
Abstract
Purpose: One of the major problems in revision total hip arthroplasty (THA) is severe acetabular bone loss. The aim of our study was to evaluate the clinical outcomes of revision THA using a Kerboull-type reinforcement device (KT plate) and allogeneic structural bone graft. Methods: This retrospective study evaluated 48 hips that underwent revision THA using a KT plate and allogeneic structural bone graft between 2008 and 2016, with a median follow-up of 6.2 years (range 3–12.6 years). Functional outcome was assessed using the Japanese Orthopaedic Association (JOA) hip score. Postoperative and follow-up radiographs were compared to assess migration and breakage of the implant. Results: The mean JOA hip score improved from 45.6 (±16.3) points before surgery to 72.1 (±11.9) points at the most recent follow-up examination (p < 0.001). Two hips (4.2%) underwent re-revision THA because of cup loosening due to breakage of the KT plate. A total of 13 hips (27.1%) were classified as radiological failures. Binomial logistic regression analysis showed that a Kawanabe classification of stage 4, which indicates massive bone defects in the weight-bearing area, was a risk factor for radiological failure (odds ratio: 4.57; 95% confidence interval: 1.01–26.35). Conclusions: A KT plate with an allogeneic structural bone graft is a useful method of acetabular reconstruction in revision THA that restores bone stock and improves hip function. Our findings indicated that a Kawanabe classification of stage 4 was a risk factor for radiological failure of the implant.
Keywords
Introduction
The number of total hip arthroplasty (THA) procedures performed annually is projected to increase each year through 2030, 1 with a corresponding increase in the number of revisions. 2 One of the major problems in revision THA is severe bone loss in the acetabulum. Acetabular bone loss has traditionally been treated with bone grafting and the addition of a reinforcing ring or a specially designed cage. 3 Studies evaluating recent implant designs have also reported good results with the addition of porous metal augmentation.4,5 Each reconstruction method has its advantages and disadvantages. 6
Tanaka et al. 7 introduced the Kerboull-type acetabular reinforcement device (KT plate, Kyocera, Osaka, Japan), which is a modified version of the original Kerboull acetabular reinforcement device. 8 The KT plate has been proven to support bone grafting, restore bone defects, and provide a good long-term survival rate as a reconstruction method in patients with acetabular defects.8–13
Implant survival after revision THA is affected by multiple factors. Although some studies have evaluated risk factors for failure of revision THA with a KT plate, these risk factors have not been clearly identified. In addition, most of these studies have included both primary and revision THA, or have included cases in which artificial bone or morcellated bone grafts were used.7,11,14,15 Because there are reports of poor results with artificial bone and morselized bone grafting,14,15 we use allogeneic structural bone grafting in the weight-bearing area in all cases. To the best of our knowledge, there are few studies that have evaluated only patients undergoing revision THA with allogeneic structural bone grafting.
We hypothesized that the risk factors for failure existed in all cases of revision THA using a KT plate and allogeneic structural bone grafting. The aim of our study was to evaluate the clinical outcomes of revision THA using a KT plate and allogeneic structural bone graft and determine the risk factors for radiographic failure.
Materials and methods
Patient data
Patients’ demographic data (n = 48).

Data are presented as n (%), median (range), or mean ± standard deviation.
