
Abstract
Despite growing evidence supporting the evaluation, classification, and treatment of acetabular bone loss in revision hip replacement, advancements have not been systematically incorporated into a single document, and therefore, a comprehensive review of the treatment of severe acetabular bone loss is needed. The Stavros Niarchos Foundation Complex Joint Reconstruction Center at Hospital for Special Surgery held an Acetabular Bone Loss Symposium on June 21, 2019, to answer the following questions: What are the trends, emerging technologies, and areas of future research related to the evaluation and management of acetabular bone loss in revision hip replacement? What constitutes the optimal workup and management strategies for acetabular bone loss? The 36 international experts convened were divided into groups, each assigned to discuss 1 of 4 topics: (1) preoperative planning and postoperative assessment; (2) implant selection, management of osteolysis, and management of massive bone loss; (3) the treatment challenges of pelvic discontinuity, periprosthetic joint infection, instability, and poor bone biology; and (4) the principles of reconstruction and classification of acetabular bone loss. Each group came to consensus, when possible, based on an extensive literature review. This document provides an overview of these 4 areas, the consensus each group arrived at, and directions for future research.
Introduction
Total hip replacement continues to have outstanding long-term results with excellent pain relief, improved hip mobility, and high levels of functional improvement [88]. While hip replacement revision rates are decreasing, approximately 10% to 15% of patients will undergo revision at 20 years; the most common causes of failure are aseptic loosening, instability, and periprosthetic joint infection, and each failure mode can lead to acetabular bone loss and even pelvic dissociation in severe cases [14,138]. Bone loss can occur as a consequence of mechanical loosening, osteolysis, or removal of components at the time of revision. Osteolysis is often secondary to polyethylene or articular metal wear debris but may also develop secondary to corrosion at modular metal junctions used in the femoral or acetabular components [2,159,183]. The successful management of complex acetabular defects and pelvic discontinuities requires careful preoperative planning, specific operative techniques, and a comprehensive understanding of implant design, bone ingrowth potential, and bearing materials [146]. Despite countless articles, chapters, and podium presentations on the evaluation, classification, and treatment of acetabular bone loss in revision hip replacement, several topics remain controversial, with multiple acetabular reconstruction options and a range of operative techniques available. Evolving surgical techniques, technologies, and materials have facilitated the management of complex acetabular defects. However, these advancements have not been systematically incorporated into existing treatment paradigms. A comprehensive review and approach to the treatment of severe acetabular bone loss is therefore needed.
The complexity and controversies around the surgical management of acetabular bone loss at the time of revision total hip replacement led to the creation of the Acetabular Bone Loss Symposium. The goals were to convene an international panel of hip revision experts, surgeons, and biomechanical engineers, to delineate accepted trends, emerging technologies, and areas of future research and to develop, when applicable, consensus answers, based on an extensive literature review, to questions related to the workup and management of acetabular bone loss. The consensus symposium was convened by the Stavros Niarchos Foundation Complex Joint Reconstruction Center at Hospital for Special Surgery on June 21, 2019, in New York City. The 36 experts were divided into groups, with each discussing a specific area related to the evaluation and management of acetabular bone loss.
Prior to the symposium, the steering committee and invited participants created a list of questions that fell into 4 categories of investigation and discussion: (1) preoperative planning and postoperative assessment; (2) implant selection, management of osteolysis, and management of massive bone loss; (3) the treatment challenges of pelvic discontinuity, periprosthetic joint infection, instability, and poor bone biology; and (4) the principles of reconstruction and classification of acetabular bone loss. This was followed by a comprehensive literature search related to each topic, with the search results made available to the participants. The 4 panels developed preliminary consensus statements that were then presented to the entire group for comment, discussion, and further refinement into a final document. After revision, the final document was circulated to all participants for their input and approval. The results of the symposium, presented here, represent the current recommendations of this expert group of revision hip surgeons and biomechanical engineers on approaches to acetabular bone loss, with the incorporation of available evidence where applicable.
Panel 1: Preoperative Planning and Postoperative Assessment
The preoperative assessment should confirm the etiology of failure of the total hip replacement and the reason for revision, determine the necessary preoperative preparations including required instruments and implants, and produce a preoperative plan for a patient with acetabular bone loss. Once the etiology of failure (aseptic vs septic loosening, for example) has been determined, the surgeon must decide whether additional imaging is necessary. In addition, preoperative planning should anticipate intraoperative challenges including the techniques for implant removal, the implants for reconstruction, and the intraoperative plan that includes expected cup size, bearing couple, implant constraint, and additional materials needed (mesh, augments, cages, bone graft). This panel focused primarily on preoperative factors that may influence the surgical management of acetabular bone loss. While outside the scope of this document, the expert panel would like to emphasize that all patients undergoing primary or revision surgery should undergo standardized health optimization and infection screening protocols to reduce the risk of perioperative medical or surgical complication.
