
Abstract
Background:
Revision of failed anatomic total shoulder arthroplasty or hemiarthroplasty is a challenging procedure. Restoring adequate soft tissue balance in the revision setting can be particularly problematic. When persistent posterior instability is encountered in the revision setting, options include changing component position or size, posterior capsular plication (PCP), or conversion to a reverse arthroplasty. The purpose of this study was to report the clinical and radiographic outcomes, complications, and reoperations of PCP performed in the setting of revision anatomic shoulder arthroplasty.
Patients and Methods:
Between 1975 and 2013, 15 patients (16 shoulders) had PCP during revision anatomic shoulder arthroplasty. Indications for revision arthroplasty included posterior instability in 15, glenoid loosening in 3, polyethylene wear in 2, and glenoid erosion in 1 shoulder. The mean (standard deviation (SD)) age was 60.1 (12.6) years, and the median (range) follow-up was 68 (2–228) months. A retrospective chart review was conducted to obtain all data.
Results:
At the last follow-up, nine shoulders (56%) had absence of posterior radiographic subluxation. Five (31%) cases underwent reoperation due to persistent posterior instability. Complications were observed in seven (44%) cases. Complete pain relief was achieved in four (25%) shoulders. The mean (SD) postoperative forward flexion, external rotation, and the American Shoulder and Elbow Surgeons score were 110° (41°), 40° (29°), and 62.1 (21.9), respectively. Results were excellent in two (13%), satisfactory in seven (44%), and unsatisfactory in seven (44%) shoulders.
Conclusions:
PCP to correct posterior instability during revision anatomic shoulder arthroplasty had an unacceptably high failure rate. In these circumstances, consideration should instead be given to conversion to a reverse shoulder arthroplasty.
Keywords
Introduction
Total shoulder arthroplasty (TSA) has been reported to provide successful outcomes in terms of pain relief and function, 1 –4 but is also associated with potential complications. Instability after shoulder arthroplasty is a common complication, 5 and achieving adequate soft tissue balance is a challenging scenario for even experienced shoulder surgeons.
Management of instability after anatomic shoulder arthroplasty may require soft tissue procedures, revision arthroplasty with or without bone graft, bone block stabilization procedures, or a combination. 6 –8 There are three studies where the principal treatment for posterior instability was revision arthroplasty with or without bone graft, though a small number of patients also underwent posterior capsular plication (PCP) to improve soft tissue tension balance. 9 –11 Acceptable shoulder stability was reported, 9 and pain relief and range of motion were modestly improved. However, none of these studies were specifically conducted to evaluate the usefulness of this soft tissue procedure. We observed a 71% success rate of PCP at correcting intraoperative posterior instability during primary anatomic shoulder arthroplasty. 12 To the best of our knowledge, there are no dedicated studies investigating the results of PCP in the setting of revision for unstable shoulder arthroplasty.
The purpose of this study was to report the clinical and radiographic outcomes, complications, and reoperations of revision shoulder arthroplasty using anatomic components combined with PCP to correct persistent posterior subluxation at the time of the index revision procedure.
Patients and methods
Procedures
Between 1975 and December 2013, all patients undergoing revision of a failed anatomic TSA or hemiarthroplasty (HA) by three senior surgeons (JWS, RHC, and JSS) were identified using our institutional Total Joint Registry database. Inclusion criteria were the following: age above 18 years, PCP performed during revision of TSA or HA to correct persistent intraoperative posterior subluxation or dislocation, minimum clinical follow-up of 2 years or until revision surgery, and the availability of postoperative anterior–posterior and axillary radiographs. Patients with an infected primary arthroplasty undergoing staged revision, cuff-tear arthropathy, fracture sequelae with absence of greater and/or lesser tuberosity, or isolated inferior instability were excluded. Shoulders replaced using metal-backed glenoid components were not excluded, although this component design is not currently used in our institution. A retrospective chart review was conducted to obtain the relevant data for the present study. After data collection, a radiographic assessment session was prepared in which all preoperative, early follow-up, and last follow-up radiographs were evaluated by two senior surgeons (JWS and JSS) blinded to the clinical outcomes. This study received Institutional Review Board approval (ID 15-006671).
