
Abstract
Introduction:
The aim of this study was to analyze the survival of the Echelon® femoral stems in revision hip surgeries in patients with Paprosky I–IIIA femoral defects.
Patients and methods:
Sixty-six patients (70 hips) who underwent revision hip surgery with at least 3 years of follow-up data were included in the study between 2000 and 2013. The mean patient age was 64.5 (32–83) years, and the mean follow-up period was 93 (45–206) months. The reasons for revision were aseptic loosening in 55 (78.6%) patients, periprosthetic joint infection in 9 (12.9%) patients, periprosthetic fracture in 4 (5.7%) patients, and stem fracture in 2 (2.9%) patients. The preoperative and postoperative follow-up X-rays and functional scores were evaluated.
Results:
Five patients died in an average of 70 (45–86) months after surgery due to non-related diseases. We encountered sciatic nerve palsy in two patients and early hip dislocation in two patients, whereas 54 patients were able to walk without any assistive device. The remaining 12 patients required an assistive device to walk. The mean Harris hip score significantly increased from 34 (7–63) preoperatively to 72 (43–96) postoperatively. Aseptic loosening was observed in one patient. The survival of the porous-coated anatomical uncemented femoral stem was 98.4% over 10 years.
Conclusion:
This study showed that good clinical outcomes and survival can be obtained when using porous-coated anatomical uncemented femoral stems.
Introduction
The number of revision hip arthroplasties has been increasing annually due to the increasing number of primary hip arthroplasties performed in younger patients and mechanical stem failures. According to the study conducted by Coyte et al., the number of the revision hip surgeries is increasing by 4.7% each year. 1 It is estimated that the number of revision hip surgeries will double at 2026 compared with 2005 and that 96,700 revisions will be performed each year by 2030. 2
Revision hip surgery is a challenging procedure due to the lack of bone stock and distorted anatomical structure. Consequently, the complication rates for revision hip surgery are higher than those for primary hip arthroplasty. 3 –5 There are many options to be used in femoral stem revision surgery, such as long cemented or cementless stems, hydroxyapatite-coated stems, massive allografts, or proximal femur replacement implants. The advantage of the cementless femoral stem is that it allows for bone regeneration and the ability to adapt to different bone structures, given its modularity. Cemented femoral stems are also preferred for limited indications such as short life expectancy and marginal bone defects. Long femoral stems provide advantages clinically and radiologically by passing proximal poor bone stock and holding diaphysis. 4,5
Recent studies have been conducted in favor of cylindrical fully porous-coated uncemented femoral components for Paprosky types I–IIIa bone losses to achieve long-term predictable results. 6,7 In this study, we aimed to analyze survival of porous-coated cylindrical shaped diaphyseal femoral stems (Echelon™, Smith and Nephew; Memphis, Tennessee, USA; Figure 1) in revision patients with Paprosky types I–IIIa bone losses.

Echelon™, Smith and Nephew, Memphis, Tennessee, USA.
Materials and methods
Patient files were evaluated retrospectively after study approval by the institutional review board. Eighty-seven patients were identified as having undergone femoral component revision surgery with Echelon® stems between 2000 and 2013. Demographic features (age and gender), date and indication for revision surgery, intraoperative details, Paprosky classification of femoral bone loss, and data of the last known follow-up were extracted from the records. Twenty-one patients with insufficient information in their files or a follow-up shorter than 36 months were excluded. Seventy hip joints from 66 patients (41 women (62%) and 25 men (%38)) were included in the study. The mean age of the 66 patients at the time of surgery was 64.5 years (range 32–83 years). The mean follow-up period was 93 months (range 45–206 months). Both hips were included in four patients who underwent bilateral revision surgery. The indications for surgery were aseptic loosening in 55 (78.6%) hips, periprosthetic joint infections in 9 (12.9%) hips, periprosthetic fracture in 4 (5.7%) hips, and stem fracture in 2 (2.9%) hips (Table 1).
Demographic and clinical features of patients.