Patient History and Patient Demographics: Considerations in Acetabular Revision
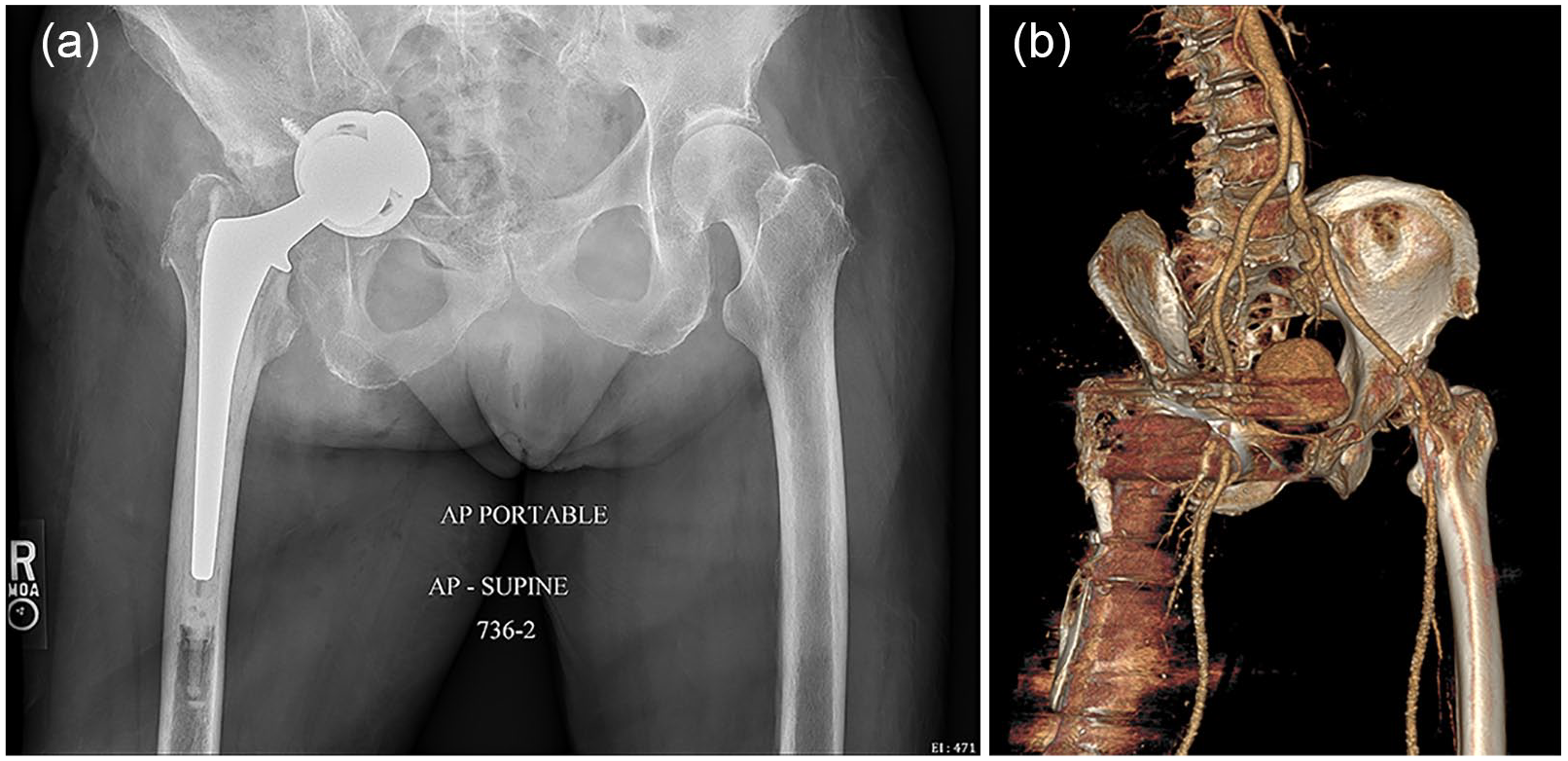
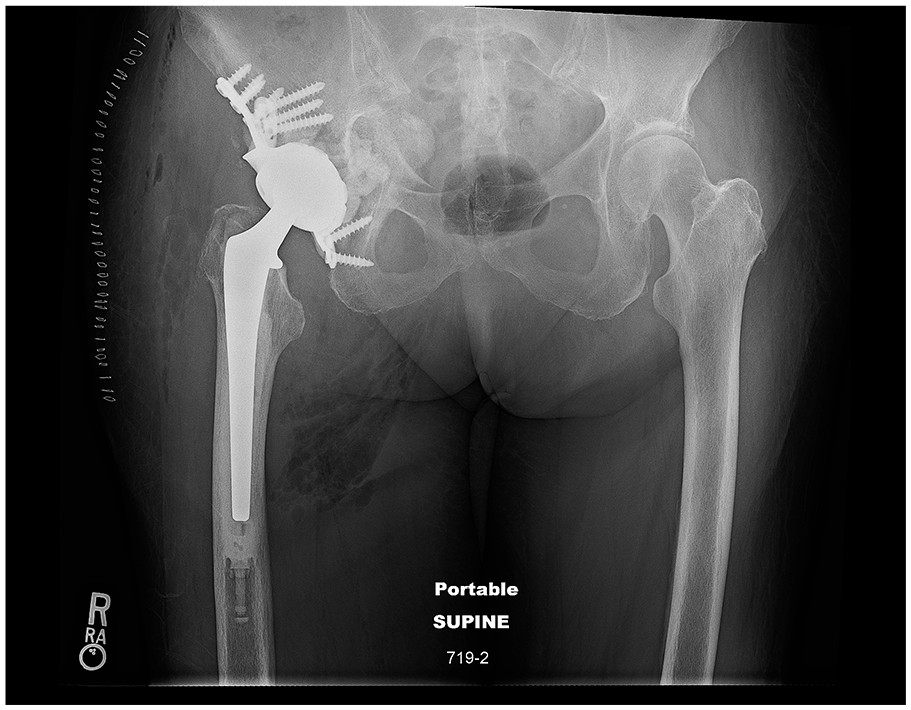
Patient age and sex provide important demographic information that may influence the surgical treatment plan. From an anatomical standpoint, the female pelvis tends to be smaller and has a smaller acetabular diameter [205]. The relevance of this anatomical sizing difference between men and women relates to increased likelihood of requiring an acetabular augment when reconstructing a superior acetabular defect; this is because the maximum anteroposterior (AP) diameter will often be diminished and not allow jumbo acetabular components to obliterate these superior bone defects. These bone defects of similar size in male patients with greater surrounding bone stock and a larger acetabular AP diameter can often be treated with an oversized acetabular component with screw fixation (Fig. 1).
