
Abstract
Background:
The direct anterior approach has gained popularity in total hip arthroplasty (THA) over the past decade. However, there are few reports that describe the use of this approach for cases of complex revision. The purpose of this study was to report the surgical procedure and early clinical results of acetabular revision in the presence of bone defects using a Kerboull-type reinforcement device through the direct anterior approach.
Methods:
Eleven patients who had undergone acetabular reconstruction using a Kerboull-type reinforcement device for aseptic or septic loosening bone defects were enrolled. All procedures were performed using the direct anterior approach on a standard operating table. The mean age was 71.8 years, the mean period from initial surgery to revision THA was 14.5 years, and the mean follow-up period was 19.8 months.
Results:
The Kerboull-type acetabular reinforcement device with cemented cup combined with allogenic femoral head bone grafts was used in all hips. The mean operative time and intraoperative blood loss were 148 min and 743 g, respectively. None of the patients required allogeneic blood transfusion. One patient required revision surgery 11 months postoperatively because of device displacement. No other major or minor orthopedic complications were observed.
Conclusion:
The direct anterior approach allows for less invasive acetabular reconstruction using a Kerboull-type reinforcement device.
Keywords
Introduction
The direct anterior approach for total hip arthroplasty (THA) has gained popularity over the past decade as a minimally invasive approach through the interneural interval. 1 –3 The surgical procedure using the direct anterior approach for simple primary THAs has been well established 1 –3 and systemic reviews have revealed early functional recovery compared to other approaches. 4,5 However, complex revision THA through this approach is considered to be a challenging procedure and there is a limited number of reports on the outcomes of this approach in complex revision cases.
The management of large acetabular bone defects is a challenging problem in revision THA. Several techniques have been proposed for managing acetabular defects without bone grafting, including the acceptance of a high socket center using cementless cups, 6,7 oversized sockets, 6,8 and prosthetic augmentation. 9,10 However, bone grafting appears to be an effective option for biological reconstruction of bone defects because sufficient grafting makes it possible to bring the acetabular components into the original position of the acetabulum 11 and recovery of the bone stock is preferable to surgical options after taking further revision surgery into account. Acetabular reinforcement devices are recommended with bulk bone grafting 12 because high failure rates of acetabular revision surgery using bulk allografts without reinforcement devices have previously been reported. 13 To date, conventional direct lateral or posterolateral approaches have been widely used for acetabular revision using reinforcement devices to obtain a good surgical view. 14 –16
Among the several types of reinforcement devices available for acetabular reconstruction, the Kerboull-type acetabular reinforcement device is effective and has preferable mid- to long-term results. 14 –16 We have used the Kerboull-type acetabular reinforcement device with cemented cup combined with allogenic femoral head bone grafts for acetabular revision with bone defects through the direct anterior approach since 2014. The purpose of the present study was to report the surgical technique and the preliminary results of acetabular revision using the Kerboull-type reinforcement device through the direct anterior approach.
Patients and methods
Patients
The Kerboull-type acetabular reinforcement device combined with allogenic femoral head bone grafts was used for revision of acetabular components following previous THA in 13 hips of 13 patients between July 2014 and February 2017. Of those 13 patients, 2 patients who had undergone primary THA for secondary osteoarthritis following severe pelvic fracture were excluded. The remaining 11 patients who underwent acetabular cup revision using the device for aseptic or septic loosening were enrolled in this study. We retrospectively assessed the medical records of these patients. They were all women. The mean age was 71.8 ± 10.9 years (range 49–91 years). Mean weight, height, and body mass index were 55.4 ± 10.5 kg, 150.5 ± 6.3 cm, and 24.5 ± 4.1 kg/m2, respectively. The mean duration from initial surgery to the present procedure was 14.5 ± 9.0 years (range 0.5–26 years). Six of the 11 patients had already undergone acetabular component revision once or more following failed acetabular revision. In these six patients, the mean duration from first revision surgery to the present procedure was 18.7 ± 20.9 months (range 1–48 months). No patient was lost to follow-up and the mean follow-up period was 19.8 ± 10.2 months (range 10–42 months).
Acetabular defects were classified using the Paprosky system. 17 Of the 11 hips enrolled, 2 hips (18%) had a type-2A defect with superomedial bone loss (Figure 1(a)), 1 hip (9%) had a type-2C defect with medial wall loss (Figure 1(b)), 3 hips (27%) had a type-3A defect with superior migration of the femoral head of more than 3 cm (Figure 1(c)), and 5 hips (45%) had a type-3B defect with a risk of pelvic discontinuity due to severe superomedial migration of the femoral head and extensive medial wall loss (Figure 1(d)). All patients had cementless acetabular cups. Nine patients had cementless stems and two patients had cemented stems. On the femoral side, focal osteolysis was observed in the proximal femur in five hips (45%) and Engh’s 18 grade 2 to 3 stress shielding was observed in seven hips (64%).
