
Abstract
Background
The purpose of this study was to determine whether high BMI affect short-term clinical and radiologic outcomes of robotic-assisted total knee arthroplasty (TKA) by comparing the clinical outcomes, radiologic outcomes and complications between high BMI and normal patients.
Methods
We retrospectively compared the short-term clinical and radiological outcomes of 424 knees (408 patients). The patients were divided into four groups: BMI < 24.9 kg/m2 (normal); BMI between 25.0 and 29.9 kg/m2 (overweight); BMI between 30.0 and 34.9 kg/m2 (obese class I) and BMI between 35.0 and 39.9 kg/m2 (obese class II). Clinical and radiologic outcomes were evaluated.
Results
There was no significant difference in radiologic outcomes between those groups (p > .05). Furthermore, there was no significant difference in operation time, drainage volume, fall in hemoglobin, post-operative CRP and complications, including periprosthetic fracture and periprosthetic joint infection (PJI), between those groups.
Conclusion
High BMI does not affect short-term clinical and radiologic outcomes in robot-assisted TKA.
Introduction
The mechanical axis of the lower limb and component position after total knee arthroplasty (TKA) are crucial factors for determining the long-term survival of the implant.1,2 Accurate implant positioning, balanced flexion-extension gaps and appropriate ligament tensioning can decrease the rate of polyethylene wear and thus minimize the need for revision arthroplasty.3,4 Robotic-assisted arthroplasty is a widely used technique to improve implantation accuracy. Although it remains controversial whether this technique can provide better long-term outcomes to patients, several studies have confirmed that robotic-assisted TKA can improve the accuracy of implantation and mechanical alignment.5–9
A significant number of patients undergoing robotic-assisted TKA are high BMI or even morbidly high BMI. Several studies have reported that high BMI can substantially affect the results of TKA.10–14 The rate of revision arthroplasty is significantly high in high BMI patients with poor prosthetic component positioning. 15 It is difficult to achieve the optimal mechanical axis of the lower limb and implant positioning in high BMI patients because of obstruction of bony landmarks by the substantial amount of adipose tissue, restricted surgical visibility, and reduced flexion due to soft-tissue constraints. High BMI patients are considered susceptible to some issues such as tibial loosening, wound complications, cardiovascular events, and respiratory complications after TKA, contributing to poorer patient outcomes.16–18 Therefore, some surgeons advocate the use of computer navigation technology to treat these patients. Some studies have reported the use of computer-assisted TKA for mechanical alignment in high BMI patients. 19 However, to the best of our knowledge, it remains unelucidated whether high BMI affects short-term clinical and radiologic outcomes in robotic-assisted TKA.
The present study aimed to determine whether high BMI affect short-term clinical and radiologic outcomes of robotic-assisted TKA by comparing the clinical outcomes, radiologic outcomes (mechanical axis of the lower limb, component position), and complications between high BMI and normal patients.
Methods
Patients
This retrospective study included 408 patients (424 knees) who underwent robotic-assisted TKA in our hospital from January 2021 to January 2023. Inclusion criteria for this study included the following
1
: patients with knee osteoarthritis or rheumatoid arthritis undergoing primary TKA,
2
patient between 18 and 80 years of age,
3
surgery using the robotic-arm assisted technique,
4
varus deformity. The exclusion criteria were as follows
1
: secondary osteoarthritis of the knee,
2
revision TKA or previous open knee surgery,
3
neurological or hematological disorders,
4
those who we were unable to contact or declined follow-up, and
5
morbidly obese and super obese patients (BMI≥40.0 kg/m2). Ethical approval for this study (QYFYEC 2020-017-01) was provided by our hospital and the written informed consent of all patients was obtained. Robotic-assisted TKA was performed by two senior surgeons who had received specialized training in this field. We excluded a total of 16 according to the exclusion criteria. Then, the patients were divided into four groups: BMI < 24.9 kg/m2 (normal); BMI between 25.0 and 29.9 kg/m2 (overweight); BMI between 30.0 and 34.9 kg/m2 (obese class I) and BMI between 35.0 and 39.9 kg/m2 (obese class II). 89 patients (94 knees) in the normal group, 111 patients (117 knees) in the overweight group, 112 patients (114 knees) in the obese class I group and 80 patients (83 knees) in the obese class II group were included in the study (Figure 1). Flowchart of the cohort. pts, patients.