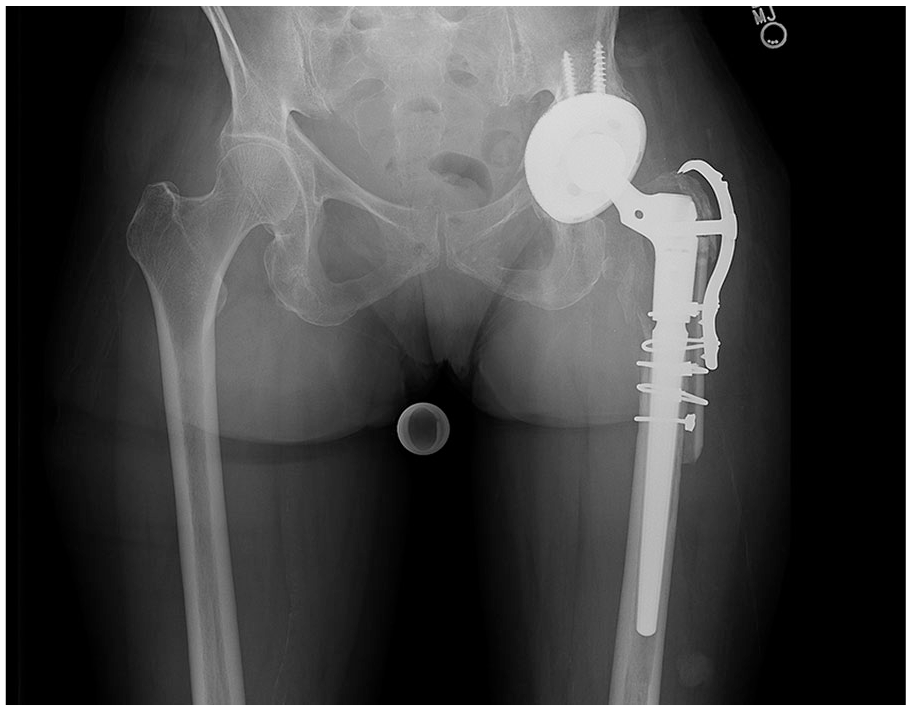
Anteroposterior left hip X-ray demonstrates a jumbo cup with screw fixation.
In addition, often women present at the time of revision with worse bone quality and have a higher incidence of metabolic bone disorders (including osteopenia, osteoporosis, or insufficiency fractures) than age-matched men and these conditions influence the ability to gain rigid fixation during acetabular reconstruction. While these factors may be more common in older female patients, the expert panel emphasized the importance of preoperatively assessing native acetabular diameter and the quality of host bone available for fixation at the time of reconstruction. In addition, the panel emphasized the importance of identifying other modifiable and nonmodifiable risk factors for poor bone quality, including prior radiation to the pelvis, chronic immunosuppressive or corticosteroid medication use, and a history of inflammatory arthritis.
All prior hip surgeries, surgical approaches, and incisions need to be carefully recorded and evaluated, particularly in the multiply revised patient. In addition, the currently implanted components must be known preoperatively. Previous operative reports and implant labeling information, especially for the most recent procedure, are helpful in identifying current implants and also prior surgical approaches. If retaining the femoral stem, knowing the type of femoral component (eg, modular vs monoblock and, if modular, trunnion size and the availability of suitable heads sizes and lengths) is essential. The primary diagnosis for the index procedure (eg, developmental hip dysplasia, slipped capital femoral epiphysis) can provide information regarding pelvic size and bony anatomy. A history of wound or periprosthetic joint infection may influence the need for extensive preoperative workup for infection. Also, risk factors for postoperative instability, such as a history of hip instability, lack of spinopelvic mobility as assessed on sitting and standing radiographs [141], or prior spinal surgery with instrumentation [5], should be identified; these will influence bearing choice (a large femoral head diameter, dual mobility, or constrained liner).
Physical Examination
The location of prior surgical incisions and the overall condition of the soft tissue envelope around the hip must be evaluated to determine if there is adequate tissue quality for coverage and healing. If the prior incision is adherent to the underlying tissues or to the greater trochanter, or the soft tissue coverage may be at risk, a preoperative plastic surgery consultation is indicated. Wound erythema or localized heat or swelling may indicate indolent infection or an underlying adverse local tissue reaction (ALTR). Proximal thigh and gluteal atrophy may demonstrate the severity and duration of hip joint dysfunction and musculoskeletal deconditioning that may influence recovery after revision surgery.