Surgical procedure
THA was performed via the posterior approach with the patient in the lateral position. An allogenic bone graft was used in all included patients. The graft bone was obtained from the femoral head of osteoarthritic patients during the previous primary THA, and was re-sterilized using a thermal processing method (Lobator sd-2; Telos, Marburg, Germany) and stored at −80°. These procedures were performed in accordance with the guidelines of the Japanese Orthopedic Society. The KT plate placement was based on the technique described by Kerboull
8
; the hook of the KT plate was placed under the teardrop, and screws were passed through the pallet of the KT plate and fixed to the host pelvis. A structural bone graft was added for bone defects in the weight-bearing area. Additionally, morselized bone was packed into the gaps between the structural bone graft and host bone. The all-polyethylene cup was fixed with bone cement (Figure 1). The KT plate has various types of offsets and vertical lengths. Using the high hip center type of KT plate has the advantage of reducing the amount of bone grafting required in the weight-bearing area due to the large area of the pallet in contact with the acetabulum. For this reason, we used the high hip center type of KT plate in 45 of 48 cases (93.8%). In cases where the KT pallet could not be attached directly to the host pelvis due to a bone defect in the weight-bearing area, all screws were fixed to the pelvis via a structural bone graft. Partial weight-bearing was commenced immediately after surgery, and full weight-bearing was possible at 4–6 weeks after surgery in all cases. Anteroposterior radiographs of a 70-year-old woman who underwent hemiarthroplasty for femoral neck fracture 8 years ago. (a) At the time of revision THA, there is hemiarthroplasty migration due to septic loosening, with an AAOS type III defect. (b) Immediately after revision THA using a high hip center type of KT plate and allogeneic structural bone graft, the severity of the bone defect in the weight-bearing area is classified as Kawanabe stage 4. (c) At 7 years after revision, there is no implant migration or breakage. The graft bone has not collapsed and is remodeled. THA, total hip arthroplasty; AAOS, American Academy of Orthopedic Surgery; KT plate, Kerboull-type acetabular reinforcement device.
Postoperative evaluation
Hip function was evaluated using the Japanese Orthopaedic Association (JOA) hip score. The JOA hip score is a 100-point scale that comprises the subcategories of pain (0–40 points), range of motion (0–20 points), ability to walk (0–20 points), and activities of daily living (0–20 points). The maximum total JOA score for a normal hip is 100 points, with higher scores indicating better function. The JOA hip score was evaluated preoperatively and at final follow-up.
During surgery, the acetabular defect was classified using the American Academy of Orthopedic Surgery (AAOS) grading system. 16 Each AAOS classification is categorized as type I segmental defect (peripheral, central), type II cavitary defect (intact rim: peripheral, central), type III combined defect, or type IV pelvic discontinuity.
Postoperative and follow-up radiographs were compared to assess migration of the implant. In accordance with previous studies,8,17 radiological failure was defined as the presence of any of the following criteria: 1) acetabular revision due to aseptic loosening, 2) breakage or loosening of the screw or device, and 3) movement of the center of the implant femoral head by more than 5 mm due to horizontal or vertical migration, or an inclination of the KT plate of more than 5°.
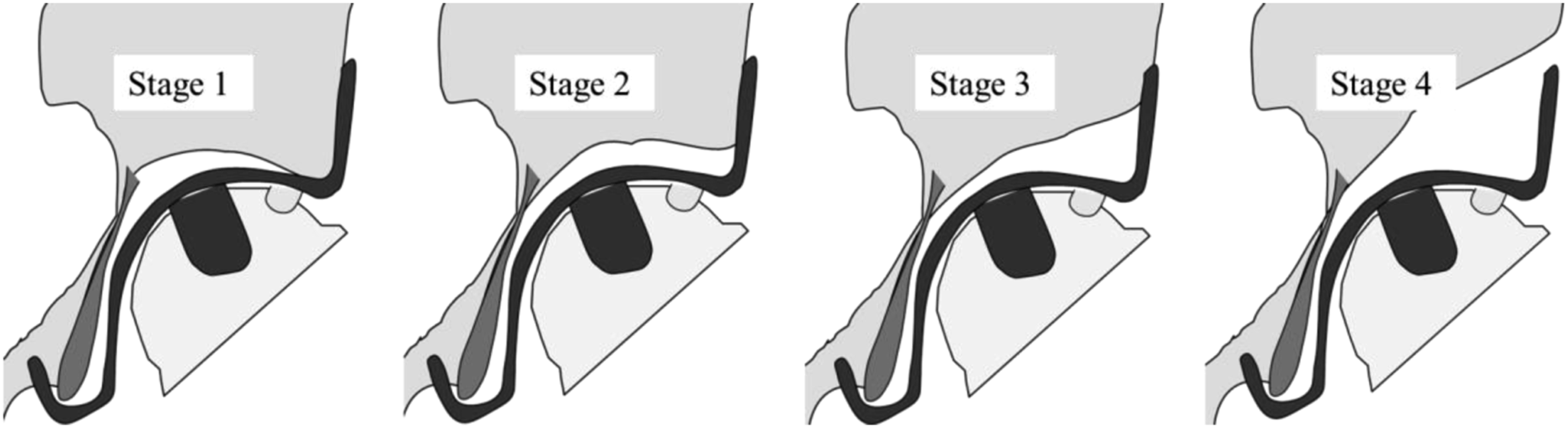
The Kawanabe classification was used to grade the acetabular bone defect according to the severity of the superior segmental bone loss.