Patients
A total of 688 revision TSA or HA were performed in the study period by the three senior surgeons. Of these, 21 shoulders (3%) underwent PCP at the time of revision arthroplasty. Three patients were excluded because the follow-up was less than 2 years, one case because the PCP was performed during staged revision arthroplasty for infection, and one case because the greater tuberosity was absent as a result of a proximal humeral fracture treated with an HA. This left a total sample of 16 cases in 15 patients available for the present study. The index procedure for the present study was the first revision arthroplasty performed at our institution in which a PCP was used to correct intraoperative subluxation. At the last follow-up, six (38%) cases were seen in the office for follow-up, and 10 (63%) returned a validated follow-up questionnaire. 13 There were eight men and seven women (one male patient had undergone bilateral revision arthroplasty) with a mean (standard deviation (SD)) age of 60.1 (12.6) years. There were 12 right-handed and 3 left-handed patients, with eight revision arthroplasties performed on the dominant side and eight performed on the nondominant side.
The indications for the primary arthroplasty were the following: primary osteoarthritis in nine (56%) cases (four of them with preoperative posterior subluxation), posttraumatic osteoarthritis in three (19%) cases, osteoarthritis secondary to shoulder instability in two (13%) cases, osteoarthritis secondary to glenoid dysplasia in one (6%) case, and rheumatoid arthritis in one (6%) case. One patient had undergone a prior Bristow procedure and one patient had undergone prior a Putti-Platt procedure, both for anterior instability prior to the development of capsulorrhaphy arthropathy. There were 15 (94%) cases of primary TSA and 1 (6%) case of primary HA. The primary arthroplasty was done elsewhere in six (38%) cases. One patient also had one revision arthroplasty performed elsewhere, and another patient had two revision arthroplasties performed elsewhere before being referred to our institution.
The reason for revision arthroplasty was posterior instability in 15 shoulders, glenoid loosening in 3, polyethylene wear in 2, and glenoid osteoarthritis (failed HA) in 1 shoulder, though some patients had more than one reason for revision. The median (range) length of follow-up was 68 (2–228) months. There was one patient with a follow-up of 2 months and another one with a follow-up of 17 months. These shoulders were included because they represented early failures that require revision surgery within the first 2 years after revision arthroplasty. The length of follow-up in both patients was 50 and 101 months, respectively. The median (range) radiographic follow-up was 53 (6–183) months.
Radiographs before the primary arthroplasty were not available in 10 (63%) cases. In the remaining six cases, using the original Walch classification of glenoid types, 14 there were two (13%) cases with A2, three (19%) cases with B2, and one (6%) case with C. Bone erosion was present in five of the six cases, being moderate in the posterior glenoid in three (19%) cases, severe in the posterior glenoid in one (6%) case, and severe in the central glenoid in one (6%) case. Four (25%) cases had no superior subluxation, and two (13%) cases had mild superior subluxation. There were three (19%) cases with moderate and three (19%) cases with severe posterior subluxation.
All patients had radiographs before the index procedure available. There were four (25%) cases with no superior subluxation, six (38%) cases with mild, five (31%) cases with moderate, and one (6%) case with severe superior subluxation. There were eight (50%) cases with moderate posterior subluxation, three (19%) cases with severe posterior subluxation, and five (31%) cases with posterior dislocation. The glenoid was loose in three (19%) cases, and polyethylene wear was present in two (13%) cases.
Surgical procedure
All operations were performed through a deltopectoral approach. In three cases, the deltoid was detached from the clavicle and anterior acromion (anteromedial approach). 15 During the approach, the anterior aspect of the distal deltoid muscle was torn in one patient and required repair at the end of the case. According to operative notes, the status of the posterior–superior rotator cuff was as follows: torn in the anterior supraspinatus in 1 (6%) case, torn in the supraspinatus and anterior aspect of the infraspinatus in 1 (6%) case, thin but intact in 4 (25%) cases, and intact in 10 (63%) cases. The subscapularis was intact in 15 (94%) cases and thin with scar tissue formation requiring repair in 1 (6%) case. Among patients without intraoperative information on the posterior–superior rotator cuff, there were three (43%) cases without, one (14%) case with mild, two (29%) cases with moderate, and one (14%) case with severe superior humeral head migration. Clinically, only two of these patients had mild preoperative weakness in abduction and external rotation.