A careful assessment of gait patterns and the presence or absence of a limp provide additional information on potential abductor weakness [238], coxalgia secondary to weight bearing hip pain, or presence of an underlying leg length discrepancy [7]. The use of assistive devices for ambulation, such as crutches, walker, or cane, is important additional information about a patient’s overall functional status prior to revision surgery [240]. In such cases, upper extremity function significantly influences postoperative recovery. Watching the patient arise from a seated position and get on and off the examining table also provides information about functional ability, coordination, muscle power, and overall physical function. Hip range of motion and the presence of adductor and/or hip flexion contractures should be noted during the physical examination. Hip exposure planning in these cases will be more complicated and must be extensile. Significant soft tissue releases and ample scar excision may be necessary to mobilize the femur and acetabulum. Lower limb muscle power should be carefully recorded, particularly abductor power [149], as abductor dysfunction may influence implant selection (eg, larger femoral head or dual mobility bearings). For complete abductor deficiency, constrained hip implants are generally required [54], although the use of dual mobility implants in these situations is increasing [189]. A thorough neurovascular examination must be documented preoperatively because vascular injury and neuropraxias can occur in extensive acetabular reconstructions, and documentation of preoperative neurovascular status is important as a baseline. Preoperative vascular surgery consultation is indicated when there is evidence of vascular compromise [224].
When reconstructing hip center of rotation, leg length inequality must be carefully assessed in the standing position and compared with radiologic measurements. If the source of the leg length inequality (secondary to functional or structural leg length differences, hip contractures, fixed vs flexible pelvic obliquities, intra-articular or extra-articular structural leg length differences) is unclear, then long leg imaging should be obtained [140,142]. Patients should be counseled preoperatively concerning leg length inequality and whether the revision surgery will improve it. Discussing patient expectations on leg lengths and overall function is necessary to optimize patient satisfaction after revision surgery.
Imaging
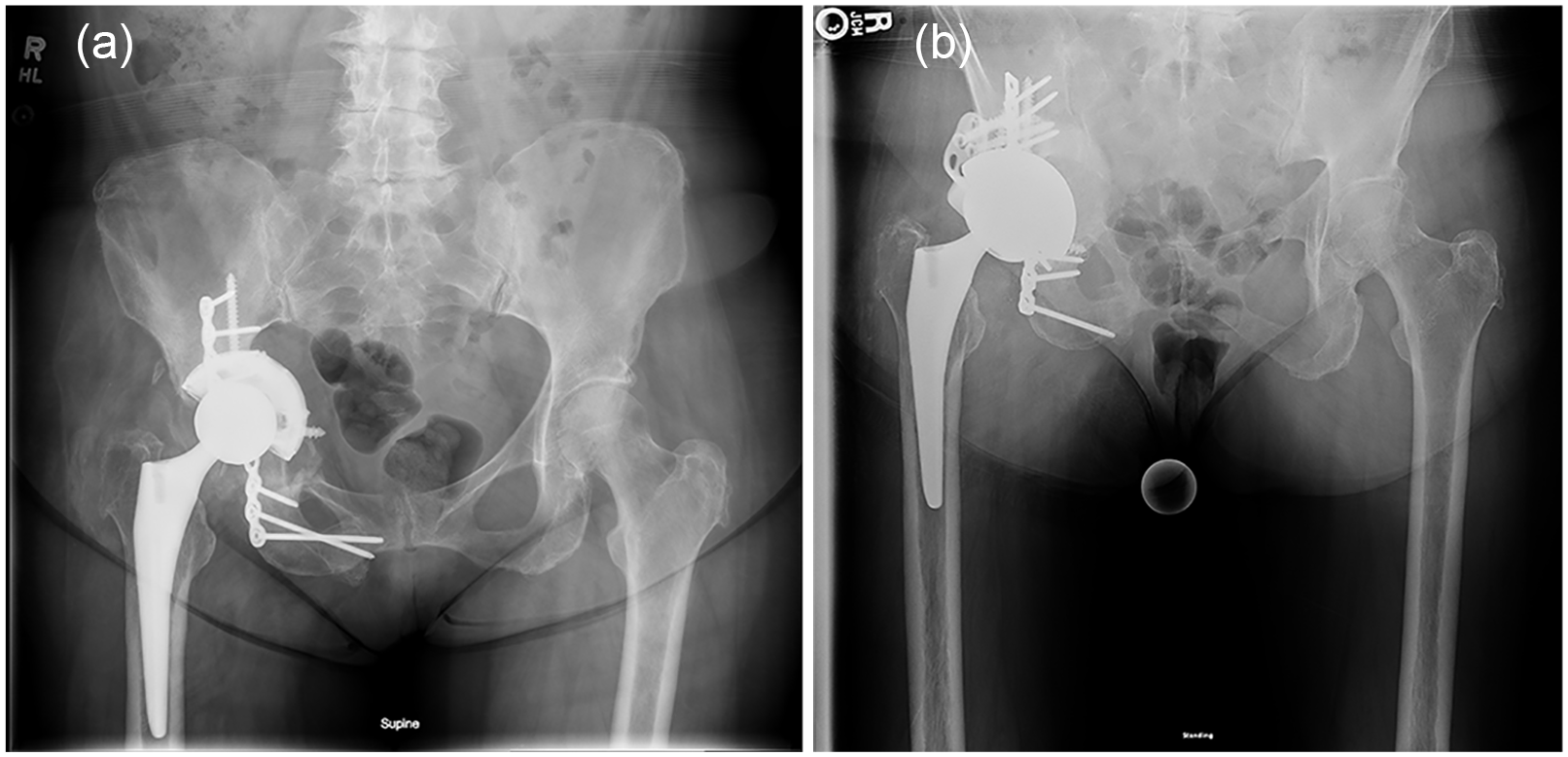
Preoperative radiographs should always be obtained to allow previous reconstructions to be evaluated. Older radiographs also provide a better assessment of interval radiographic changes and the potential etiology of progressive acetabular bone loss. Various imaging modalities are available to assess acetabular bone loss, and each 1 can provide a different perspective to improve preoperative planning. The expert panel agreed that for cases with minimal acetabular bone loss, an AP pelvis radiograph is sufficient (Fig. 2).