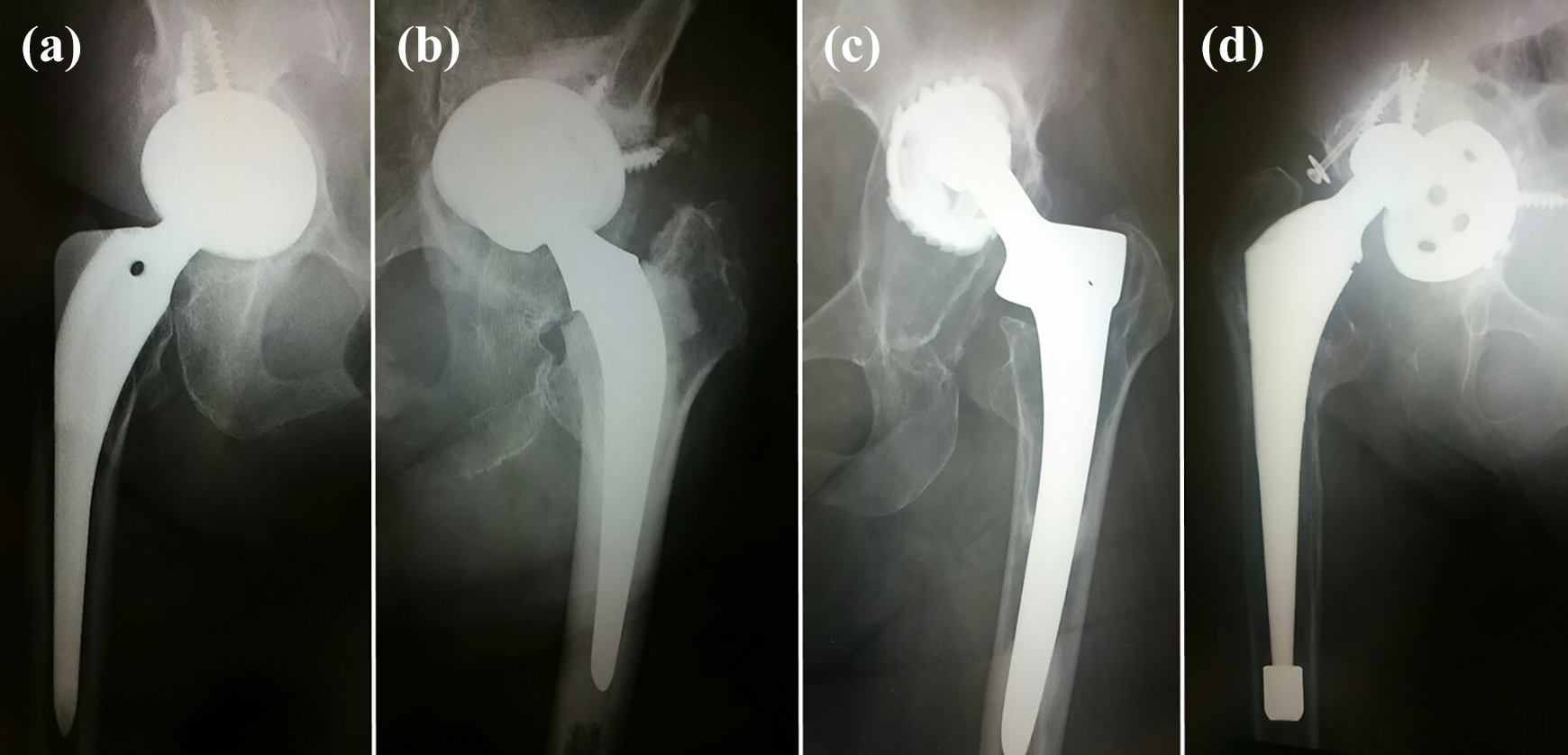
Preoperative X-ray showing aseptic acetabular loosening in four hips. (a) The right hip of a 75-year-old female with type-2A defect. The cup migrated superomedially. (b) The left hip of a 91-year-old female with type-2C defect. The cup migrated superomedially with medial wall loss. (c) The left hip of a 62-year-old female with type-3A defect and severe superior migration of the cup. The medial wall was preserved. (d) The left hip of a 78-year-old female with type-3B defect and severe superomedial migration of the cup. There was extensive loss of the medial wall.
