
Abstract
Background
Prosthetic surgery has shown good short-term results with the use of short stems, results comparable with the experience of conventional stems. The aim of this study was to investigate and describe the characteristics and clinical course of patients operated on with the short stem GTS in the medium term.
Methods
Between November 2010 and September 2014, 152 primary hip prostheses were operated on in 142 patients with a mean follow-up of 95.49 months (range 75–120). We analyzed the intraoperative and postoperative complications and the reviews performed during the follow-up.
Results
One intraoperative complications occurred; case in which a femoral calcar fracture occurred and a screw was required during the operation. The clinical evaluation at the end of the follow-up, according to the Merle D’Aubigne Scale, showed the mean value was 17.3684 (SD 0,79472), with a survival at the end of the follow-up of 99.3% of the placed GTS stems.
Conclusions
GTS short stems have shown good results after more than 6 years of follow-up, with comparable results to conventional uncemented stems. Short-stem hip arthroplasty is an advanced way to preserve bone stock while protecting soft tissue
Introduction
Prosthetic hip surgery is today one of the best-performing surgical procedures. There is a survival expectancy of prosthetic implants of more than 90% at 10 years after implantation, both in cemented and uncemented procedures.1,2 This has resulted in younger and younger patients undergoing prosthetic surgery in the hope of improving their quality of life. Finite element studies have shown that there are no problems in fixing the short stems compared to conventional stems. 3 This has led to new prosthetic designs becoming less invasive, respecting the anatomy of the proximal femur as much as possible, in order to improve the quality of the femur at the time of revision surgery. Short stems preserve a greater amount of bone and, due to their biomechanical effect, allow greater compression forces on the lateral column of the femur and reduce stress shielding.4,5 Additionally, they allow the placement of a conventional stem as a rescue in the failure of a short stem.
The GTS® (Zimmer Biomet, Warsaw, USA) stem is based on the concept of tissue preservation surgery, whereby we must not unnecessarily alter the proximal femoral anatomy to achieve stability if we respect it. Stem stability is achieved by : metaphyseal press fit obtained by conical wedge design and compaction of cancellous femoral bone, rotational stability obtained by octagonal elliptical stem cross section, stability and maximized rotary press fit achieved by compression fins longitudinal.
Different studies have been published on the experience of the use of short stems, presenting good short-term results,6–13 comparable to conventional stems,14,15 even with the return to sports activities. 16 However, there is a lack of data in the medium and long term. Some disadvantages of short stems have been reported, such as thigh pain that appeared in 25% of cases between 2–4 years after the intervention and was correlated with the young age of the patients. 17 In other series, proximal cortical hypertrophy was reported in patients operated with short stems between 1.3 and 3.3 years.11,18 Or the appearance of periprosthetic fractures. 2
The objective of our study is to present a series of patients who underwent surgery with the placement of a Global Tissue Sparing (GTS) stem with a mean follow-up of more than six years. We will analyze the results, as well as the differences between the intervened population groups.
Material and methods
In total, 142 patients underwent 152 primary total hip arthroplasties, operated between November 2010 and September 2014, placing a GTS stem. The study was conducted in line with the established ethical guidelines of the hospital: each patient at the hospital was asked to sign an informed consent whether to let his or her data public or private for future access, and only open access medical records were reviewed by the authors of the study. Since this is an observational retrospective study, it does not describe experimental studies on either humans or animals and so it does not need any ethical approval.The GTS stem is made from forged titanium alloy. The stem is available in thirteen sizes and with a standard offset at 133° or lateral offset at 122° for each size. The acetabular component used was an Exceed® Advanced Bearing Technology (ABT) (Zimmer Biomet, Warsaw, USA) hemispherical cup with a 10° E1 polyethylene, to increase the rim cover and a ceramic head.
The indications for these particular implants were: patients up to 85 years of age and suffering from primary osteoarthritis, developmental dysplasia of the hip and avascular necrosis. Contraindications were a body weight of more than 120 kg, severe hip dysplasia (Crowe grade III,IV classification), background of femoral intertrochanteric osteotomy or any other femoral distortion, a cortical index of less than 3, and severe osteoporosis.19,20 All cases underwent preoperative planning.