The surgical technique for PCP has been previously described. 12 In cases of posterior subluxation of the humeral head trial of more than 40%, the head size was increased in an attempt to increase soft tissue tension and, therefore, joint stability. All shoulders included in this study had persistent posterior humeral head subluxation despite the use of a larger head size, and a decision was made to perform the PCP. A bone hook was used to retract the humerus laterally and create a working space for the PCP procedure. Then, multiple nonabsorbable sutures were placed lateral to medial to shorten the posterior capsule. All the sutures were first placed, and then, the bone hook was removed to allow adequate tightening of the sutures.
The index procedure was an HA in three (19%) cases because of insufficient glenoid bone stock and TSA in 13 (81%) cases (Table 1). The mean (SD) operative time was 228 (80) min. There were 12 Cofield (monoblock or modular) Shoulder System prostheses (Smith and Nephew, Memphis, TN, USA), 2 Comprehensive Total Shoulder System prostheses (Biomet, Warsaw, IN, USA), 1 Arthrex Univers™ II shoulder system (Arthrex, Naples, FL, USA), and 1 Neer II prosthesis (3M Company, St Paul, MN, USA). There were six (38%) metal-back implants, one of them with posterior augmentation. The humeral stem was cemented in two (13%) cases, and the glenoid component was cemented in five (32%) cases. Bone graft was used in four (25%) cases: all of them in the glenoid and one also in the humeral side. Three bone grafts were in patients who underwent HA. The procedure was all soft tissue in one (6%) case, with division of the anterior–inferior capsule, tightening of the rotator interval, and PCP.
Clinical and functional outcomes.
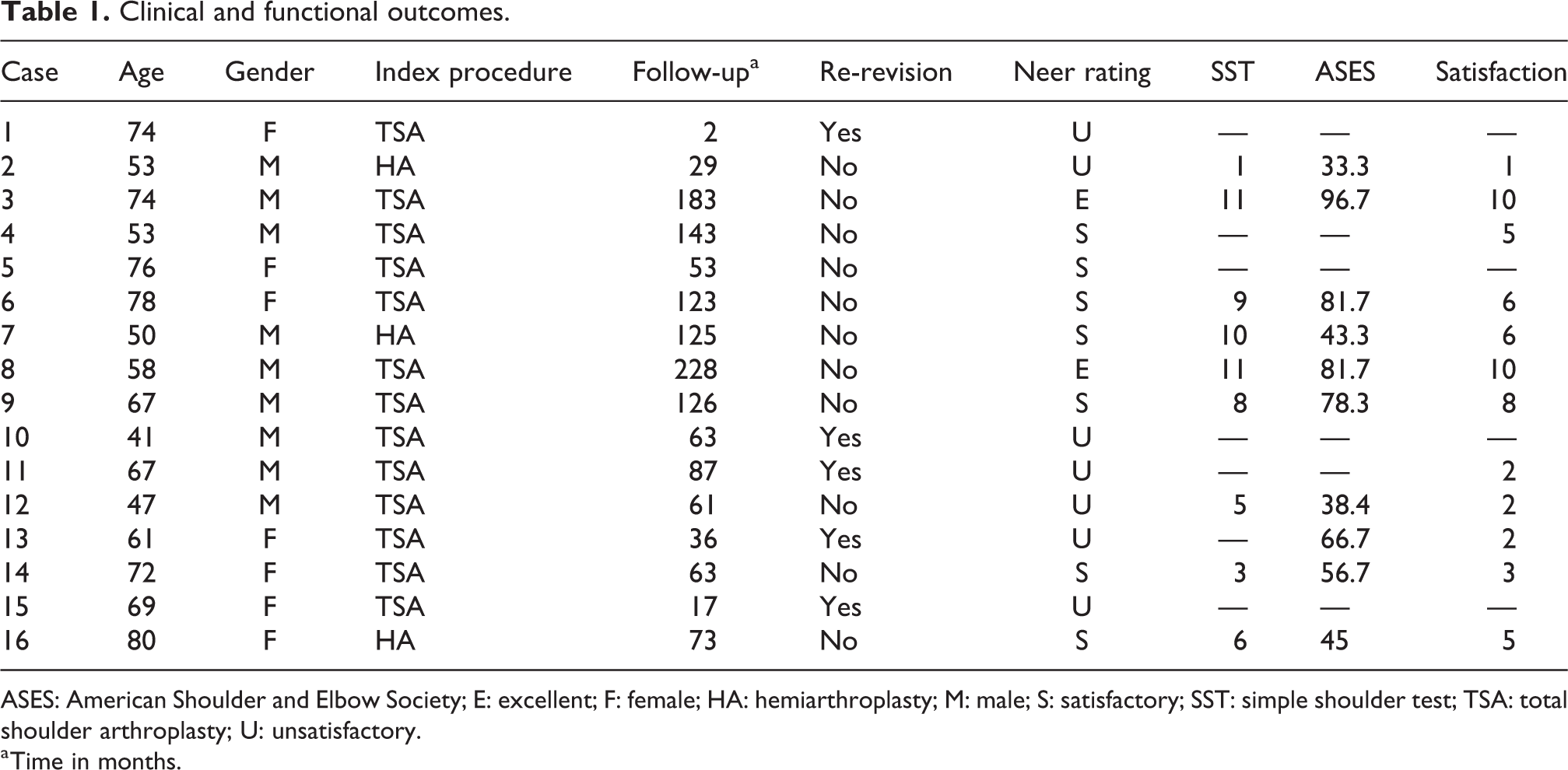
ASES: American Shoulder and Elbow Society; E: excellent; F: female; HA: hemiarthroplasty; M: male; S: satisfactory; SST: simple shoulder test; TSA: total shoulder arthroplasty; U: unsatisfactory.