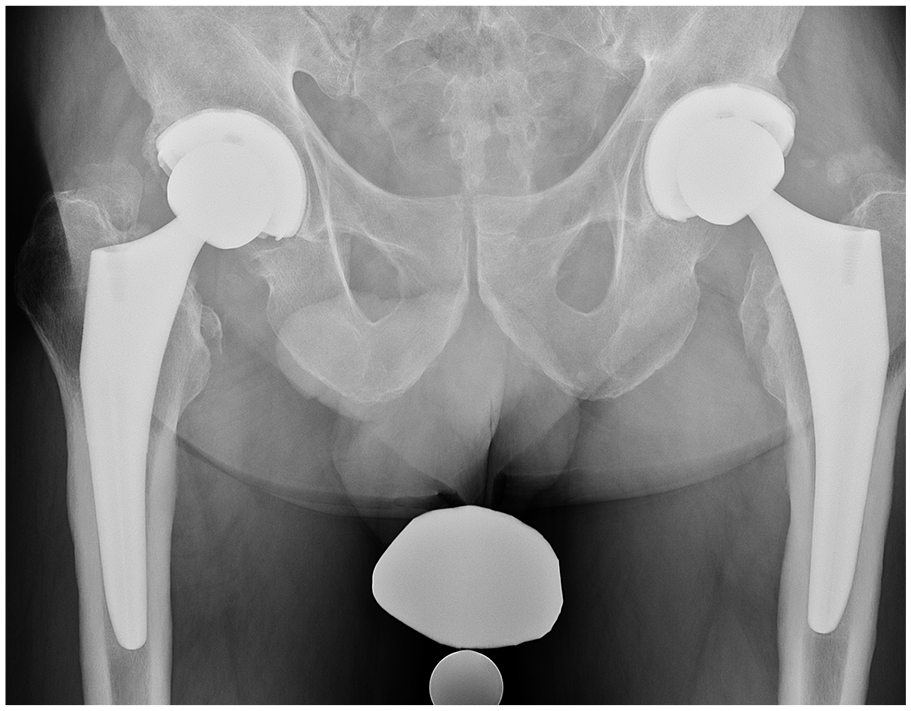
Anteroposterior pelvis radiograph shows bilateral total hip arthroplasties, with the right hip undergoing revision for recurrent instability without periacetabular bone loss.
For acetabular bone loss, Judet views offer a better, more detailed assessment of the anterior and posterior columns. For more complex acetabular bone loss patterns, a majority of the panel agreed that computed tomographic (CT) scanning with or without 3D reconstructions provides a valuable role in assessment of the location and quantity of acetabular bone loss and can help diagnose the presence of a pelvic discontinuity. CT scans are also recommended in the assessment of the extent and location of osteolysis and can provide important information on the need for bone graft, acetabular augments, or alternative acetabular reconstructions (cup-cage or custom).
Anteroposterior pelvis radiograph
All patients being evaluated for a painful total hip replacement and possible acetabular bone loss should have an AP pelvis radiograph. A standing AP radiograph allows for a better understanding of the functional pelvic position (pelvic tilt), as well as presence of a pelvic obliquity, which may contribute to a functional leg length discrepancy or be compensatory from a structural leg length inequality. The AP pelvis radiograph also provides valuable information regarding the symmetry of the obturator foramina, intra-articular leg length differences, fixation of the acetabular component and presence or absence of peri-implant radiolucency, component position, acetabular center of rotation, migration of the acetabular component, and acetabular bone loss and osteolysis assessment [167,172,211,227]. The expert panel agreed that from the AP pelvis radiograph, the degree and location of bone loss, the extent of osteolysis, and the amount of component migration can identify whether advanced imaging is needed for further assessment [2,122,246] (Fig. 3).
