
Abstract
Quadriceps tendon rupture after total knee arthroplasty (TKA) is a rare but dire complication. It is associated with adverse outcomes and morbidities. Studies on such complications are scarce in the literature. In this study, we share our experience in the management of four patients who sustained quadriceps tendon rupture in the early postoperative period. Efforts should be focused on prevention. Meticulous surgical techniques during the medial parapatellar approach to preserve the integrity of quadriceps can reduce the risk of rupture. The importance of prompt diagnosis is emphasized as delayed treatment may lead to poor outcomes. However, making a diagnosis can be challenging, as worsening of the quadriceps strength after TKA is expected because of the surgical approach that violates the quadriceps muscle. In an event of postoperative trauma with resultant extensor weakness, an ultrasound evaluation to exclude a quadriceps tendon rupture should be promptly performed after a fracture is excluded.
Introduction
Total knee arthroplasty (TKA) is a well-proven treatment modality that delivers favorable long-term clinical and radiological outcomes for patients with severe osteoarthritis of the knee. 1–2 Precise bone cuts, balancing of soft tissues as well as proper implant placement are the keys to achieving good outcomes. During arthrotomy, it is crucial for surgeons to attain adequate exposure, while maintaining the integrity of the quadriceps tendon, and to ensure that it is amenable to good repair. In situations with inadequate exposure, several surgical techniques such as V-Y quadricepsplasty, quadriceps snip, and tibial tubercle osteotomy were reported in the literature, with good functional outcomes after knee replacement surgery. 3 –6
Postoperative quadriceps tendon rupture remains a potential, albeit rare, complication after TKA and is associated with significant morbidity. 7 –11 Dobbs et al. reported an incidence of 34 cases (0.1%) of quadriceps rupture in a series of 23,800 patients who underwent TKA. Outcomes were reported to be poor for the patients with complete quadriceps rupture with a rerupture rate of 40% postrepair. 10
In this article, we present four cases of post-TKA quadriceps rupture. The main objectives are, firstly, to emphasize the spectrum of presenting signs and symptoms and, secondly, to heighten the awareness and increase the vigilance on this issue among the readers. This is a single-surgeon retrospective study from a tertiary institution. Out of the 913 patients operated over the last 4 years, four patients developed post-TKA quadriceps rupture. All the patients were operated for Kalgren and Lawrance grade 3–4 symptomatic osteoarthritis of the knee. All patients had American Society of Anesthesiologist (ASA) score of 1–2. Preoperative alignment was measured using weight-bearing roentgenograms and the varus anatomical angle of knees ranged from −2.23° to 2.36°. The range of motion of knee and functional outcome scoring (Knee Society Score (KSS), Oxford Knee Score (OKS), and Short Form 36 Health Survey (SF-36)) were recorded pre and postoperatively. The KSS consists of two components: knee score and functional score. Knee score is an objective evaluation, while functional score is a subjective evaluation of patient’s symptoms and function. 12 The OKS is scored differently from its counterpart, as its score is inversely proportional to the outcome. 13 The SF-36, like KSS, consists of two components: physical and mental. 14