a Time in months.
Following the index procedure, a shoulder immobilizer (sling) was used in seven (44%) cases, shoulder abduction brace in six (38%) cases, shoulder external rotation brace in one (6%) case, and shoulder abduction splint in two (13%) cases. Immobilization was maintained for 6 weeks in all except two cases. One patient used an abduction brace for 10 weeks, and a second patient used a shoulder brace in external rotation for 12 weeks.
Outcome assessment
The retrospective review was used to obtain (1) pre- and postoperative pain (1 = no pain; 2 = mild pain; 3 = pain with usual activities; 4 = moderate pain; and 5 = severe pain) and range of motion (ROM); (2) pre and postoperative radiograph characteristics; (3) characteristics of the surgical treatment (operative time, problem identified, implants used, and the use of bone graft or cement); (4) complications and reoperations; (5) functional outcomes (Neer rating scale, simple shoulder test (SST), and American Shoulder and Elbow Surgeons (ASES) score); and (6) patient satisfaction on a 0–10 scale (where 0 is not satisfied). Information on the subjective feeling of stability was also collected from the charts. The Neer rating system used in this study was first described by Neer et al. 3 and later modified by Cofield. 1 The result was considered excellent if the patient had no or slight pain, active abduction to 140°, and external rotation to 45° and was satisfied with the procedure. A satisfactory result consisted of no or slight pain or moderate pain only with vigorous activity, active abduction to 90°, external rotation to 20°, and the patient being satisfied with the procedure. A result was graded as unsatisfactory if the criteria for excellent or satisfactory were not met or if the patient needed a revision procedure.
