
Abstract
Purpose:
To investigate the association between body mass index (BMI) and perioperative complications until hospital discharge, following primary total knee arthroplasty (TKA).
Methods:
This retrospective study reviewed 1665 cases of elective primary unilateral TKA performed between 2006 and 2010, from a prospective secure electronic database. Types of complications, length of operating time, and duration of hospital stay were analyzed in both adjusted (for known confounders) and unadjusted analyses. A further matched analysis was also performed.
Results:
In terms of overall complications, there was no statistically significant difference between the BMI categories. When individual obesity category was considered, obese 2 had the lowest odds of developing complications, both with unadjusted (odds ratio (OR): 0.61, 95% confidence interval (CI) 0.41–0.91, p < 0.015) and adjusted regression analysis (OR: 0.65, 95% CI: 0.43–0.99, p = 0.044). Compared to normal weight category, obese class 3 (≥40 kg/m2) individuals were at 66% (OR: 0.34, 95% CI: 0.21–0.55) lower (unadjusted) odds of developing cardiac complications (overall p < 0.001). With the matched analysis, compared to normal weight category, obese class 3 (≥40 kg/m2) individuals were at a 60% (OR: 0.40, 95% CI: 0.23–0.68) lower (unadjusted) odds of developing cardiac complications (overall p = 0.004). Obese 3 patients had significantly higher operating time compared with other groups (p < 0.001).
Conclusion:
This study did not find a significant association between BMI and increased overall in-hospital medical or surgical complications following primary TKA. Obesity significantly increased the length of operating time.
Introduction
Obesity has been one of the major public health issues that seem to have evolved into a global crisis. According to projections, based on current rates of weight gain, the prevalence of obesity will increase to 34% by 2025 in Australia. 1 Many obese individuals are in need for lower limb joint arthroplasty due to the higher likelihood of developing osteoarthritis. 2 Operating on individuals with a higher body mass index (BMI) is challenging to the surgeons because of the complexity of the procedure, increased risk of perioperative complications, and issues with patient recovery in the long term. 3
The influence of obesity on the occurrence of postoperative complications following total knee arthroplasty (TKA) remains controversial. 4 Moreover, there is paucity of evidence in the in-hospital complications and their association with obesity categories in this cohort of patients. Some studies have evaluated long-term postoperative complications following TKA, 5 –7 while others have investigated functional recovery and wound complications. 8 Another study that assessed in-hospital complications following TKA classified all those with a BMI ≥ 30 kg/m2 into one category. 9 Due to potentially different risk profiles of various BMI categories and the concept of paradoxical survival benefit in high BMI individuals, it becomes essential to analyze the likelihood of complications with different classes of obesity. The purpose of this study was to investigate the association between different categories of BMI and the postoperative adverse outcomes in patients undergoing primary TKA during their hospital stay.
Materials and methods
The Prince Charles Hospital (TPCH) is a tertiary referral hospital in Brisbane, Australia. The TPCH Department of Orthopaedics Joint Replacement Programme provides in excess of 500 elective major joint replacement procedures each year. Following institutional ethics approval (HREC/13/QPCH/76), this retrospective study reviewed all cases of elective primary TKA performed between January 1, 2006, and December 31, 2010, inclusive from a prospective secure electronic database maintained by the Department of Orthopaedics. Revision knee surgery and bilateral knee arthroplasty were excluded. The database provided information on the patients’ demographics, surgical details, and any documented complications during postoperative follow-up.
Initially from the list of included patients, a small group of patients (n = 50) were randomly selected for a feasibility study to assess the validity of data collection as well as to cross verify the accuracy of the database with the patient records. This limited pilot demonstrated that patient data were sufficiently intact and available for investigation. Subsequently in addition to the data from the database, the study team, consisting of trained medical officers, medical students, and a senior anesthetist, sequentially accessed patient records and reviewed the operation reports, preadmission and anesthetic records, inpatient medical records, and discharge summaries to extract data to find out whether there was missing or inadequate information. Patients were grouped according to their BMI with the World Health Organization obesity classification system into the following categories: underweight (<18.50 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), obese class 1 (30–34.9 kg/m2), obese class 2 (35–39.9 kg/m2), and obese class 3 (≥40 kg/m2). 10 From a prospective list of complications, outcomes of interest were identified and categorized into system-based complications (Table 1).