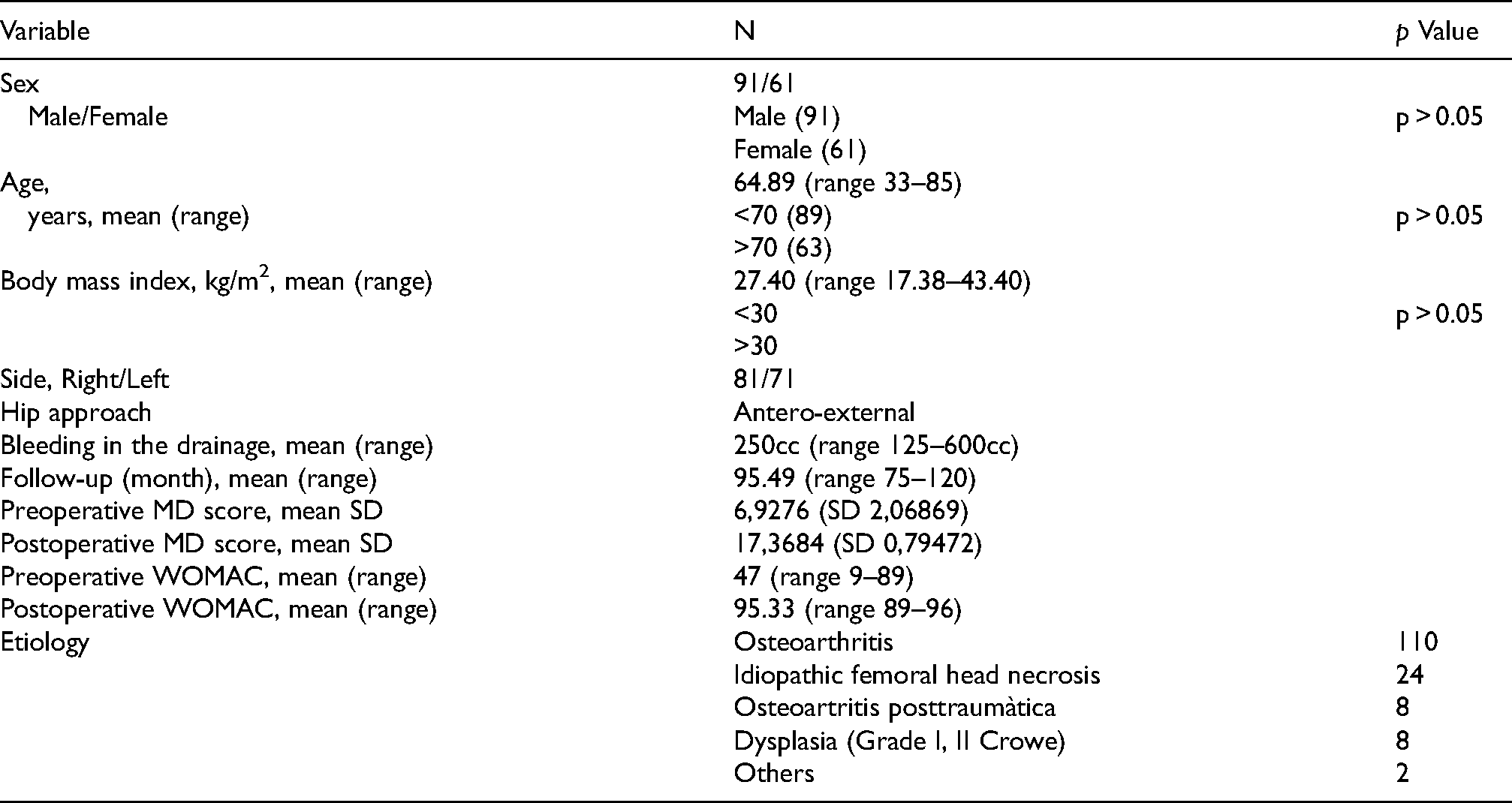
The 152 cases in 142 patients comprised 85 men (6 with prostheses on both hips) and 57 women (4 with prosthetics on both hips) with a mean age of 64.89 years (range 33–85) at the time of the surgery. The mean follow-up was 95.49 months (range 71–120 months). The mean body mass index was 27.40 kg/m2 (range 17.38–43.40). The distribution of patients according to diagnosis was: 110 with primary osteoarthritis of the hip (69.5%), 24 with necrosis of the femoral head (17.96%), 8 with post-traumatic osteoarthritis of the hip (5.46%) 8 with dysplasia Crowe grade II (4.68%) and 2 post-epiphisiolysis cases (2.54%) (Table 1).
Demographics of the cohorts.