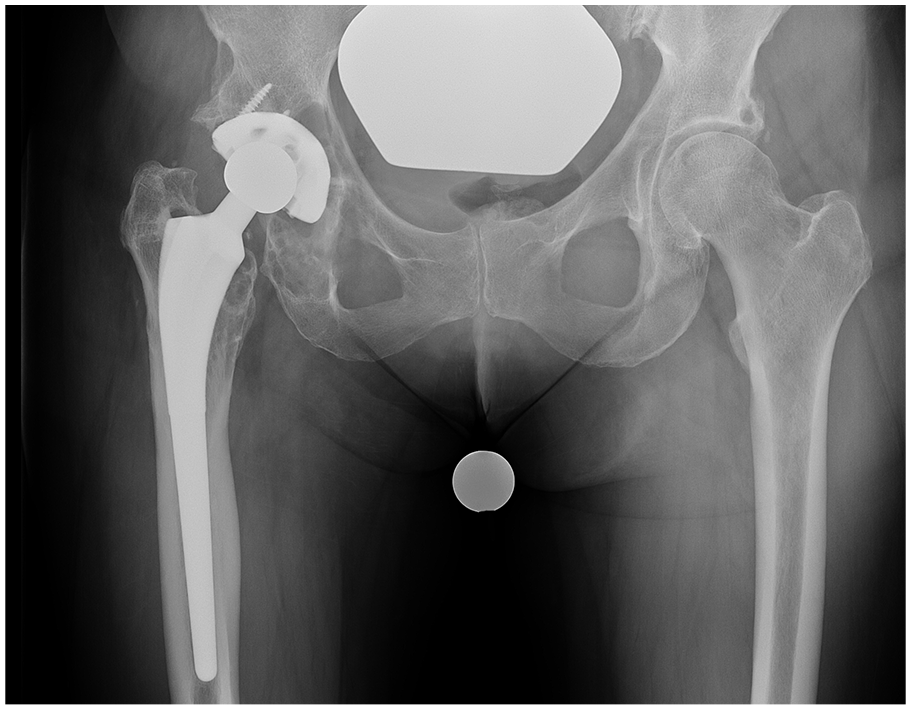
Anteroposterior pelvis X-ray shows osteolysis medially and extending inferiorly into the ischium. A computed tomography scan can quantify the volume of osteolysis and involvement of the posterior column and is recommended.
Frog lateral view
This view provides more information on the quality of fixation of the femoral component, overall femoral bone quality, and deformity in the sagittal plane [154], and proximal femoral deficiency. However, this view does not provide additional information than the AP pelvis radiograph on the evaluation of acetabular bone loss (Fig. 4).
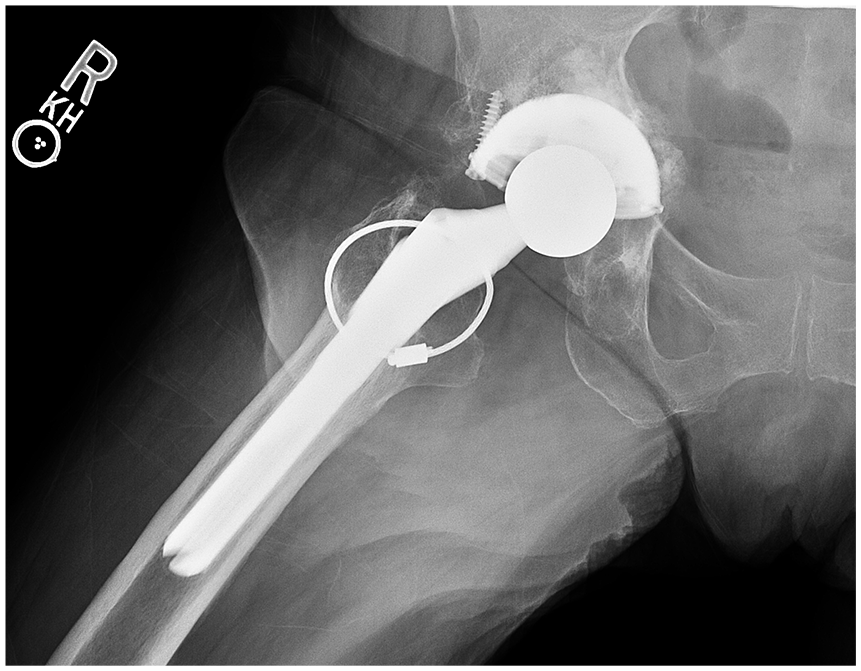
Frog lateral view shows a medial wall defect. This view does not provide additional information compared with the anteroposterior view with regard to the extent and location of acetabular bone loss.
Cross-table orthogonal view
This radiograph provides additional information of acetabular anteversion and can further delineate the extent of posterior column and ischial osteolysis (Fig. 5).

Cross-table lateral X-ray demonstrating posterior column osteolysis.