The principal radiographic outcomes included the anterior–posterior and axillary views in the preoperative, immediate postoperative, and last follow-up periods. Plain radiographs before the primary procedure or previous revision surgery (in patients revised elsewhere) were evaluated whenever available. The radiographic parameters evaluated before and after the index procedure included presence and degree of superior and posterior subluxation, humeral or glenoid radiolucent lines, implant loosening, and component shifting. In cases where radiographs before the primary procedure were available, glenoid erosion (degree and location), glenoid type according to the Walch classification, 14 and humeral head superior and posterior subluxation were also collected. The degree of subluxation was categorized as none, mild (<25%), moderate (25–50%), and severe (>50%). Glenoid radiolucencies were classified as 0 (none), 1 (faceplate only), 2 (1 mm incomplete), 3 (1 mm complete), 4 (1.5 mm incomplete), 5 (1.5 mm complete), and 6 (2 mm complete). Humeral radiolucencies were classified as 0 (none), 1 (1 mm incomplete), 2 (1 mm complete), 3 (1.5 mm incomplete), 4 (1.5 mm complete), 5 (2 mm in 1–2 zones), 6 (2 mm in 3–4 zones), and 7 (2 mm complete). The presence of glenoid/humeral loosening or implant shifting was determined by consensus between the two senior surgeons involved in radiograph analysis (JWS and JSS). Radiographic success of the PCP was considered when there was absence of posterior subluxation in the most recent radiographs.
Statistical analysis
Descriptive statistics were used to summarize the outcomes. Data were reported as number of cases (n), percentage, mean, median, SD, and range. Nonparametric tests were used for all preoperative–postoperative comparisons. A paired Wilcoxon test was used to compare preoperative and postoperative forward flexion and external rotation. The Fisher’s exact test was used to compare preoperative and postoperative pain and internal rotation. The α level was set at 0.05. All the statistical analyses were conducted using the SPSS Version 21 program (SPSS Inc., Chicago, Illinois, USA).
Results
According to the Neer rating system, the clinical results were excellent in two (13%) cases, satisfactory in seven (49%) cases, and unsatisfactory in seven (49%) cases (Table 1). The mean (SD) SST and ASES scores were 7.1 (3.6) and 62.1 (21.9), respectively. The mean (SD) satisfaction score was 5 (3.1). With the numbers available, differences between the preoperative and postoperative values for pain, forward flexion, external rotation, and internal rotation were not statistically significant (Table 2). Postoperatively, there were four (25%) shoulders with no pain, four (25%) with mild pain, and eight (50%) with moderate pain.
Comparison of preoperative and postoperative pain and range of motion.

SD: standard deviation.
a Values are median (range).
At most recent radiographic follow-up, nine shoulders (56%) had absence of posterior subluxation. There was one (6%) case of moderate posterior subluxation, four (25%) cases of severe posterior subluxation, one (6%) case of posterior dislocation, and one (6%) case of moderate anterior subluxation. At most recent radiographic follow-up, six (38%) cases had absence of superior subluxation, four (25%) had mild superior subluxation, four (25%) had moderate superior subluxation, and two (13%) had severe superior subluxation. Twelve (75%) cases improved, three (19%) cases had equal, and one (6%) case had worse posterior subluxation in the last compared with the preoperative radiograph. Three (19%) cases improved, six (38%) cases had equal, and seven (44%) cases had worse superior subluxation in the last compared with the preoperative radiograph. No patients had radiographic glenoid or humeral component loosening, but one (6%) case had 2-mm incomplete glenoid radiolucent line and two (13%) cases had faceplate-only glenoid radiolucent lines.
The intraoperative problems identified during surgery, their solutions, and the success of the procedure at providing a stable and well-balanced joint (radiographic success) are summarized in Table 3. There were five cases in which the only problem identified was a lax posterior capsule. Four (80%) of these cases had an unsuccessful procedure. Of the 11 cases in which a lax posterior capsule and an additional component problem were identified (loosening, wear, or malposition), there were 8 (73%) successful and 3 (27%) unsuccessful results (Figure 1). Four (100%) of the four cases with humeral stem subsidence or excessive retroversion that was corrected during surgery had a successful procedure (Table 3).
Problems and solutions during revision of unstable shoulder arthroplasty.