All patients were operated on by a single surgeon using a Watson-Jones anterolateral approach. At the time of the operation, these stems, thanks to their design, can be introduced in varus, correcting this varus little by little. We prefer to place them straight directly, thus avoiding varus positioning. Thromboembolic prophylaxis with low molecular weight heparin was performed, as well as antibiotic prophylaxis with Cefazolin 2gr IV in the induction of anesthesia and blood saving protocol with tranexamic acid. In the postoperative period, surgical bleeding and days of hospital admission were analyzed.
Patients were clinically assessed using the Merle d’Aubigné (MD) score preoperatively and at the end of follow-up. The mean preoperative assessment was 6.9276 (SD 2.068669). The radiological evaluation was carried out by means of a standard anteroposterior radiography of the pelvis and lateral hip, verifying the migration, osteolysis and signs of radiolucency, as well as the position of the cup and the position of the femoral stem. 21
Descriptive data are presented as median and range or by mean and standard deviation. Kaplan-Meier estimators with a 95% confidence interval for survival rates were used. The level of significance for all the analyzes performed was established at p ≤ 0.05. Statistical analyzes were performed using SPSS 26.0 (SPP Inc., Chicago, IL, USA).
Results
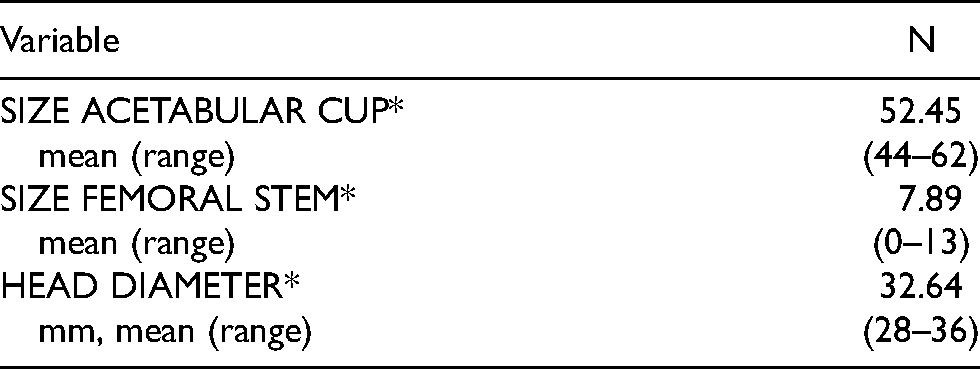
The most commonly used cups were 50 mm diameter in 41 cases and 52 mm in 39 cases. The most commonly used stem size was number 3 in 31 cases and size 1 in 21 cases. The diameter of the femoral head was 32 mm in 81 cases, while the 36 mm diameter was placed in 48 cases and 28 mm in 23 cases (Table 2).
Characteristics of implants.