The surgical exposure for the patients in this study group involves a medial parapatellar approach to the knee, with the quadriceps incised superiorly at the musculotendinous interval and followed distally around the patella and ending just medial to the patella tendon. Femoral and tibial bone cuts are made using jigs, and posterior-stabilized prostheses were used in all cases. Patellar debridement is performed without resurfacing. The quadriceps tendon is subsequently repaired with interrupted no. 1 vicryl sutures, followed by layered closure of the subcutaneous tissues and skin. The patients are allowed to weight bear with a walking frame and are started on physiotherapy after postoperative knee X-ray radiographs are reviewed. The patients are discharged to a rehabilitation facility or sent home with outpatient physiotherapy, when the range of motion of the knee is at least 90° and when the patients are able to climb stairs, and this usually occurs on the fourth postop day. Ambulation may be progressed to one with walking stick, if the patient is doing well. Physiotherapy is then continued on an outpatient basis. At the first outpatient visit 2 weeks after surgery, the sutures were removed for the patients. The patients are then followed up in the outpatient clinic at 2 months, 6 months, 12 months, and 24 months from the time of surgery.
Case reports
Case 1. A 72-year-old Chinese female underwent TKA for her left knee osteoarthritits. When reviewed at 2 weeks postoperatively, she was ambulant with walking stick and postoperative range of motion was 5° to 120°. However, the patient came back to the clinic on the same day after her review when she was heard a pop sound in her knee during her transfer to the car. She experienced pain in the left knee and was unable to actively extend her knee. Physical examination revealed a defect over the quadriceps tendon and reduction in active extension, with a passive range of motion of 0° to 120°. The X-ray radiograph did not reveal fracture (Figure 1a). The ultrasound of left knee showed disruption of distal quadriceps tendon architecture at the superior pole of left patella with small bony fragment on the superior lateral aspect of the patella measuring about 1 cm. The quadriceps tendon to patellar bone gap was measured at about 1.1 cm.
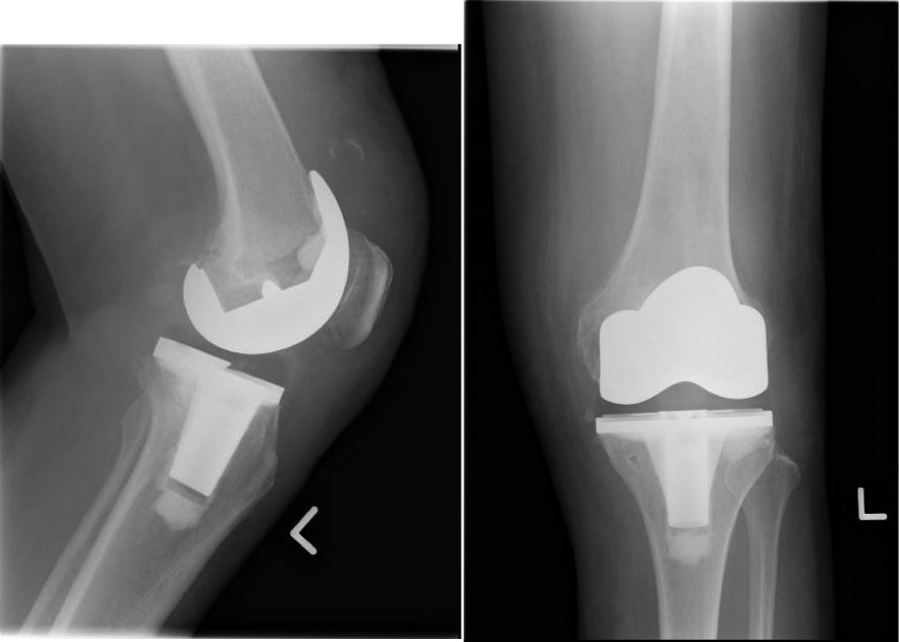
X-ray radiograph of left knee: soft tissue swelling in suprapatellar region. No obvious periprosthetic fracture/loosening.
The patient underwent surgical repair of the quadriceps tendon the next day. Intraoperative finding of a left complete full thickness quadriceps tendon tear was noted (Figure 1b). Krackow repair was performed with two 6.5 triple-loaded suture anchors and with Ethibond 5/0 suture transosseous repair. The patient was kept on back slab for 2 weeks and on full cylindrical cast for 1 month postoperatively.