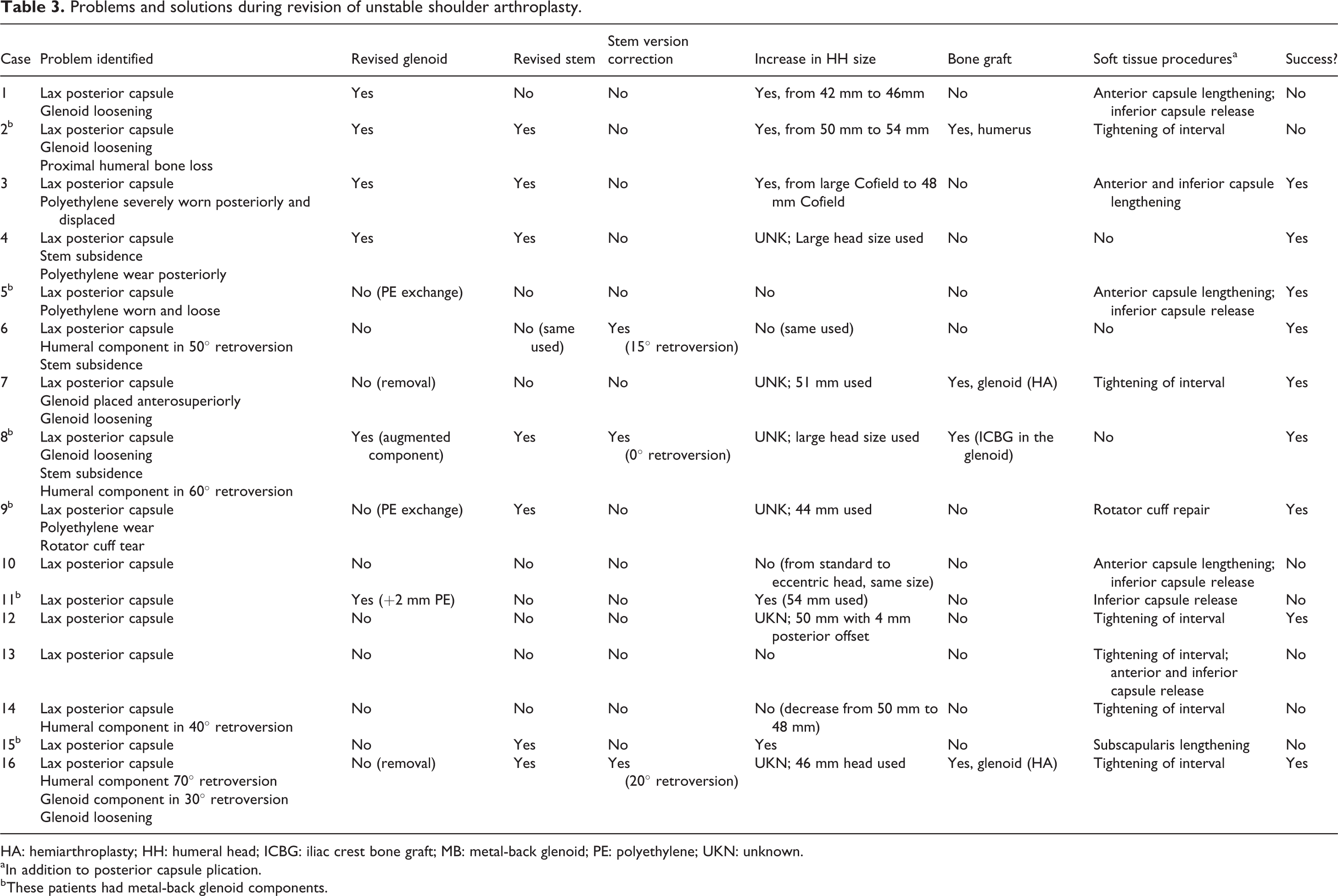
HA: hemiarthroplasty; HH: humeral head; ICBG: iliac crest bone graft; MB: metal-back glenoid; PE: polyethylene; UKN: unknown.
a In addition to posterior capsule plication.
b These patients had metal-back glenoid components.