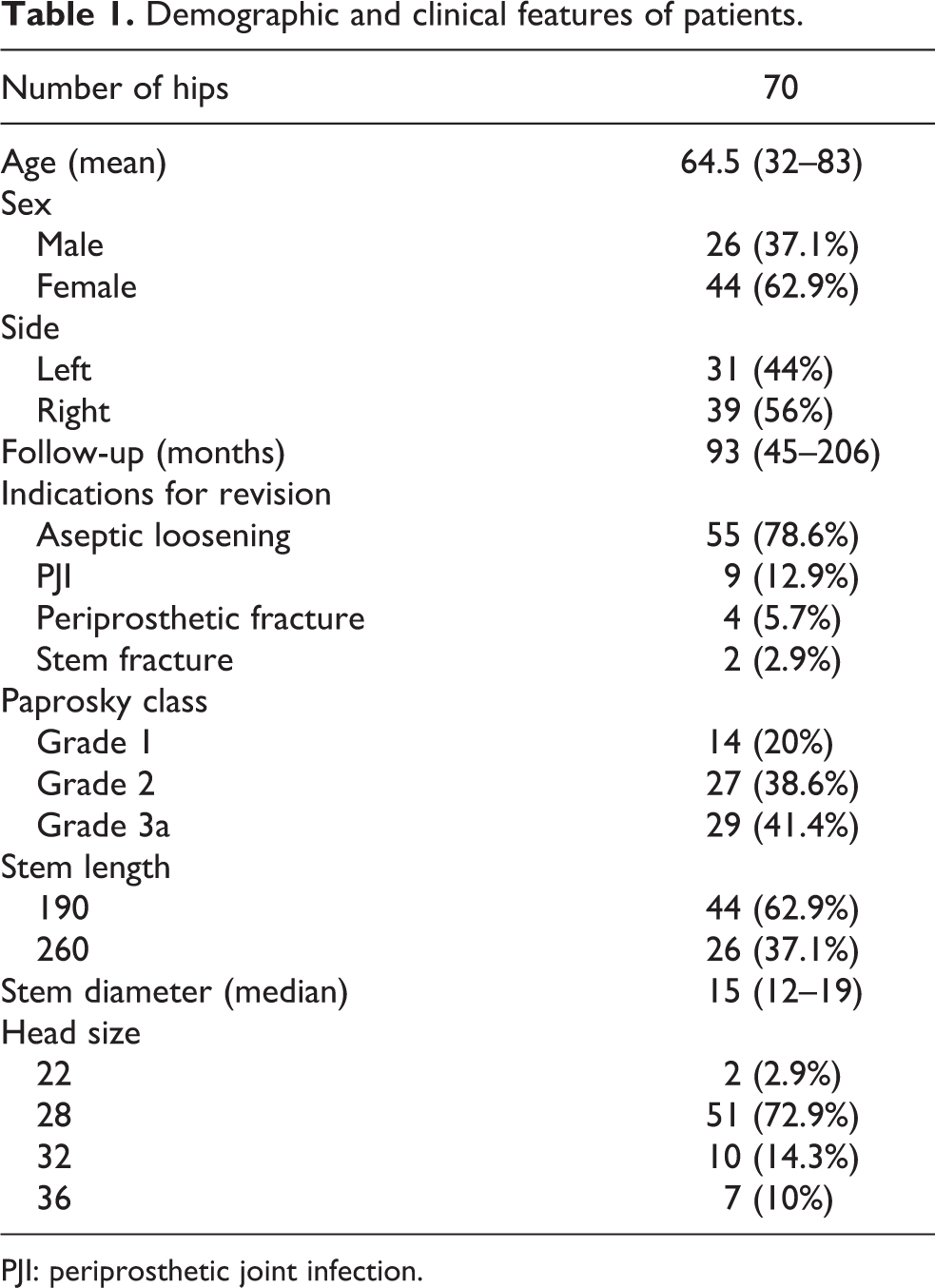
PJI: periprosthetic joint infection.
Our arthroplasty archive was used to analyze radiographs at preoperative, postoperative, and final follow-up evaluations. The preoperative values were obtained from patient files at each follow-up visit. A telephone audit was carried out with the patients who did not show up during the last 6 months to assess their functional status. Postoperative and follow-up X-rays were evaluated for subsidence, loosening, and wear of the liner. We defined loosening as radiolucent areas around the stem, progressive tilt of the stem, stem fracture, and subsidence of 5 mm or more of the stem. Stem design and manufacturing were not changed during this time. Only first revision surgeries with Echelon stems were included in the study.
Femoral defects were independently classified according to Paprosky femoral bone loss classification (7) by two senior authors. The femoral bone defects were type I in 14 hips, type II in 27 hips, and type IIIa in 29 hips. The clinical outcomes were evaluated using the Harris hip score. Pain, range of motion, walking, stair climbing, limp, and ability to conduct daily activities were evaluated by the Harris hip score.
The patients who had undergone revision surgery because of periprosthetic joint infection were revised in two stages, and the implantations were performed after removal of the antibiotic-loaded spacers. The femoral defects of the patients operated because of periprosthetic joint infection were Paprosky type I in two patients, type II in three patients, and type IIIa in four patients.