Surgical technique
The direct anterior approach was used in all hips regardless of the previous surgical approach with the patients in the supine position on a standard surgical table. 3 The skin incision was started 2 cm lateral and 2 cm distal to the anterior superior iliac spine and followed the anterior border of the tensor fasciae latae muscle. The length of the incision ranged from 8 cm to 10 cm depending on body size or degree of femoral head migration. Compared to standard primary THA, the incision was slightly extended proximally as needed. The fascia of the tensor fasciae latae muscle was incised in line with the muscle running course with the incision approximately 2 cm away from the anterior border of the tensor fasciae latae to avoid damage to the lateral femoral cutaneous nerve. Blunt dissection was performed along the medial side of the tensor fasciae latae muscle. The tensor fasciae latae muscle was retracted laterally and the sartorius and rectus femoris muscles were retracted medially to expose the hip capsule. The capsule was removed as much as possible to obtain working space to remove the acetabular components and mobilize the proximal femur. Placing the hip in an abduction and internal rotation position allowed the surgeon to remove the lateral portion of the capsule easily and the external rotation position (figure-four position) allowed the surgeon to remove the medial and inferior portions of the capsule easily. After achieving mobilization of the proximal femur, the femoral head was disconnected and removed.
In cases of femoral revision, a retractor was placed behind the greater trochanter to elevate the proximal part of the femur and the operating table was bent at the location of the hip joint to allow hip hyperextension of approximately 20°. Then, the stems were retrieved through the femoral neck.
For the acetabular procedure, a retractor was placed behind the posterior wall of the original acetabulum to retract the proximal part of the femur, including the neck of the femoral stem posteriorly, and identify the posterior rim of the original acetabulum. Placing the hip in the adduction and flexion position (placing the leg on the contralateral leg) allowed the surgeon to retract the femoral neck behind the retractor easily. After removal of the inferior capsule, fibrous tissue, and osteophytes, the superior border of the obturator foramen could be identified. Following total removal of the acetabular components, the acetabulum could be visualized well using four retractors and the orientation of the acetabulum was observed carefully and bone defects evaluated. Reaming was performed into the original acetabulum with careful attention to avoid damage to the anterior and posterior walls. For hips with large superior defects of the acetabulum, reaming was performed 10–15 mm superiorly to the original acetabulum. Femoral head allografts, either morselized or structural, were used for acetabular bone defects. In cases with large medial or superior defects, structural bone grafting was performed. Then, the morselized graft was packed into the gaps between the structural grafts and host bone and into the other cavity defects. The Kerboull-type reinforcement device has various sizes and vertical offsets. We placed the acetabular cup as close as possible to the original acetabulum. In cases of severe migration of the femoral head, a high-placement-type device (offset of 10 or 15 mm) was choosen if required. The device was fixed with at least two screws through the rounded plate of the device and bone graft before engaging the host bone (Figure 2). We used intraoperative X-ray to confirm appropriate placement of the inferior hook of the device on the superior edge of the obturator foramen (Figure 3). In cases with inferior acetabular osteophytes, the osteophytes sometimes prevent appropriate placement of the inferior hook; therefore, careful attention should be paid to removal of the osteophytes. Finally, a polyethylene component was inserted into the device and fixed with cement taking pelvic tilt into consideration. With a trial femoral head attached, the leg length and hip stability were checked. Then, the selected femoral head components were attached and the hip was reduced. Following intra-articular administration of 1000 mg of tranexamic acid, the fascia and skin were closed with absorbable sutures. We did not use drains in any patient.

Intraoperative photograph of the left hip. The retractors were inserted on the posterosuperior aspect of the acetabulum (A), anterior wall (B), superior edge of the obturator foramen (C), and posterior wall (D). The inferior hook of the device (*) was inserted at the superior edge of the obturator foramen, which was held by the retractor (C). The device was fixed using three screws passed through the plate and bulk bone graft (BG) before engaging the host bone. Med: medial; Sup: superior.

Preoperative (a), intraoperative (b), and postoperative (c) X-rays of a 61-year-old female who underwent acetabular revision. (a) Preoperative X-ray showing type-3A defect. The cup migrated superolaterally. (b) Intraoperative X-ray showing appropriate placement of the inferior hook of the device. The hook was held by a retractor, which was inserted at the superior edge of the obturator foramen. The proximal femur, including the femoral neck of the stem, was rotated externally and retracted posteriorly. (c) The acetabulum was reconstructed using the reinforcement device with 15 mm of vertical offset. The bony defects were filled with both morselized and structural allogenic bone graft. Two screws perforated the structural allogenic bone graft and were fixed to the host bone tightly.
Postoperative management
Full weight-bearing was allowed for patients with type-2A, 2C, and 3A defects on the first day. In patients with type-3B defects, partial weight-bearing was allowed on the first day. Then, over the first month, the patient progressed to full weight-bearing. Both active and passive motion exercises of the involved joint were allowed immediately after surgery. The patients were instructed to avoid deep hip flexion with internal rotaion and hyperextension with external rotation during the first 3 weeks to prevent early dislocation, after which no precautions were taken.