List of complications included under each category.

Statistical analysis
Statistical analyses were performed by a biostatistician (SLW) using SPSS for Windows (version 23, IBM Corp. Version 23.0, Armonk, NY.). Data were tested for normality and presented as means (standard deviation) or medians (interquartile range (IQR)) calculated accordingly, with appropriate testing performed. Frequencies were compared using the χ 2 test or Fisher’s exact test as appropriate. Unadjusted and adjusted logistic regression analyses were performed and odds ratios (ORs) with 95% confidence intervals (CIs) presented. Following the analysis of the primary end point (overall complications), different complication subtypes were examined to identify whether there was a more specific relationship with the individual complications (cardiac, surgical, pulmonary, renal, neurological, thromboembolic, infectious, or gastrointestinal). Adjustment was made in the regression analysis for the known confounders: age, gender, comorbidity defined by American Society of Anesthesiologists (ASA) classification, underlying pathology necessitating surgery, and the type of anesthesia. Due to the statistically significant differences in age and gender between the BMI categories, additional analysis was performed to further control these confounders; each normal weight control was matched by age and gender (blinded to other variables), with one case from each of the higher BMI categories, resulting in 141 normal weight cases matched with 141 in each BMI group.
Results
Patient characteristics
There were 1665 primary TKA performed during the study period: 141 patients (8.5%) were of normal weight, 481 (28.9%) were overweight, 508 (30.5%) belonged to class 1 obesity, 320 (19.2%) belonged to class 2 obesity, and 213 (12.8%) belonged to class 3 obesity. There were 2 (0.1%) patients who were underweight (BMI < 18.5 kg/m2). The demographics of the cohort are presented in Table 2. The median age of the patients undergoing TKA at the time of their primary operation was 69 years (IQR 13, range 36–92). Majority of the patients belonged to ASA 2 category (57.1%, n = 951) and were females (61.9%, n = 1030). Osteoarthritis (98.3%, n = 1637) was the most common reason for undergoing TKA. Overall, the median patient BMI was 31.7 kg/m2 (IQR 8.4, range 17.7–62.1). Obese 3 and underweight patients were significantly younger than the rest of the BMI categories (p < 0.001). Gender differences between the groups were also significant (p < 0.001). No significant differences were noted between the BMI categories with respect to the listed medical comorbidities.
Demographic details of the patients who underwent primary TKA during 2006–2010 (n = 1665).

TKA: total knee arthroplasty; IQR: interquartile range; ASA: American Society of Anesthesiologists; OA: osteoarthritis.
a Statistically significant.
Occurrence of complications
The outcomes included both major and minor complications. Due to the small number (2, 0.1%) of underweight patients, these cases were excluded from further analyses. There was no in-hospital mortality. There was no statistically significant difference between the BMI categories in terms of overall complications, both with χ 2 test (p = 0.114, Table 3) and with unadjusted regression analysis (p = 0.065, Table 4). Although when individual BMI categories were considered, it was observed that obese 2 had the lowest odds of overall complications, both with unadjusted (OR: 0.61, 95% CI 0.41–0.91, p < 0.015) and with adjusted regression analysis (OR: 0.65, 95% CI: 0.43–0.99, p = 0.044) (Tables 4 and 5). On the other hand, when various categories of systemic complications were subsequently investigated using unadjusted regression analysis, it was observed that the risk for developing cardiac complications progressively and significantly decreased with an increase in BMI. Compared to normal weight category, obese 1, obese 2, and obese 3 individuals were at 36% (95% CI: 0.43–0.94), 49% (95% CI: 0.33–0.78), and 66% (95% CI: 0.21–0.55) lower odds of developing cardiac complications, respectively (overall p < 0.001). Additionally, obese 3 category had significantly decreased odds of gastrointestinal complications (OR: 0.23, 95% CI: 0.07–0.73, p = 0.01). Overall, BMI significantly influenced the likelihood of cardiac (p < 0.001), neurological (p = 0.04), and gastrointestinal (p = 0.01) (Table 4) complications in the unadjusted analyses.