Surgical details
All patients were operated on in the lateral position using the direct lateral approach of the Hardinge. Extended trochanteric osteotomy was used in 17 (24%) hips. Fixation of the osteotomy was done with trochanteric plates in 5 hips and cables in 12 patients. To support the femoral shaft, the strut allograft was used in 13 patients. Other bone grafts, such as cancellous bone grafts, were used on three hips in this series. The femoral reconstruction was supported with cables or cerclage wires in 49 patients. Limb length discrepancy was checked and decided during the revision procedure. Cefazolin was given preoperatively for infection prophylaxis. Low-molecular-weight heparin (LMWH) and anti-embolic stockings were used for deep vein thrombosis prophylaxis. Most of the patients received LMWH until discharge, and prophylaxis was continued by LMWH for 3 weeks.
Statistical analysis
Kaplan–Meier survival analyses were used to evaluate stem survival. Differences between preoperative and postoperative scores were evaluated using the Wilcoxon matched pairs test. The level of significance was p < 0.05. All statistical analyses were performed using SPSS 20.0 (IBM Corp, Armonk, New York, USA) for oscar-sierra-space-xray (OSX).
Results
Five patients died after a mean period of 70 months (range 45–86 months) after the initial revision surgery due to non-orthopedic causes. Sciatic nerve palsy was observed in two patients, in which one healed completely and the other incompletely. Hip dislocation occurred in two patients. One patient was treated with closed reduction and abduction orthosis during the early postoperative period. Another patient who had hip dislocation at 33 and 37 months was treated with acetabular component revision for the first dislocation and closed reduction and abduction orthosis for the second dislocation. Other perioperative complications such as fracture or perforation were not seen during the operation in this special cohort group. Fifty-four patients were able to walk without any assistive device, 7 patients could walk with canes, 3 patients used sets of two crutches, and 2 patients used walkers. Revision surgeries need extensile approaches. Gluteus medius and abductor mechanism generally impaired during these extensile exposures. Infections are another reason for bone and soft tissue damage. Seven of the 12 patients who need assistive device had periprosthetic infections and two-stage revision. Remaining five elderly patients who need assistive device underwent revision surgery because of aseptic loosening of hemiarthroplasty with posterior approaches. As a conclusion, the patients have to use assistive device, had more soft tissue damage, and were at older age (mean 72 years old, range 52–81 years) in our cohort. The mean Harris hip score was 34 (763) preoperatively and 72 (43–96) at the last follow-up visit. The differences between the preoperative and postoperative scores were significant (p < 0.05; Figure 2(a) and (b)).
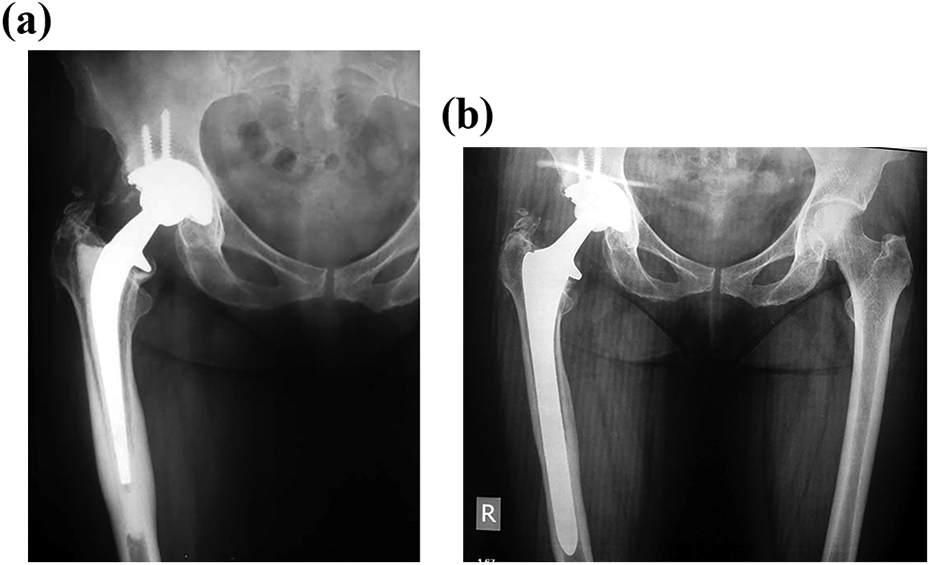
(a) Example of loosening in a 70-year-old female who underwent revision surgery for femoral component loosening at 9 years after the primary surgery. (b) X-ray of the same patient 9 years after the revision surgery.