Preoperative planning
All patients underwent TKA assisted by the MAKO robotic interactive orthopaedic arm system (Stryker Corp, Mako Surgical Corp). All patients took standard preoperative radiograph and CT scans. The CT scans were done with a slice space of 1 mm, and the CT data were transmitted to the MAKO planning module. Then, the MAKO Robotic Knee System’s 3D template software was used to preoperative planning in order to achieve optimal bone resection, implantation and limb alignment.
MAKO total knee robotic-assisted surgery
Under general anesthesia, TKA was performed in all patients through the medial parapatellar approach. Tourniquet was used during the operation. After registration pins were inserted, a probe was used to touch the corresponding points on the surface of the femoral condyle and tibial plateau in order to complete the registration. Intraoperative dynamic tracking markers were used to assess the flexion and extension gaps, alignment, and range of motion. Tibial and femoral bone resections were performed perpendicular to the tibial and femoral mechanical axes, respectively. Based on the evaluation of flexion space and range of motion, the femoral component flexion and tibial slope were then adjusted as required. All patients used posterior stabilized (PS) implant (Stryker, Triathlon). Both femoral and tibial components were fixed with bone cement. To reduce perioperative blood loss, all patients received an intravenous infusion of 120 mg/kg epsilon aminocaproic acid (EACA) mixed with 100 mL of normal saline. Following implant placement, 2 g EACA was injected into the joint cavity. All patients were placed with drainage tubes, which were removed the next morning, and the drainage volume was measured.
Postoperative rehabilitation
During the postoperative period, all patients were managed according to the guidelines of Accelerated Rehabilitation of Chinese Hip and Knee Joint Replacement-Expert Consensus on Perioperative Management Strategies to prevent infection of the surgical site, maintain appropriate analgesic use after surgery, and prevent thrombosis. The first physiotherapy session was undertaken at the first day post-operatively. (POD1). Patients underwent a standardized post-operative rehabilitation program with full weight-bearing and active range of movement exercises commenced from day of surgery. Each physiotherapy session lasted 30 min in total and all rehabilitation was performed by the same team in both treatment groups. All patients were discharged from the hospital on the POD4. All patients received a self-controlled analgesia and 50 mg of intravenous Flurbiprofen axetil twice a day. The patients were also administered an intravenous infusion of 1 g cefazolin sodium for prophylactic anti-infective treatment (1 time during surgery and 3 times postoperation). To prevent thrombosis, low-molecular-weight heparin was used after surgery and oral apixaban was given for 2 weeks after discharge.
Clinical assessments
All patients underwent outpatient follow-up at 6 weeks, 3 months, 6 months, 1 and 2 years after the surgery. All patients end the follow-up period in the second year after surgery. Clinical scores, including Knee Society score (KSS pain and function), 20 WOMAC score, 21 and FJS-12 score 22 before the surgery and at the final follow-up were compared between the high BMI and noraml groups. The KSS system is subdivided into a knee score that rates only the knee joint itself and a functional score that rates the patient’s ability to walk and climb stairs. The dual rating system eliminates the problem of declining knee scores associated with patient infirmity. WOMAC is a disease-specific purpose built high performance instrument for evaluative research in osteoarthritis clinical trials. The Forgotten Joint Score is a patient-reported outcome measure validated in assessing patients post knee arthroplasty, anterior cruciate ligament (ACL) reconstruction surgery and patellar dislocation. Blood tests such as Complete Blood Count test, electrolyte test and C-reactive protein test were usually performed on POD2. The operation time (min), postoperative drainage volume (mL), postoperative CRP level (mg/L), and hemoglobin loss (g/L) (difference between preoperative and postoperative hemoglobin levels) were recorded. Periprosthetic fractures and PJI were evaluated based on the review of medical records.