Overall complications, length of stay, and operating time.

IQR: interquartile range.
a Statistically significant.
Results of unadjusted regression analysis of overall and specific postoperative outcomes following TKA by BMI category expressed as ORs with 95% CIs (underweight category excluded).

TKA: total knee arthroplasty; OR: odds ratio; CI: confidence interval.
a Statistically significant.
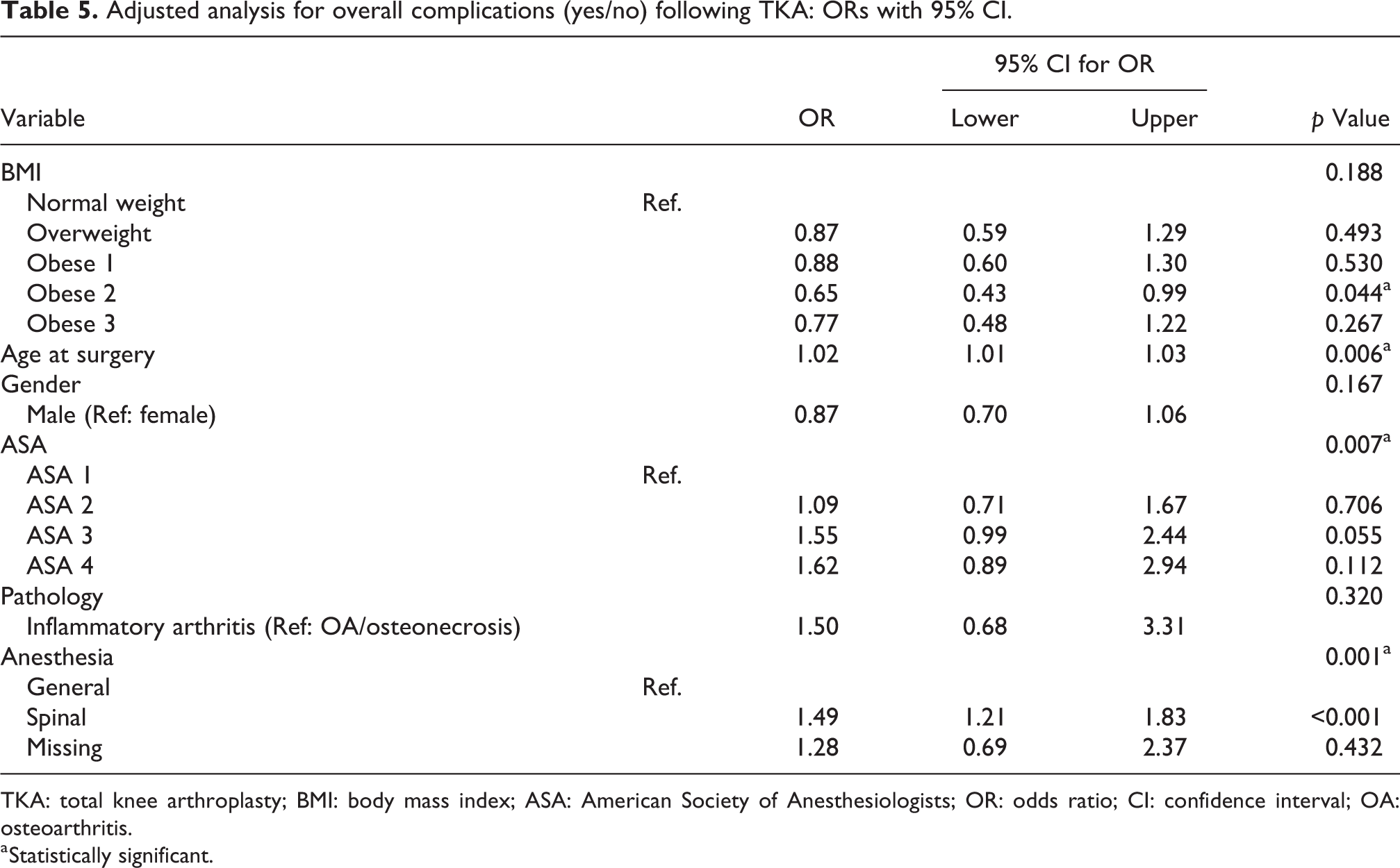
Adjusted analysis for overall complications (yes/no) following TKA: ORs with 95% CI.