Successful revision of total shoulder arthroplasty in a patient undergoing exchange of humeral component to correct 50° of retroversion and plication of the posterior capsule. Panel A: Anterior–posterior and axillary view radiographs before revision surgery demonstrating excessive retroversion of the humeral component and posterior dislocation of the humeral head prosthesis. Panel B: Anterior–posterior and axillary view radiographs 10 years after revision surgery demonstrating a well-centered humeral head prosthesis and corrected version of the humeral component.
Complications were observed in seven (44%) cases, including posterior dislocation in three (19%) cases, symptomatic posterior instability in two (13%) cases, subscapularis failure in one (6%) case, and posterior–superior rotator cuff failure in one (6%) case. Five (31%) cases underwent revision surgery after the index procedure (all were TSA) because of posterior instability or dislocation. None of the patients underwent conversion to an HA during the re-revision procedure. None of the patients underwent more than one revision surgery after the index procedure.
The intraoperative problems identified during the re-revision surgery, their solutions, the Neer rating, and the radiographic success are summarized in Table 4. There was one patient who had no follow-up of the re-revision procedure. Case 1 (Table 4) had a posteriorly dislocated prosthesis at last radiographic follow-up without implant loosening and with forward flexion and external rotation of 40°. However, because she had only slight pain, she did not want to have another re-operation. Case 10 (Table 4) has forward flexion of 100°, external rotation of 20°, and internal rotation to sacrum with only very mild pain, no posterior or superior subluxation, and no implant loosening at 25 months. This patient was satisfied with the re-revision procedure. Case 11 (Table 4) had forward flexion of 110°, external rotation of 50°, and internal rotation to L3, very slight pain during activities, no posterior or superior subluxation, and no implant loosening at 27 months. This patient had an SST, ASES score, and satisfaction of 7, 71.2, and 8, respectively. Case 15 had forward flexion of 135°, external rotation of 35°, and internal rotation to L4, no pain, no posterior or superior subluxation, but asymptomatic glenoid loosening at 92 months. This patient partially answered the questionnaire and had an SST of 12.
Problems, solutions, and outcomes in patients undergoing re-revision procedure for unstable shoulder arthroplasty.

PE: polyethylene; S: satisfactory; U: unsatisfactory.
a Time in months.
b In addition to posterior capsular plication.
Discussion
Persistent intraoperative posterior subluxation may be encountered at the time of revision shoulder arthroplasty performed using anatomic components. PCP has been recommended in these circumstances in an effort to improve soft tissue balance. Although PCP has been reported to provide moderate success in these circumstances in the primary setting, 12 the results of this study seem to indicate that it is less successful in the revision setting. Shoulders with obvious component malposition corrected during revision to an anatomic arthroplasty had a higher chance of a successful outcome, but overall, the failure rate was unacceptably high.
The treatment for posterior instability after shoulder arthroplasty and the intraoperative finding of posterior subluxation during revision of anatomic shoulder arthroplasty are challenging scenarios. Multiple factors may contribute, including rotator cuff deficiency, posterior capsular laxity, component retroversion, or anterior soft tissue contracture. Theoretically, the most effective treatment strategy is likely the correction of all potential causes of instability. Therefore, treatment considerations should include decreasing or correcting excessive humeral or glenoid component retroversion, increasing head size, rotator cuff repair, subscapularis and anterior capsule lengthening, and PCP, as indicated. To our knowledge, there are no studies specifically reporting the outcomes of PCP in the setting of persistent posterior subluxation at the time of revision shoulder arthroplasty using anatomic components.
PCP for the treatment of posterior instability after shoulder arthroplasty was first described by Namba and Thornhill. 16 The authors successfully treated a patient with posterior capsule laxity leading to instability during primary shoulder arthroplasty with PCP. Their technique involved the plication of the posterior capsule with sutures tied to the anterior aspect of the humeral neck after drilling holes into the proximal humerus. There are three studies that reported the use of PCP in patients undergoing revision arthroplasty for instability. 9 –11 Moeckel et al. reported the outcomes of three patients with posterior instability after shoulder arthroplasty. 9 Two patients had revision of components, and one patient had an isolated PCP. The treatment for the patients with revised components was correction of excessive retroversion of the humeral component (previously placed at 70°) and head size increase, and both patients had a stable revision arthroplasty. The third patient who underwent PCP alone had recurrent posterior subluxation. The ROM in successful cases was 108° and 132° of forward flexion and 39° and 43° of external rotation.