Radiographic assessment
Anteroposterior, lateral, and standing radiographs were acquired preoperatively and at each follow-up. The radiographs obtained at the final follow-up were used to compare the alignment and positions of components. Standing radiographs were used to evaluate the HKA axis and implant position, while anteroposterior and lateral radiographs were used to measure the coronal and sagittal inclinations of the femoral and tibial components (α, β, γ, δ) (Figure 2). Outliers were defined when the measured angle exceeded ±3° from the neutral alignment in each radiological measurements on the final follow-up radiograph. To test the intrarater and interrater reliabilities of the radiographic assessments, all radiographs were measured twice at an interval of 2 weeks (once by a specially trained surgeon and once by a blinded surgeon). The intraclass correlation coefficient (ICC) was >0.8, which indicated good reproducibility.
23
Radiologic measurement of femoral and tibial implants. α, coronal inclination of femoral component, β coronal inclination of tibial component, γ sagittal inclination of femoral component, δ sagittal inclination of tibial component.
Data analyses
The continuous variables were expressed as the mean and standard deviation, or range. Categorical variables were represented by frequency and constituent ratio. The one-way analysis of variance (ANOVA) with Bonferroni post hoc test was used to compare the continuous variables. Chi-square test and Fisher’s exact test was used for categorical variables. p < .05 means the difference is statistically significant. Statistical analysis and graphing were performed using SPSS version 25 (IBM Corporation, Armonk, New York, USA).
Results
Demographic data of patients.
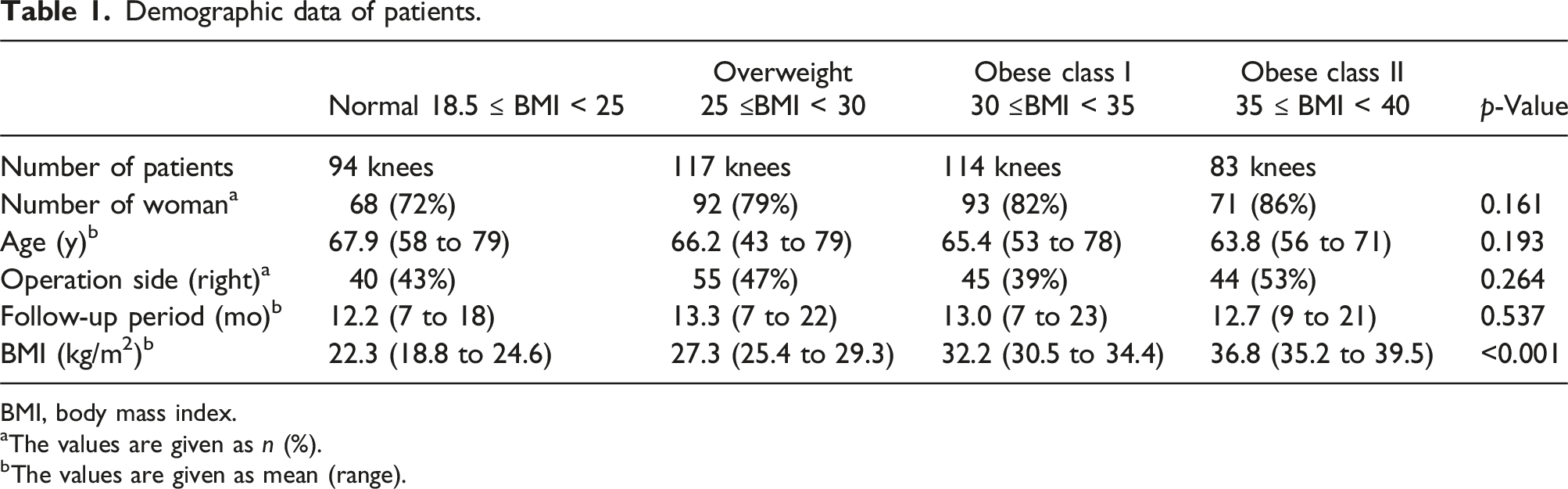
BMI, body mass index.
aThe values are given as n (%).
bThe values are given as mean (range).
Clinical outcomes
Comparison of operative data and clinical results.

BMI, body mass index; CRP, C-reactive protein.
aThe values are given as mean ± standard deviation.
bThe values are given as n (%).
cFisher’s exact test.