Judet views
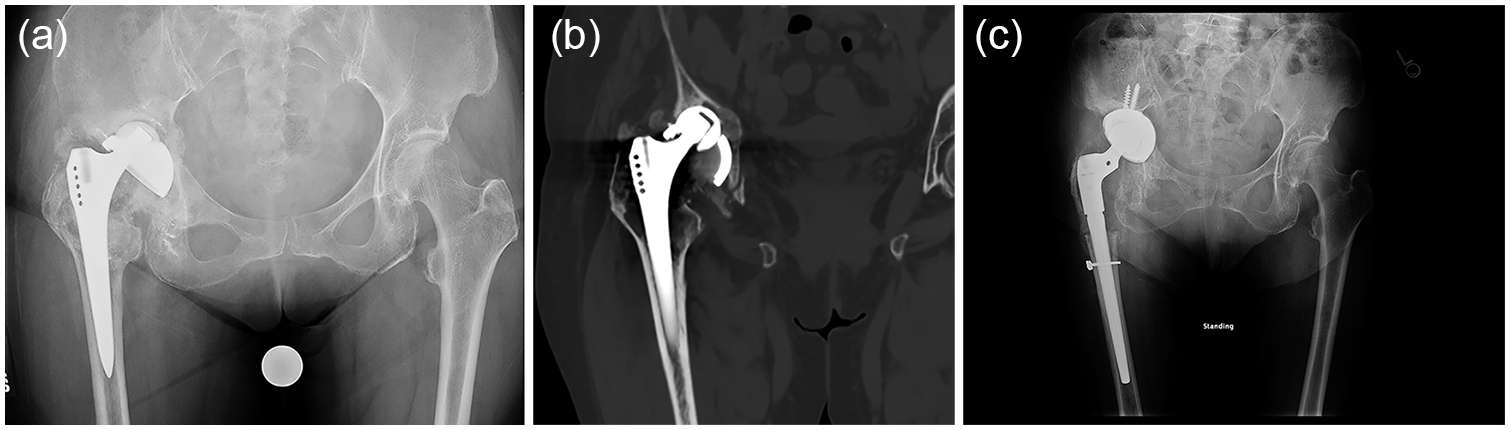
To better understand the integrity of the anterior and posterior columns, the direction of acetabular component migration in the AP plane, and the assessment of posterior or anterior column acetabular osteolysis that is difficult to identify on the AP pelvis view, Judet views are useful [154,171,211,216,234]. Disruption of both the anterior and posterior columns, as visualized on the obturator and iliac oblique views, respectively, indicates presence of a pelvic discontinuity. Martin et al [154] documented the effectiveness of Judet views in evaluating pelvic discontinuity compared with advanced imaging with CT. They found that in diagnosing pelvic discontinuity, AP pelvis and true lateral views of the hip in combination with Judet views were 100% accurate when used in intraoperative confirmation of findings to confirm its accuracy [154]. The majority of the expert panel agreed that Judet views were often sufficient to diagnose without further imaging (Fig. 6a–c).
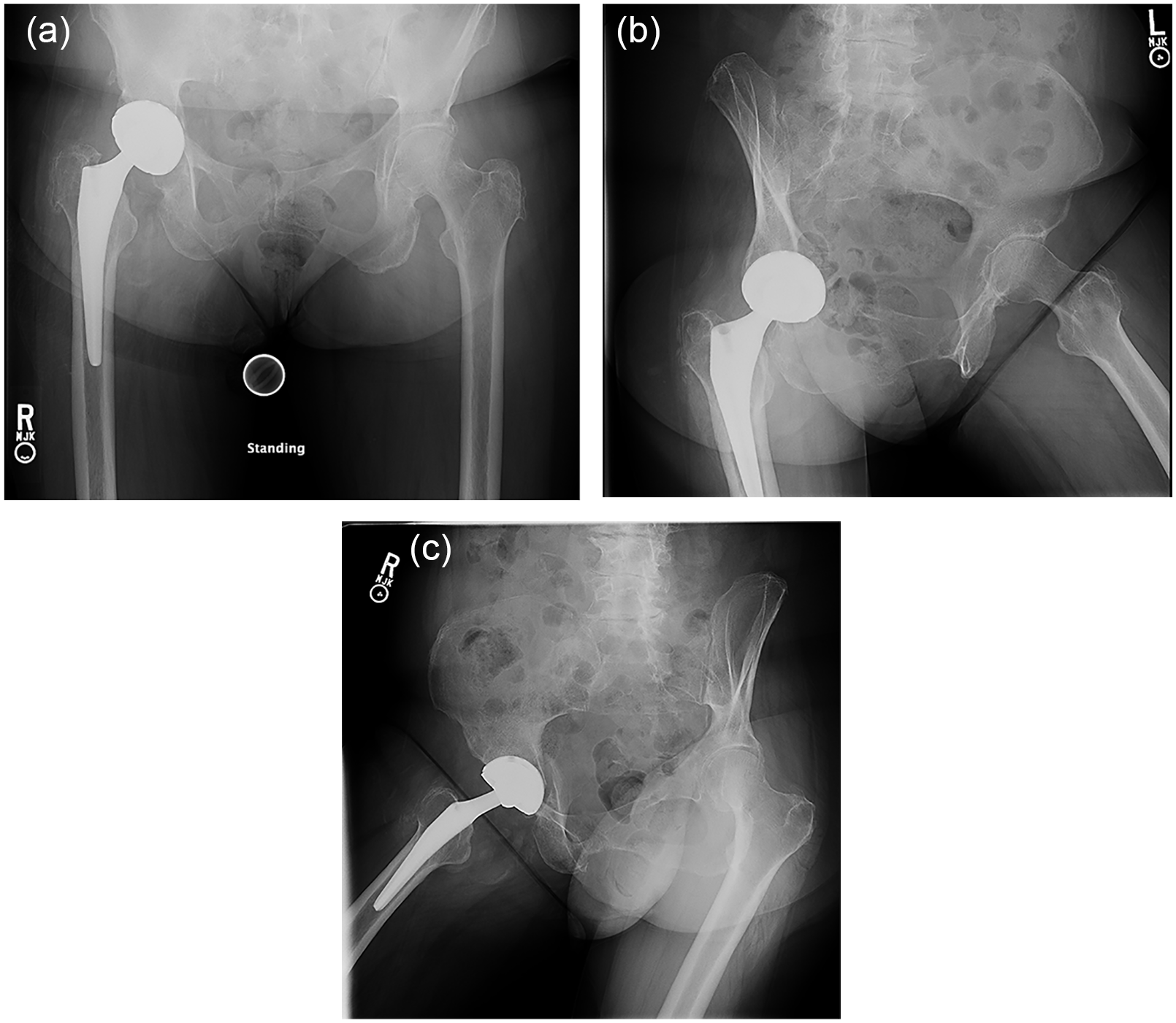
(a) Anteroposterior pelvis radiograph demonstrates disruption of the ilioischial line and obturator asymmetry concerning for pelvic discontinuity. (b) Obturator oblique demonstrates an intact anterior column. (c) Iliac oblique X-ray shows a posterior column fracture.