Results
Isolated acetabular component revision was performed in nine hips. The remaining two patients underwent both acetabular and femoral revision. The mean operative time was 148 ± 43 min (range 103–246 min). The mean intraoperative blood loss was 743 ± 405 g (range 200–1600 g). Intraoperative blood salvage was performed in eight patients (73%) and all collected blood was returned to each patient immediately after surgery. Serum hemoglobin level was decreased from 11.8 ± 1.7 g/dl preoperatively to 9.9 ± 1.7 g/dl on postoperative day 1. None of the patients required allogeneic blood transfusion. The allogenic bone grafts harvested from the femoral heads, both morselized and structural, were used in all hips. We used devices with no vertical offset in seven hips (64%) and vertical offset of 10 mm in one hip (9%) and 15 mm in three hips (27%). The diameter of the cemented cups used was 44 mm in two hips (18%), 48 mm in eight hips (73%), and 52 mm in one hip (7%). We used 28-mm and 32-mm diameter femoral heads in five (45%) and six hips (55%), respectively.
Postoperative radiographic analysis showed the vertical distance from the inter-teardrop line to the femoral-head center was 21.5 ± 5.8 mm. The vertical leg lengthening in the present procedure was 17.0 ± 12.2 mm. The leg length discrepancy was decreased from 14.9 ± 12.0 mm preoperatively to 2.2 ± 11.3 mm postoperatively.
As a complication, displacement of the device with acetabular components was observed in one hip (9%). This case was a 79-year-old female with a type-3B acetabular defect. Postoperative X-ray revealed inadequate placement of the inferior hook of the device to the superior edge of the obturator foramen due to inferior osteophytes. Anterior rotation of the device progressed gradually and finally, the anterior support of the device was broken 11 months postoperatively. She underwent rerevision surgery. In the remaining 10 hips (90%), both acetabular and femoral components remain stable at the latest follow-up. In three hips that underwent the present procedure as one-stage revision for septic loosening, exacerbation of infection has been not detected in any patient at a mean follow-up of 20.0 months. There were no other local or systemic major complications such as dislocation, periprosthetic fracture, venous thromboembolism, femoral or sciatic nerve palsy, or lateral femoral cutaneous nerve neurapraxia.
Discussion
The Kerboull-type acetabular reinforcement device is manageable for the direct anterior approach. Even in the presence of severe acetabular bony defects, retrieval of the old acetabular components, structural or morselized allogenic bone grafting, and placement of the device could be performed less invasively through the single anterior incision. To date, direct lateral or posterolateral approaches have been widely used for acetabular revision with this device to obtain a good surgical field for operation. 14 –16 The direct anterior approach had been considered as an approach that is limited to primary arthroplasty. Only in recent years, interest and enthusiasm have emerged for the anterior approach whether complex revision is indicated or not, and several authors have focused on extension of this approach proximally 9,19 or distally 20,21 and on the anatomy of the surrounding structures involved in the direct anterior approach. 20,21 However, to our knowledge, there is no report on surgical outcomes of revision THA through the direct anterior approach using reinforcement devices for hips with large acetabular bone defects.
The direct anterior approach is a reasonable approach for acetabular reconstruction. While the femoral procedure sometimes remains problematic, the strength of this approach is the acetabular procedure. 22 This approach offers easy access to the acetabulum without detaching the abductor muscles and a good view of this area; therefore, acetabular reconstruction using bone grafts and reinforcement devices can be performed without difficulty. Moreover, the direct anterior approach decreases the need for postoperative restriction of weight-bearing or precautions to avoid postoperative dislocation.
In this series, we experienced failed acetabular reconstruction using the device in only one hip (9%). We considered that inappropriate placement of the inferior hook resulted in failure, that is, a technical failure. Inferior osteophytes of the acetabulum can prevent appropriate placement of the inferior hook and identification of the superior edge of the obturator foramen; therefore, careful attention should be given to osteophyte removal. Besides, the patient had a severe anterior column defect. Extension of the approach proximally and reconstruction of the anterior column using allografts 23 or hardware 13 could be used as an alternative option in such cases.
An important limitation of this study was the small sample size and short follow-up period. We began to use this device in combination with allografts for acetabular reconstruction in 2014. Therefore, these results should be considered as preliminary. However, the preferable implant placement and minimally invasive aspect of this procedure promise good mid- to long-term outcomes.
In conclusion, the direct anterior approach allows for less invasive acetabular revision using a Kerboull-type reinforcement device. The device is manageable for acetabular revision through the direct anterior approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.