One intraoperative complications occurred; case in which a femoral calcar fracture occurred and a screw was required during the operation, delaying the patient's recovery for six weeks (Figure 1). There was also a case of postoperative dislocation that was resolved by closed reduction and one case of crural nerve paresis that resolved spontaneously within three months and did not affect the functional recovery of the patient. There were no infections, no vascular problems (Figure 2).
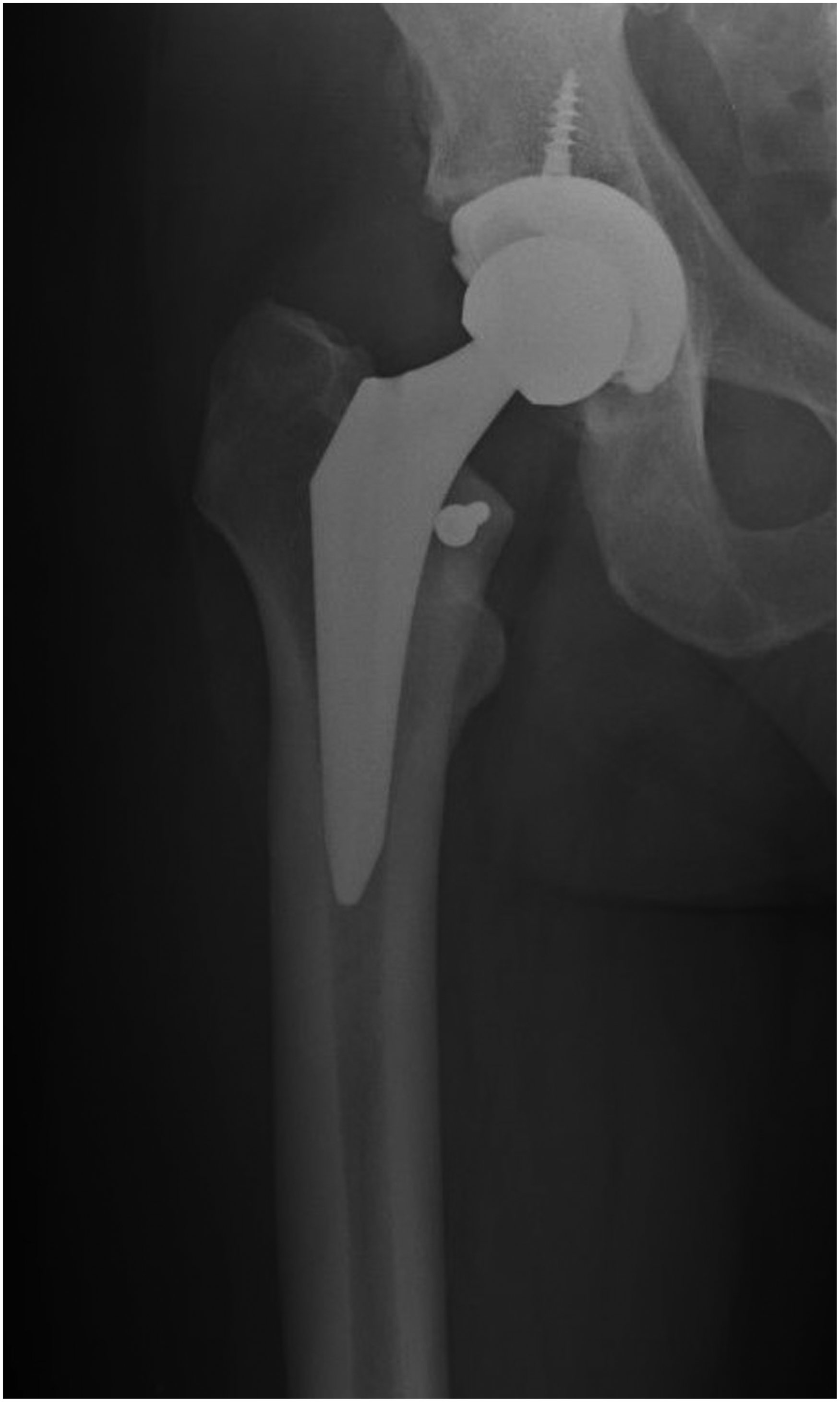
Anteroposterior X-ray, a man of 54 years-old with osteoarthritis of right hip. At 6 years after the intervention with the calcar femoral osteosynthesis.

Anteroposterior X-ray, a man 69 years-old, at 7 years after surgery.
In the postoperative period, a mean bleeding in the drainage of 250cc (between 125–600cc) was registered. Only 6 cases (3.94%) required transfusion. The mean hospital stay was 4.5 days (range 3–7 days). All patients begin sitting, rehabilitation exercises and weight-bearing ambulation the day after the intervention. In the moment of hospital discharge, according to our hospital protocol, 101 patients followed the Home Hospitalization protocol with the assistance of a physiotherapist at home for the first week. 13 patients were transfered to a social health center for recovery and the rest of the cases were discharged home and followed a rehabilitation program in a specialized center.
One postoperative complications occurred; case in which the femoral stem was placed in a non-tolerable varus greater than 5°. In the successive controls an increase in femoral varization was found accompanied by femoral pain. The case was reoperated one year post surgery, replacing the femoral stem and placing a conventional Taperloc® (Zimmer Biomet, Warsaw, USA) stem (Figure 3).

56-year-old man operated, placing GTS stem. (a) One year after surgery with progressive varización femoral stem. (b) Stem revision with convencional stem.
The clinical evaluation at the end of the follow-up, according to the Merle D’Aubigne Scale, showed the mean value was 17.3684 (SD 0,79472), with a survival at the end of the follow-up of 99.3% of the placed GTS stems (Figure 4).
