient.
Footnotes
Acknowledgements
The authors would like to thank Richard Jackson of the Liverpool Cancer Trials Unit at the University of Liverpool for his help with statistical advice.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Knee fellow at The Royal Liverpool & Broadgreen University Hospitals was financed by Smith and Nephew, and Mr Santini has received speaker honorarium from Smith and Nephew.