Seven patients had thigh pain but only one patient had the evidence of radiological loosening. Aseptic loosening was observed in a 93-year-old patient at 5 years after the revision surgery. The femoral defect of the patient who had aseptic loosening was Paprosky type II. Due to lack of complaints, this patient was followed up without surgical intervention. There was no postoperative infection in this series. The survival of the porous-coated cylindrical shaped diaphyseal femoral stem was 98.4% at both 5 and 10 years (Figure 3).

The Kaplan–Meier survival curve for all patients with failure for any reason as the end point.
We couldn’t find any statistical difference among the groups of revision surgery indication in terms of complications and functional scores. However, we observed that periprosthetic joint infections group and elderly patients have some difficulties for ambulation in our cohort.
Discussion
With an increasing number of hip arthroplasties in young patients, the number of revision surgeries is also increasing. Revision hip surgeries are technically challenging procedures even for experienced surgeons. The main problems associated with these procedures are poor bone stock and damaged soft tissues. Although previous studies have reported high failure rates, 8,9 good results have been obtained in recent studies. 6,10 In this series, we achieved excellent results with Echelon stems in terms of stem survival of 98.4% at 5 and 10 years.
Several stem designs and techniques have been described in the literature for femoral component revision surgery, and these techniques can be summarized as follows: surgery with proximally porous-coated femoral components, proximally modular femoral components, extensively porous-coated femoral stems, tapered stems, modular tapered stems, non-modular tapered stems, cemented stem with impaction graft, allograft prostatic component (APC), and mega prosthesis. 7 The femoral component is selected according to the degree of femoral bone loss. Poor survivorship was directly correlated with the degree of preoperative bone. 11 Cylindrical fully porous-coated uncemented femoral components have been associated with predictable long-term fixation for Paprosky types I–IIIa bone loss. 6,7 Type IIIb defects are generally best managed with modular tapered fluted stems; however, some centers have had good long-term results with impaction bone grafting. 12 APC and mega prostheses should be considered part of the armamentarium for managing type IV femoral bone loss. 6,7 All patients in this series were treated with cylindrical fully porous-coated uncemented femoral component (Echelon). The main reasons for choosing this type of extensively porous-coated femoral stem included its strong diaphyseal grip and durability and its ability to prevent subsidence. The Echelon-type prostheses have a long stem that provides good distal diaphyseal fit as required for proximal bone loss.
Waddell et al. from Canada evaluated 392 Echelon stems in primary hip replacements. These authors showed that the Echelon stem survival for revision surgery was 95.2% at a mean of 5.9 years, and the requirement of re-revision was 4.8%. 10 Our result stem survival rate was 98.4% at 10 years.
Another option for femoral stem revision is to use a cemented stem. The main problem with cemented stems is the difficulty of obtaining good cement interdigitation with bone in patients who have thin and sclerotic bones. It also has a higher re-revision rate than cementless stems for revision surgeries in the literature. 4,5,13 –17 In the study conducted by Wang et al., the 5-year survival rates of the cemented and cementless stems were 88.2% and 91.3%, respectively. 18
Bone grafts are utilized frequently in revision hip arthroplasty to compensate for present bone loss. Bone grafts serve two purposes, including mechanical support and osteogenesis. In Paprosky type I defects, the grafts are hardly needed. Type II defects and more severe cases possibly require strut grafts along with allografts. 6 Bone grafts are also used in revision surgery with bone impaction and cemented stems. 12 Strut allografts are used more commonly than cancellous allografts.
Our results showed that all of our patients fell into Paprosky types I–IIIa category, and literature reports have shown that, in these types of patients, cementless stems can be placed in a stable manner, whereas in Paprosky types IIIb and IV femurs, this is not possible, and the use of bone grafts is required. In our series, strut allografts were used in 13 patients to support the femoral shaft. Cancellous bone grafts were used only in three patients. Bone impaction is not preferred to avoid associated complications such as fractures and subsidence. 19 Stem revision is rarely indicated in primary hip prosthesis with cementless stems in the study by Kim. 20 The survival of the primary hip arthroplasty with Echelon stems was reported to be 98.3% in the study by Lewis et al. 21 Similarly, our survival result for Echelon femoral stems for revision surgery was 98.4% at 5 and 10 years.
The main limitation of this study was its retrospective nature, meaning that not all data were available and the patients were at various stages of follow-up, ranging from 3.7 years to 17.1 years, after their revision surgeries.
Conclusions
Femoral bone loss and damaged soft tissues are the main problems in revision hip surgery. Our experience has shown that cylindrical fully porous-coated uncemented femoral components have been associated with good clinical outcomes and survival.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions from the Department of Orthopedics and Traumatology, Istanbul Faculty of Medicine, Istanbul University, Turkey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.