Intraoperative finding of complete thickness quadriceps tendon tear.
The patient subsequently recovered well and was able to perform active quadriceps extension. She was able to walk independently in the subsequent follow-ups. At 2 years postoperative assessment, the patient had improvement in her functional outcome scores and range of motion as compared to the preoperative scores (Table 1).
Patients’ characteristics.

BMI: body mass index; ASA: American Society of Anesthesiologist.
Patients’ clinical presentation.

Details of the patients’ management.

Functional scores and range of motion of the knee for case 1.

OKS: Oxford Knee Score; KSS: Knee Society Score; SF-36: Short Form 36 Health Survey.
Case 2. A 57-year-old Chinese gentleman underwent TKA for his left knee osteoarthritis. He presented to the clinic 1 month postoperatively with pain in his left knee after he slipped and fell on his operated knee. Physical examination revealed wasting of the left quadriceps muscles. The quadriceps tendon was intact with no palpable gap. The extensor mechanism was intact with range of motion of 0° to 90°. The X-ray radiographs of his left knee (Figure 2a) did not reveal any periprosthetic fracture. The clinical impression was that of postoperative quadriceps weakness, and the patient was advised to continue outpatient physiotherapy for muscle strengthening.

X-ray radiograph of left knee: no significant periprosthetic abnormalities to suggest either loosening or infection. No acute fracture is detected. There is neither callus formation nor periosteal reaction demonstrated.
During the follow-up at 2 months postoperatively, the patient still required walking aid due to persistent right knee pain. On examination, there was wasting of quadriceps muscle and weakness in knee extension with active range of motion of 45°–90°. A gap was palpable on the quadriceps tendon. The patient was arranged for ultrasound of left quadriceps (Figure 2b) which revealed complete rupture of quadriceps tendon with retraction gap of about 4.7 cm in knee flexion. The tendon tear was found 2.5 cm above the patella.

Ultrasound report of quadriceps tendon: complete rupture of the quadriceps tendon with retraction gap of approximately 4.7 cm measured in knee flexion. A lobulated, septated fluid collection is seen between the retracted tendon edges. The tendon tear is located at about 2.5 cm above the patella. Underlying suprapatellar knee effusion also noted.
The patient underwent surgical repair of the quadriceps tendon. Intraoperative finding was a transverse intrasubstance tear of the left quadriceps tendon. The quadriceps tendon tear was exposed and debrided. Direct repair was performed with eight core sutures of Ethicon Ethibond 5-0 and with running epitendinous stitches using Ethicon Ethibond 2-0. The patient was kept on back slab for 2 weeks and on full cylindrical cast for 1 month postoperatively.
The patient subsequently recovered well and was able to perform active extension of his left knee. He was able to walk independently in the subsequent follow-ups. At 6 months postoperative assessment, the patient had poorer functional outcome and range of motion as compared with the preoperative scores. The patient was lost to follow up for the postoperative 2-year assessment (Table 2).
Functional scores and range of motion of the knee for case 2.

OKS: Oxford Knee Score; KSS: Knee Society Score; SF-36: Short Form 36 Health Survey.
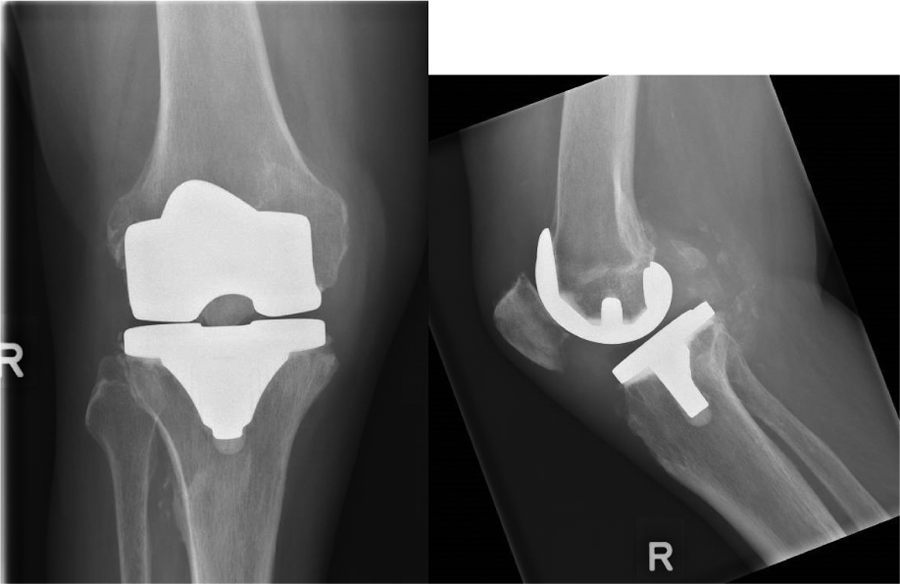
Case 3. A 74-year-old Indian gentleman underwent TKA for his right knee osteoarthritis. He presented to the clinic at 1 month postoperatively with difficulty in ambulating due to pain in his right knee after he slipped and twisted his operated knee. The physical examination revealed wasting of the right quadriceps muscles. The quadriceps tendon was intact with no palpable gap. The extensor mechanism was intact with range of motion of 0° to 120°. The X-ray radiograph of right knee did not reveal periprosthetic fracture (Figure 3). The clinical impression was that of postoperative quadriceps weakness, and the patient was advised to continue physiotherapy for muscle strengthening.