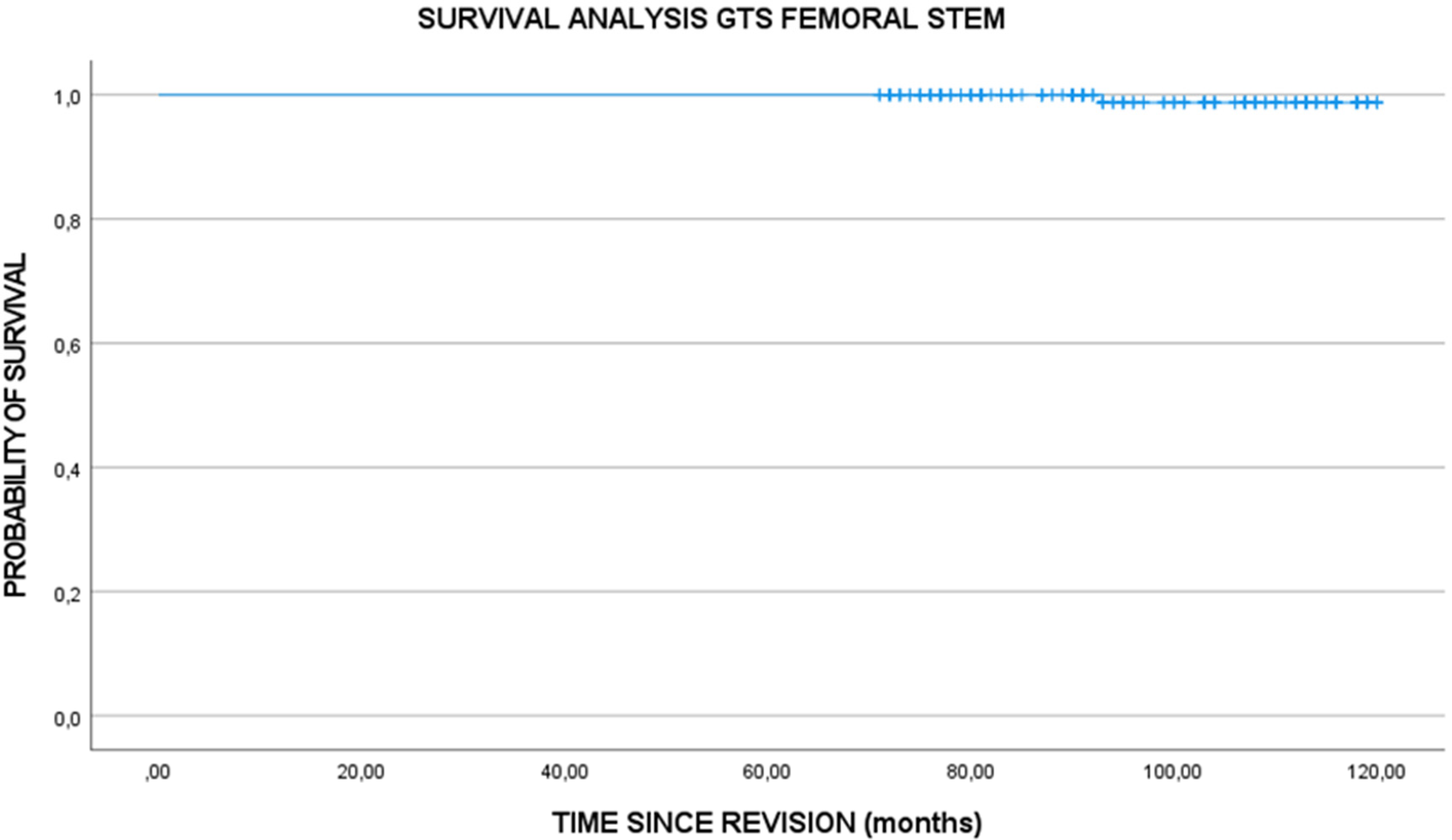
Kaplan-Meier survival curve GTS femoral stem.
The radiographic evaluation at the end of the follow-up showed no subsidence of the femoral stems, there was no osteolysis, no periprosthetic ossification or radiolucencies. The average acetabular inclination was 44° (range 42°–50°). However, there was mild varus in 7 cases (4.60%) less than 5° and one case of varisation greater than 5° that forced the stem to be replaced at 12 months.
Discussion
The use of short stems in hip replacement surgery is based on two concepts: the philosophy of bone tissue conservation and the biomechanical concept of load transfer in the lateral femoral stem. Recent studies have confirmed the excellent clinical and radiographic results with positive periprosthetic bone remodeling of shorts stems in the short term. The absence of pain in the thigh, the disappearance of stress shielding and the recovery of the system suggest an optimal load transfer in short stems.
The success of short uncemented stems is due to osseointegration of the implant. The prerequisite is primary stability. 5 This stability should prevent both stem sinking and rotation. Some finite element studies have stated that cementless short stems should decrease migration and subsidence, improving the stability of femoral implants. 3 In GTS stems, stability is provided by the press-fit metaphyseal design. This is achieved by the conical wedge shape and compaction of the cancellous femoral bone. Rotational stability is achieved by the elliptical cross section of the octagonal bar and the maximized rotational stability obtained by the longitudinal press-fit of the compression fins.