TKA: total knee arthroplasty; BMI: body mass index; ASA: American Society of Anesthesiologists; OR: odds ratio; CI: confidence interval; OA: osteoarthritis.
a Statistically significant.
Using adjusted logistic regression for the presence of complications, adjusted for known confounders, it was noted that age at surgery, ASA category, and type of anesthesia were significant predictors of complications (p = 0.006, p = 0.007, and p = 0.001, respectively) (Table 5). Patients who underwent spinal anesthesia had 49% (OR: 1.49, 95% CI: 1.21–1.83, p < 0.001) higher odds of complications than who had general anesthesia.
With the further analysis of the matched data, it was observed that 54 patients (38.3%) in the normal weight group developed cardiac complications compared with 54 (38.3%) in pre-obesity, 40 (28.4%) in obese 1, 45 (31.9%) in obese 2, and 28 (19.9%) in obese 3 groups. Unadjusted regression for this matched analysis also resulted in a statistically significant difference between BMI categories in terms of cardiac complications (p = 0.004), but only obese 3 category had significantly reduced odds compared to normal weight category (OR: 0.40, 95% CI: 0.23–0.68, p = 0.001) (Table 6). Neurological and gastrointestinal complications were no longer significantly different between BMI categories. From the adjusted logistic regression analysis of the matched data set for overall complications (Table 7), it was noted that the only significant predictor of overall complications was the type of anesthesia (p = 0.01). However, adjusted logistic regression of the matched data set for cardiac complications indicated that BMI category was also significant in the model (p = 0.026) with the obese 3 group having significantly lower odds of developing cardiac complications than the normal weight group (OR: 0.45, 95% CI: 0.25–0.81, p = 0.008) (data not shown but available on request).
Results of unadjusted regression analysis of matched data with overall and specific postoperative outcomes following TKA by BMI category expressed as ORs with 95% CIs (underweight category excluded).

a Statistically significant at 5% level.
Adjusted analysis for matched data for overall complications (yes/no) following TKA: ORs with 95% CIs.

TKA: total knee arthroplasty; BMI: body mass index; ASA: American Society of Anesthesiologists; OR: odds ratio; CI: confidence interval; OA: osteoarthritis.
a Statistically significant at 5% level.
Length of stay and operating time
Although there was no difference in length of stay between the BMI categories, there was a significant influence of BMI upon operating times. Operating times increased with increasing BMI. Obese 3 patients had significantly higher operating time compared with other groups (p < 0.001) (Table 3).
Discussion
Our analysis of 1665 patients who underwent primary TKA at our center demonstrates that overweight or obese patients are not at higher odds than normal weight patients of developing perioperative complications during their hospital stay. In fact, adjusted analysis demonstrated that the odds of obese 2 developing complications were 35% lower (p = 0.044) than the normal weight category. Our primary finding is consistent with an earlier study with a similar sample size to our study, 11 although those patients were followed up for 30 days. However, when age- and gender-matched analysis was performed, the reduced odds with obese 2 category was no longer observed, suggesting that age and gender influence overall complication rates rather than BMI.