Comparison of preoperative and postoperative clinical outcomes.

BMI, body mass index; WOMAC, Western Ontario and MacMasters Universities; FU,follow-up; FJS-12,forgotten joint score.
Radiographic outcomes
Comparison of radiographic results.

BMI, body mass index; HKA, hip-knee-ankle angle; BMI, body mass index.
aThe values are given as mean (range).
bThe values are given as n (%).
Discussion
The present study showed no differences in short-term clinical and radiologic outcomes between high BMI and noraml patients who underwent robot-assisted TKA after a mean 1-year follow-up period. Although the clinical outcomes of the obese class II patients were worse than those of other patients, there were no significant differences.
Several studies have confirmed that high BMI can prolong the operative duration of conventional TKA.24–26 The thick soft tissue envelope in obese patients could make exposure difficult, obscure bony landmarks, and obstruct accurate positioning of cutting guides. 27 These factors may contribute to suboptimal component positioning and increased operative duration. In a retrospective study, Gadinsky et al 24 found that anesthesia induction time, total surgery time, tourniquet time, and wound closure time significantly elevated with increased BMI. The present study showed no significant differences in operation time between the groups. A possible reason for this finding was that robotic-assisted TKA can reduce intraoperative data interpretation and judgment time through precise preoperative planning and intraoperative analysis.
Some researchers found that high BMI was not correlated with increased intraoperative blood loss in TKA. However, the operative time was correlated with increased intraoperative blood loss.28,29 The present study showed no difference in drainage volume and hemoglobin loss between those groups. This conclusion was also supported by other studies, for example, Hrnack et al. 28 examined the effect of BMI, operative time and anesthesia time on total blood loss during primary TKA. The authors found that high BMI was not correlated with increased intraoperative blood loss. Tió et al. 29 reported that severely and morbidly high BMI patients did not show greater blood loss or higher red blood cell (RBC) transfusion needs after primary TKA as compared to non-obese and obese class I patients. This might be because obese class II -III patients had higher estimated blood volume but similar RBC losses.
Several studies have reported that high BMI patients exhibit poorer outcomes after TKA as compared to non-obese patients.30–33 This is because obese patients often have multiple medical comorbidities, such as diabetes mellitus and cardiopulmonary disease, which may negatively affect the results of TKA. 34 In a prospective study, Gage et al. 14 reported that patients with metabolic syndrome were more prone to complications than those without metabolic syndrome. Elevated BMI was the element of metabolic syndrome that showed the largest effect on postoperative complication rates. In another prospective study of 1214 patients, Dowsey et al. 32 observed that high BMI was associated with an increased risk of periprosthetic infection and wound complications. However, in our study, we found that high BMI did not increase the risk of complications after robotic-assisted TKA. This might be because our study did not include morbidly obese (BMI > 40 kg/m2) and super-obese (BMI > 50 kg/m2) patients. 35 Numerous studies have indicated that as the BMI level increases to morbidly and super-obese categories, the complication rates also increase.15,27,29,31,36 Another possible reason for the lower complication rate was that the follow-up time of this study was relatively short, and the long-term complications in the study were not recorded. Hence, long-term follow-up studies should be conducted in the future to confirm our conclusion. In the final follow-up, we observed that the clinical outcomes of the obese class II patients showed worse clinical outcomes as compared to other patients; however, the difference was not significant. Our conclusion was also supported by other studies, Maniar et al. 36 reported that the obese class I (30–34.9 kg/m2) have similar early and late functional recovery as the non-obese patients. However, obese class II (35–39.9 kg/m2) may show less late functional recovery than nonobese patients. Furthermore, obese class III (BMI > 40 kg/m2) have worse functional scores and lower postoperative knee flexion than nonobese patients. McCormick et al 37 analyzed 350 patients (186 Robotic-assisted TKA and 164 conventional TKA) showed that no differences in functional outcomes among patients undergoing Robotic-assisted TKA compared to conventional TKA and high BMI had no significant effect on this association. Unfortunately, our study did not include obese class III patients because of their low proportion. Hence, more studies should be conducted in the future to determine the influence of obese class III (BMI > 40 kg/m2) on short-term clinical and radiologic outcomes of robotic-assisted TKA.