14
Stage 1 indicates no superior bone loss, with the whole pallet of the KT plate placed against the host bone. Stage 2 indicates superior bone loss, with more than 50% of the pallet in contact with the host bone. Stage 3 indicates superior bone loss, with less than 50% of the pallet touching the host bone. Stage 4 indicates massive bone loss, with no part of the pallet touching the host bone (Figure 2). Kawanabe classification based on the amount of contact between the pallet of the Kerboull-type acetabular reinforcement plate and host bone.
14
Variables
We assessed the following clinical characteristics that have previously been suggested to affect the outcomes of interest.15,17–19 The assessed patient-related factors were sex, age, body mass index, primary disease, septic loosening, duration of follow-up, pre- and postoperative JOA scores, and a preoperative AAOS classification of III or IV. The assessed surgery-related factors were the inclination angle of the KT plate, Kawanabe classification of stage 4, incidence of radiological failure, and the use of a high hip center type of KT plate.
Statistical analysis
Data are presented as the mean and standard deviation for normally distributed values, and as the median and range for non-normally distributed values. Continuous data were analyzed using the Student’s t-test or Wilcoxon rank sum test according to their distribution, while categorical data were analyzed with the chi-squared test or Fisher’s exact test. Multivariate analysis was performed to adjust for potential confounders. Results were summarized as odds ratios, 95% confidence intervals, and p values. p < 0.05 was considered statistically significant. All statistical analyses were carried out using JMP pro 15.2.1 (SAS Institute, Cary, NC, USA).
Ethics approval and consent to participate
The study protocol was approved by the institutional review board our institution (no. 210158) and was performed in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients provided written informed consent for the publication of their medical data.
Results
The AAOS classification was type II in eight hips (16.7%), type III in 39 hips (81.3%), and type IV in one hip (2.1%). The Kawanabe classification was stage 1 in one hip (2.1%), stage 2 in 15 hips (31.3%), stage 3 in 11 hips (22.9%), and stage 4 in 21 hips (43.8%). The mean JOA hip score significantly improved from 45.6 (±16.3) points before surgery to 72.1 (±11.9) points at the most recent follow-up examination (p < 0.001).
The screw or KT plate was broken in three hips, and 10 hips developed substantial migration of the KT plate. Therefore, 13 hips (27.1%) had radiological failure based on our criteria. Two hips (4.2%) underwent re-revision for cup loosening due to breakage of the KT plate at 5 years (Figure 3) and 6.5 years postoperatively, respectively. Another hip had KT plate breakage observed at 3.6 years postoperatively, but there was no subsequent cup loosening. Anteroposterior radiographs of a 74-year-old woman who underwent THA for osteoarthritis 14 years ago. (a) At the time of revision THA, there is aseptic cup loosening with an AAOS type III defect. (b) Immediately after revision THA using a 10-mm high hip center type of KT plate and allogeneic structural bone graft, the severity of the bone defect in the weight-bearing area is classified as Kawanabe stage 4. (c) At 5 years after revision, there is cup loosening due to breakage of the KT plate. Re-revision THA was performed using a 15-mm high hip center type of KT plate and allogeneic bone graft. (d) At 5 years after re-revision, there is no implant migration or breakage. The graft bone is not collapsed and is remodeled. THA: total hip arthroplasty; AAOS: American Academy of Orthopedic Surgery; KT plate: Kerboull-type acetabular reinforcement device.