X-ray radiograph of right knee postfall: no evidence to suggest loosening. Soft tissue swelling with an effusion is noted in the knee joint.
During the follow-up at 2.5 months postoperatively, the patient was still unable to ambulate due to persistent pain and also weakness of the right knee. On examination, there was wasting of quadriceps muscles and weakness in knee extension with passive range of motion of 0° to 120°. A gap was palpable on the quadriceps tendon. The patient was sent for ultrasound of the quadriceps tendon, which revealed a full thickness but incomplete tear of the distal quadriceps tendon (more than 50% of tendon substance), involving mainly the medial and central aspects.
The patient underwent surgical repair of the quadriceps tendon. Intraoperative finding was a partial avulsion tear of right quadriceps tendon over previous surgical incision and repair. The partial tear was completed and debrided. Primary repair of the tear was performed with six core sutures of Ethibond 5/0. The postrepair strength was tested acceptable. The patient was kept on back slab for 2 weeks and on full cylindrical cast for 1 month postoperatively.
The patient subsequently recovered his quadriceps strength but was still weak on walking. He required walking frame for ambulation and was continued with physiotherapy. At 6 months postoperative assessment, the patient had poorer functional outcome and range of motion as compared with the preoperative scores. The patient was lost to follow up for the postoperative 2-year assessment (Table 3).
Functional scores and range of motion of the knee for case 3.

OKS: Oxford Knee Score; KSS: Knee Society Score; SF-36: Short Form 36 Health Survey.
Case 4. A 73-year-old Indian gentleman underwent TKA for both knees in separate settings (left followed by right). At 10 days after his right TKA, the patient presented to the emergency department with pain and weakness in his right knee after a fall from his commode. The physical examination revealed wasting of the right quadriceps muscles. The quadriceps tendon was intact with no palpable gap. The extensor mechanism was intact with range of motion of 0° to 100°. The X-ray radiograph of right knee (Figure 4) did not reveal periprosthetic fracture. The clinical impression was that of postoperative quadriceps weakness, and the patient was advised to continue physiotherapy for quadriceps strengthening.
X-ray radiograph of right knee post fall: no evidence to suggest loosening. Densities in the posterior joint compartment are likely due to loose bodies. Small joint effusion is seen.
During the follow-up at 2.5 months postoperatively, the patient was reviewed in the clinic after having another fall 2 weeks prior due to weakness in right quadriceps. The patient still required walking aid for ambulation and complained of persistent pain and weakness of his right knee. On examination, there was wasting of quadriceps muscles and weakness in knee extension with range of motion of 30° to 100°. There was a gap palpable in the quadriceps tendon. The patient was arranged for ultrasound of right quadriceps tendon, which revealed near complete tear of the quadriceps tendon with some fibers of the superficial lamina medially still intact. The torn ends are significantly retracted, measured at approximately 6 cm, and the intervening gap is filled by likely organized hematoma or echogenic fluid.
The patient underwent surgical repair of the quadriceps tendon. Intraoperative finding was right quadriceps tendon partial tear involving 50% of the deep portion near the insertion site at the superior pole of patella. It was noted that previous total knee replacement extensor mechanism repair site had healed and was intact. The partial tear was completed and debrided. Then, the full thickness repair was done using Ethibond 5/0 core sutures. The patient was kept on back slab for 2 weeks and on full cylindrical cast for 1 month postoperatively.
The patient subsequently recovered active extension of his right knee but still had residual weakness in quadriceps strength. He was ambulant with walking frame and was continued on physiotherapy. However, 2 years after the repair, patient was wheelchair bound in the community. As compared with the preoperative score, the patient had relatively poorer functional outcome scores but slightly improved range of motion (Table 4).
Functional scores and range of motion of the knee for case 4.