Wirth and Rockwood reported a series of 11 patients with instability after shoulder arthroplasty, of whom 7 had posterior instability. 11 The causes of instability were increased humeral component retroversion in four cases, posterior glenoid erosion in four cases, posterior capsular distension in five cases, and nonunion of tuberosities in one case. The treatment of these patients included correcting the humeral component retroversion, reestablishment of the glenoid version, and posterior capsulorrhaphy, as indicated. The outcomes were not specifically reported for the posterior instability cases, but stability was achieved in all but one patient, and there was no pain in three and mild pain in seven cases. The mean postoperative forward flexion and external rotations were 100° and 35°, respectively. Sanchez-Sotelo et al. reported the outcomes of 33 patients with instability after shoulder arthroplasty, from whom 14 had posterior instability and 8 of them were treated with PCP. 10 Although the outcomes were not reported specifically for the patients undergoing PCP, stability was restored in 9 (64%) of the 14 patients with posterior instability. Reoperation occurred in 7 (50%) of the 14 patients with posterior instability. The authors found significantly higher failure rates among patients treated for anterior compared with posterior instability. Considering the Neer rating for the entire sample, the authors reported 4 (11%) excellent, 6 (18%) satisfactory, and 23 (71%) unsatisfactory results. With the numbers available, they were unable to find a statistically significant association between the final outcomes and treatment characteristics (type of instability, type of revision, component malposition, or increased head size).
With the limited numbers available, it could not be statistically demonstrated in the present study that the results of patients undergoing PCP alone were worse than those undergoing PCP associated with component revision. However, it seems that the results of patients with only a lax posterior capsule as the cause of instability are worse compared with those with a lax posterior capsule associated with component malposition (Table 3). Therefore, it might be argued that PCP alone is not able to provide enough restraint to prevent posterior implant instability over time. Dines et al. observed that the outcomes of revision shoulder arthroplasty were better in patients with osseous or component-related problems compared with soft tissue deficiency. 17 However, only five of their patients were revised because of instability, and none of them included posterior instability. The outcomes in these five patients were fair in two and poor in three.
While the outcomes of PCP in the setting of intraoperative posterior subluxation of primary anatomic shoulder arthroplasty were successful in 70% of the cases, 12 PCP during revision arthroplasty for instability is associated with a very modest success. Therefore, conversion of anatomic to reverse shoulder arthroplasty should be considered in cases of instability after shoulder arthroplasty, especially when instability is caused only by posterior capsule laxity. Abdel et al. reported a very high success rate when unstable anatomic shoulder arthroplasties were revised to a reverse shoulder arthroplasty. 18
The present study has some limitations. First, it was a retrospective case series with a small number of patients. However, this study is the largest reported sample of patients treated with PCP during revision of unstable arthroplasty. Second, the patients were collected through a 30-year period, which overlays a period of substantial changes in implant design and surgical technique. Nonetheless, we believe all implants included in this study share similar biomechanical principles. Third, the absence of a comparative group prevented the establishment of a cause–effect relationship between the outcomes and PCP. This study has also strengths. First, it represents the largest reported series for the treatment of an uncommon but complex problem. Second, it demonstrates the clinically relevant finding that revision maintaining an anatomic arthroplasty holds questionable utility for patients with a posteriorly unstable anatomic shoulder arthroplasty, even if PCP is performed.
Conclusions
PCP for patients with posterior instability or residual intraoperative posterior subluxation in the setting of revision anatomic arthroplasty had a 44% failure rate. In these circumstances, consideration should be given to conversion of the anatomic arthroplasty to a reverse shoulder arthroplasty.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Cofield/Royalties: Smith/Nephew, DJO; Dr Sperling/Royalties: Biomet; Dr Sanchez-Sotelo/Royalties: Stryker; no other authors have anything to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.