In terms of cardiac complications, with unadjusted analysis, we observed that there was a significant difference between obesity categories. In addition, when compared with the normal weight individuals, those in obese 3 category, in particular, were at lower odds of cardiac complications. This situation persisted even after age- and gender-matched analysis. Paradoxical situation of better survival outcomes in high BMI groups has been extensively reported in cardiac failure 12,13 and other medical conditions. 14 –16 For instance, in a previous study, cardiac complications were found to be higher in patients with metabolic syndrome undergoing TKA compared to those without metabolic syndrome. 17 It is possible that these controversial findings could be the result of low discriminatory power of BMI or obesity being investigated as an isolated factor and not along with its coexistent metabolic disorders, 18 –20 and therefore, these results should be interpreted with caution.
We observed that as the BMI increased, median age at surgery of our cohort of patients progressively decreased. Underweight and obese 3 patients underwent knee arthroplasty at a significantly younger age than other patients. Although the underweight category is not well represented to make any firm conclusions, our observation of the obese cohort being younger seems to support the previous evidence on the risk of degenerative osteoarthritis with increasing BMI. 21 –23 Since age was found to be a significant predictor of complications (Table 5), we also propose that the lower age-group and possibly more intensive intraoperative monitoring in the obese patients could have played a protective role. It is possible that patients with high BMI were allocated high ASA scoring by anesthetists, and the choice of anesthesia may have been influenced by the high BMI of the patients.
Even though there are reports on obese patients being at a higher risk of thromboembolic complications, 24,25 we did not observe any significant increase in risk with increasing BMI. Majority of patients in our center receive routine aspirin thromboprophylaxis for 6 weeks along with compression stockings. Our findings are consistent with an earlier study that did not find any association between in-hospital thromboembolic complications and the presence of metabolic syndrome. 17
There was a progressive increase in the surgical time along with an increase in BMI as reported in some of the earlier studies. 9,21 Liabaud et al 21 in their study on 273 patients, had demonstrated that an increase in BMI of 1 kg/m2 increased the surgical time by 0.93 min. However, they had also shown an increased occurrence of surgical complications such as wound healing issues and arthrofibrosis requiring intervention. We did not observe any such increase in wound complications with increasing BMI. Increase in operating time in obese patients due to anticipated technical difficulties could be minimized by specialized experience in operating on high BMI groups. 26
Our study has some strengths and limitations. Our sample size is large enough to draw some robust conclusions with regression analysis. However, being a retrospective study, it is subject to limitations such as biases due to selection of patients and the choice of anesthesia based on their comorbidities, missing data, measurement bias, and errors in data entry. However, these data have been procured from a large, prospective, hospital-based orthopedic database, and postoperative outcomes have been predefined, thus limiting classification bias. Although there are possibilities of errors due to ICD-9-CM coding, follow-ups had been performed routinely by the orthopedic team until discharge and complications had been identified for the databases. Some entries such as ASA classification had been retrospectively allocated by one of the investigators (an anesthetist) based on the documented clinical comorbidities, where ASA grades were not available. Although this may have resulted in some misclassification bias, our results showing increasing odds of complications with increasing ASA category seem logical, thus making it unlikely. We had not included simultaneous or sequential bilateral or revision knee arthroplasty and only included complications that occurred before discharge. Certain categories were merged to facilitate simple statistical analysis. Since the underweight category had only two patients, we could not draw any conclusion on the effect of a low BMI.
Conclusion
In summary, this study did not find a significant association between BMI and increased in-hospital medical or surgical complications following primary TKA. Obesity significantly increased the length of operating time. We support the view that patients should not be denied a useful procedure such as TKA on the basis of high BMI alone. However, we recommend a large-scale prospective study to assess the impact of obesity along with the presence of coexisting metabolic disorders on the complications following TKA.
Footnotes
Authors’ note
Upon author’s discretion, the research data and analysis results can be made available on request.
Acknowledgments
The authors would like to thank Louise Tuppin, data manager in the Orthopaedic Research and Data Management Unit at the Prince Charles Hospital, for providing data for this project.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RWC is the principal investigator of projects supported by Stryker Orthopaedics and has received royalties from Stryker Corporation. SLW is employed with part support via external institution by Stryker Australia and Stryker EU. Other authors did not report any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.