OKS: Oxford Knee Score; KSS: Knee Society Score; SF-36: Short Form 36 Health Survey.
Discussion
Postoperative quadriceps rupture is a rare but devastating complication that can occur after TKA. In our study, three out of the four patients had poorer outcome scores after repair of the quadriceps tendon rupture. As mentioned in the literature, primary repair of extensor mechanism after TKA has low success rate. 8 –11 Schoderbek et al. reported that 6 out of 290 patients in the North American Knee Arthroplasty Revision study, who had a complication of extensor mechanism disruption, have overall worse functional outcomes. 11 Dobbs reported unsatisfactory results with complications in 10 out of 26 patients who underwent operative repair for post-TKA quadriceps tear. 10 Yun et al. also reported the unfavorable outcomes after repair of post-TKA quadriceps rupture in a case report of three patients. 9 Dobbs and colleagues had recommended nonoperative treatment for partial quadriceps tendon tear, as they had reported that the operative management of partial tear had high rate of complication in contrast to nonoperative management. 10 The three patients in our study who underwent direct suture repair for partial quadriceps rupture had poorer outcomes. However, the three patients were considered treated conservatively by default, as their problem was not diagnosed initially. Surgical intervention may be considered, if partial quadriceps rupture does not improve after a trial of conservative management. The one patient in our study with improved outcome had complete quadriceps tendon tear and underwent transosseous repair with suture anchors. Kim et al. described the use of suture anchor repair of post-TKA quadriceps tendon tear and reported favorable outcomes. 15
The literature has identified several risk factors associated with extensor mechanism disruptions, and they can be classified into patient-related and surgeon-related factors. Patient-related factors include prior knee procedures, previous knee infection, prior extensor mechanism alignment procedures, trauma, and patient’s comorbidities such as diabetes mellitus, obesity, rheumatoid arthritis, systemic lupus erythematosus, and chronic renal failure. 10,11,16 –21 In our study, two of the patients had risk factors of diabetes mellitus, obesity, and chronic renal failure. Surgeon-related factors include choice of prosthetic design and surgical techniques. 11,20,22 –24 Inadequate exposure leading to excessive strain to extensor mechanism during retracting, overresection of patella or extensor tendons, and suboptimal component placement can predispose to quadriceps rupture. We also postulate that the incision into the quadriceps tendon as part of the medial parapatellar approach may have a bearing on quadriceps tendon healing and risk of rupture. Making the incision lateral to the musculotendinous interval as opposed to at the interval itself would result in partial disruption of the integrity of the quadriceps tendon insertion to the proximal pole of the patella. This could possibly contribute to postoperative quadriceps rupture in the patients.
In our study, three patients had a delay in diagnosis and did not have favorable outcomes. It is noted that although the patients presented with postoperative weakness and pain of the knee after the fall, the extensor mechanism was intact with no extensor lag and there was no palpable tissue defect on examination. There was no clinical suspicion for quadriceps rupture until subsequent follow-up. It is common for patients to have postoperative quadriceps weakness from deconditioning. Mizner et al. reported in a prospective study of 40 patients who underwent TKA, there is a significant worsening of knee range of motion, quadriceps strength, and performance on functional test 1 month after surgery. 25 Postoperative quadriceps weakness can potentially mask the diagnosis of quadriceps rupture. In the background of trauma, we recommend ultrasound scanning for all the patients with postoperative extensor weakness. This can prevent a delayed diagnosis and a delayed repair of the quadriceps tendon as had happened to our three patients. The three patients in our study had undergone quadriceps tendon repair of 1–2 months after the injury. It is largely agreed in the literature that prompt repair of the tendon is recommended to avoid retraction of the soft tissues. 26 –28 The delayed diagnosis and repair in these patients can explain the poor clinical outcomes that ensued.
Conclusion
Quadriceps rupture is an uncommon but devastating complication of TKA. We believe efforts should be focused on prevention of such a complication. Meticulous surgical techniques during the medial parapatellar approach to preserve the integrity of quadriceps can reduce the risk of rupture. Prompt diagnosis is also very important, as delayed treatment may lead to poor outcomes. Postoperative quadriceps weakness can potentially mask the diagnosis of quadriceps rupture. Careful history taking, looking into mechanism of injury, risk factors, symptoms, and physical examination should be carried out. In the background of trauma, any quadriceps weakness even without a palpable gap or reduction in range of active motion should be taken as a red flag for possible quadriceps tendon rupture. An ultrasound evaluation to exclude a quadriceps tendon rupture should be promptly performed after a fracture is excluded.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.