Robotic-assisted TKA has been shown to consistently yield an ideal post-operative mechanical alignment with individualization of the distal femoral resection angle, accurate rotational alignment of the femoral component, accurate machining of bone surfaces with a milling device and maintenance of bone temperature during machining to prevent bone injury. Sires et al. 38 analyzed 45 consecutive cases and calculated the difference between what was planned and what was achieved for bone resection and coronal limb alignment. They found that the accuracy in achieving planned bone resection and final limb coronal alignment using the MAKO robotic arm-assisted technology is high. A prospective cohort study by Li et al. 39 showed that RATKA could accurately predict the component size and execute a preoperative plan to achieve precise bone resection, and implant placement, thereby reducing alignment outliers. But these studies did not distinguish between high BMI and noraml patients. In this study, the prevalence of outliers ranged from 5.3% to 19.7% for all parameters. There was no significant difference in the parameters between the groups. Our results are similar to the findings of Jeon et al (3.6% to 20.2%) and Cho et al (3.5% to 10.6%). The differences may be due to the learning curve of surgeons.
The surgical exposure of high BMI patients was often inadequate because of the presence of the thick soft tissue, which can make bony landmarks inconspicuous and hinder the accurate positioning of cutting guides. This, subsequently, may impact the surgeon’s judgment regarding limb alignment and component position. 27 In a retrospective review conducted by Estes et al. 13 on 196 knees, they revealed that preoperative mechanical limb alignment and BMI significantly influenced postoperative limb alignment following TKA performed with mechanical instruments. Consequently, surgeon express concerns regarding the potential impact of factors such as inadequate visualization and obscured bony landmarks on computer navigation and robotic-assisted surgery based on computed tomography scans of the patient’s knee. However, Kamat et al. 19 analyzed 287 knees in a retrospective study and found that both obese and non-obese patients who underwent computer -navigated TKA achieved good limb alignment. In this study, there was no difference in radiologic short-term outcomes between the groups who underwent robotic-assisted TKA. This finding suggests that high BMI does not affect short-term limb alignment in robotic-assisted TKA. Considering the effect of high BMI on limb alignment after conventional TKA, high BMI patients may be more suitable for robot-assisted TKA than non-obese patients. Additionally, there was no significant difference in operation time between those groups. Therefore, we propose a hypothesize that high BMI patients may be more suitable for robotic-assisted TKA than noraml patients. Further research is required to validate this hypothesis in the future.
The strength of the present was that, to the best of our knowledge, it was the only current study that compared the short-term clinical and radiologic outcomes of robot-assisted TKA between high BMI and noraml patients. We observed no negative effects of high BMI on the short-term clinical and radiologic outcomes of robotic-assisted TKA.
The present study, however, has some limitations. This was a single-center study, which may introduce selection bias. In addition, morbidly obese and super obese patients were excluded because of their low prevalence in Asian populations. Further studies are required to analyze the effect of morbid high BMI on robotic-assisted TKA. Additionally, the follow-up time was short. Because several post-operative complications can occur over a long period of time following surgery, mid- and long-term follow-up studies are required to accurately assess such complications. Besides, we are unable to calculate the sample size because we can’t find any reliable data to calculate it. We could not control for all variables that may influence the clinical and radiologic outcomes in robotic-assisted TKA and lack of some data on confounders and predictors. Finally, posterior-stabilized implant (Stryker, Triathlon) was used in all patients in this study and the conclusions obtained may not be generalizable to other types of implants.
Conclusion
Based on the present study findings, high BMI does not affect short-term clinical and radiologic outcomes in robotic-assisted TKA. Further investigations are required to understand the influence of morbid high BMI and super high BMI on the outcomes of robotic-assisted TKA.
Footnotes
Authors’ contributions
All authors contributed to conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing, review and editing, and visualization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grants from the Shandong Provincial Natural Science Foundation, China [Grant No. ZR2021MH090] and supported by Young Elite Sponsorship Program of Shandong Provincial Medical Association [Grant No. 2023_LC_0267].
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.