There are several published series of short stems that report good short-term clinical results, but the medium and long-term results remain unknown. In our series at 120 months of follow-up, we have had a good clinical result with a 120-months survival of 99.3% (Figure 4). In fact, we only had one patient who had to have the stem replaced at 12 months due to progressive stem varization (Figure 3). These results are comparable to other series of conservative stems and series of conventional uncemented stems.6–12 However, we are aware that there is still a lack of longer-term published series on the results of the short stems. 22
Tolerance to varus when positioning the femoral stem has been widely discussed. 8 Our experience has shown us that stems placed in less than 5° varus are totally acceptable, while a positioning greater than 5° can produce a progressive increase of the varus with femoral pain that requires revision of the stem. This is just what happened to us in one case. 8 Another type of complication is the peri-prosthetic fracture, already referenced in the literature.8,23 In our series we had a case, at the beginning of the series, of a peroperative femoral calcar fracture that was resolved with the placement of a screw at this level. This can be related to the learning curve in the use of short stems. It is evident that there is a certain learning curve with respect to the adequate size and positioning of the short stem, especially for young and inexperienced surgeons. 24 The follow-up of the patients in our series has not demonstrated subsidence of the stems or radiolucencies at the end of the follow up.
The indication for short stems like the GTS stem is not limited to young patients. It is suitable for all types of femur morphology and any age. The use of the short stems would only be contraindicated in patients with osteoporotic bone.12,17,18 The wide ranges of stem sizes allow it to be used on all types of femurs. Statistical analysis of the results of patients under 70 years and older than 70 years has not shown significant differences (p > 0.05) and it is shown that there is no contraindication in the use of short stems only due to age.25–27
The surgical technique differs in some common technical aspects. The femoral neck is cut obliquely as usual. It is not necessary to cut perpendicularly as required in other short stems, because our stem allows us to reach the upper part of the femoral canal and orient ourselves correctly. However, it is necessary to perform the varus entry with the scraper launcher to exploit the spongy metaphyseal cushioning support and leverage in the outer cortex of the femur. This entry should progressively correct the placement of the varus to avoid the stem in excessive varus. This technique makes it easy and reproducible. 27
Subsidence of the short femoral stem is one of the greatest concerns in surgeons. 7 We have used the measurement between the lesser trochanter to the tip of the placed femoral stem as a reference. In our series, subsidence has not occurred and is due to the design of the stem.
One of the problems that have been mentioned in the other series of short stems has been the existence of diaphyseal cortical hypertrophy.7,10 Meier reports in his series an incidence of 63% of the appearance of cortical hypertrophy, but with an excellent clinical result. 28 For Cho, this appearance is usually accompanied by thigh pain. 29 However, these authors recommend some caution in longer-term clinical outcomes. In the case of our series with the GTS stem, we have not had any case of cortical hypertrophy or femoral pain.
Other aspects of the clinical follow-up in our series were operative bleeding and hospital stay. We found had a mean blood pressure loss of 255cc (range 125–600cc). Iin only six cases ((3.94%) it was necessary to perform a transfusion, a result comparable to other series of conventional stems. 16 This result is due to the hospital protocol for saving blood in prosthetic surgery. This protocol improves preoperative hemoglobin and the use of peroperative tranexamic acid, recommended by Clavé in short stem surgery. 30 We have noticed more blood loss in men than in women and more in young people than in older people of over 70 years, although there is no statistical significance in any of the cases. This can be attributed to the greater muscle mass.
Regarding hospital stay, we have had a mean hospitalization stay of 4.5 days (range 3–7 days), which is comparable to other series. 16 Our results are due to the protocol of the hospital of Home Hospitalization, which allows us to monitor patients at home, both by the nursing staff and the physical therapists during the first days after hospital discharge. To achieve these results, we hold a preoperative information session for patients and families. We are sure that these results can still be improved with the use of the rapid recovery that we currently implemented.
Conclusions
GTS short stems have shown good results after more than 6 years of follow-up, with comparable results to conventional uncemented stems. Short-stem hip arthroplasty is an advanced way to preserve bone stock while protecting soft tissue. This not only allows for a quick recovery and a satisfactory rate of return to sports and daily activities after surgery, but is also the cornerstone for a simplified revision surgery after implant failure for the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.