Comparison of variables between the stable and radiological failure groups.

Data are presented as n, n (%), median (range), or mean ± standard deviation.
AAOS, American Academy of Orthopedic Surgery; JOA, Japanese Orthopaedic Association; KT plate, Kerboull-type acetabular reinforcement device.
*p < 0.05.
Binomial logistic regression analysis of the risk factors for radiological failure.

Coefficient of determination (R2) = 0.17.
CI, confidence interval.
*p < 0.05.
Discussion
Several reports have shown that the risk of implant failure after revision THA with a KT plate is increased by various factors, including artificial bone grafting, 15 morselized bone grafting,14,17 inclination angle of the KT plate17,19 and AAOS type IV. 15 In the present study, the risk factor for radiological failure of revision THA using a KT plate and allogeneic structural bone graft was a Kawanabe classification of stage 4. Our findings suggest that understanding the location and size of bone defects is an effective approach to prevent implant failure.
Kawanabe et al. 14 reported that the 10-years survival rates for radiological failure of structural and morcellated bone grafting in revision surgery using the Kerboull acetabular augmentation device were 82% and 53%, respectively, and proposed the Kawanabe classification to address the use of bulk bone grafting around the plate. Furthermore, a finite element model analysis revealed that in patients with massive acetabular defects, the use of bulk bone grafting was effective in reducing the stress on the KT plate and screws compared with the use of a morselized bone graft alone. 20 Based on these reports, we use structural bone grafting around the plate area in all cases. Makita et al. 18 reported favorable results for revision THA using a bulk allograft and the Kerboull reinforcement device, and reported that the presence of a Kawanabe stage 4 defect significantly influenced the long-term results of revision THA. These findings are consistent with our results, although Makita et al. 18 used the original Kerboull reinforcement device. Masumoto et al. 17 reported that the high hip center type of KT plate resulted in poorer survival compared with the original cup center type of KT plate. In contrast, our study and Kamada et al. 19 found that the two types of KT plates had similar rates of radiological failure. However, although structural allogeneic bone grafts are reported to consolidate in the short term, 18 another study reported failure in the long term. 21 The use of the high hip center type of KT plate might effectively reduce the volume of the bone graft. Our study also suggests that the KT plate with an allogeneic structural bone graft is a useful acetabular reconstruction method in revision THA; however, patients with massive bone defects might require other options or techniques.
Our study has several limitations. First, it was a retrospective analysis rather than a randomized controlled trial, so there was bias due to unmeasured factors. Second, the cohort size was small because only revision cases were included. Third, the follow-up period was relatively short, and a longer follow-up may have been necessary. Fourth, we did not examine whether the femur was revised.
One of the strengths of our study is that although previous studies have evaluated the use of structural bone grafting and a KT plate, there are few studies of only revision THA with allogeneic bone grafting. The surgical procedure differs between primary and revision THA. Furthermore, primary THA mainly involves autologous bone grafts, so the strength and remodeling cannot be compared with allogeneic bone grafts. 22 Our study evaluated the results of revision THA performed without autologous bone or artificial bone grafts. Another strength of our study is that few studies have focused on the Kawanabe classification and reported radiological failures. The Kawanabe classification is based on the severity of bone loss around the plate area. We believe that the shape and stiffness of the bone grafted in this weight-bearing area has important effects on the outcome. Addressing these issues benefits both patients and physicians involved in the increasing number of THA revision procedures in recent years.
Conclusion
The use of a KT plate with an allogeneic structural bone graft is a useful acetabular reconstruction method in revision THA that restores bone stock and improves hip function. Our findings indicated that a Kawanabe classification of stage 4 was a risk factor for radiological failure of the implant.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.