For chronic discontinuity with associated bone loss, CT is useful in understanding the location of the discontinuity and the extent of associated osteolysis [2].
Computed tomographic scanning
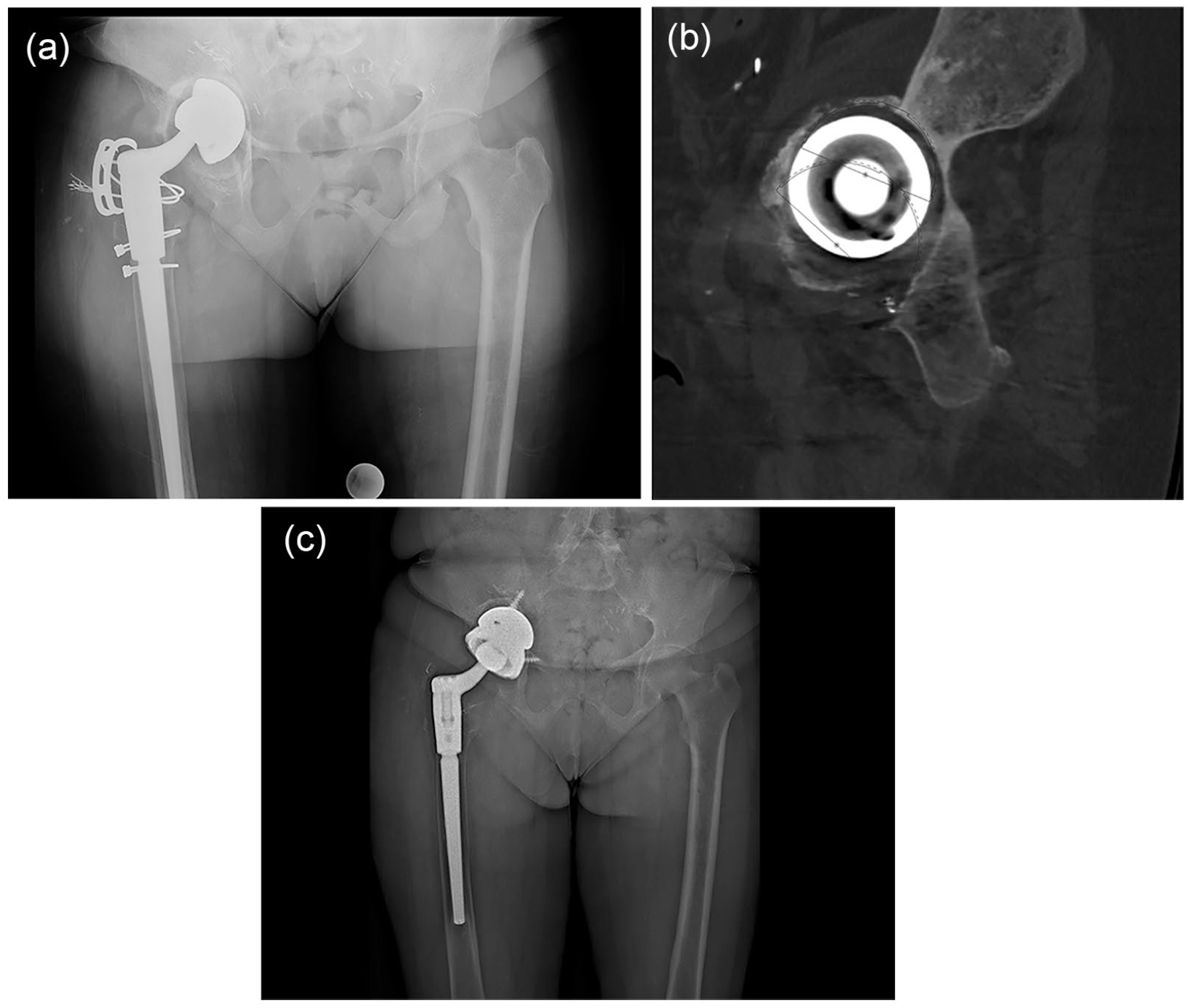
Allowing for a more comprehensive evaluation of the extent of bone loss, localization, and quality of remaining bone (particularly the extent of ischial bone loss), CT scanning can also differentiate between osteolysis and stress shielding [72,122,135,246]. In addition, it provides information on the AP diameter of the remaining acetabulum, and CT data can be manipulated into 3D reconstructions that can help in appreciating the shape and size of the bony defect [95] (Fig. 7a–d).
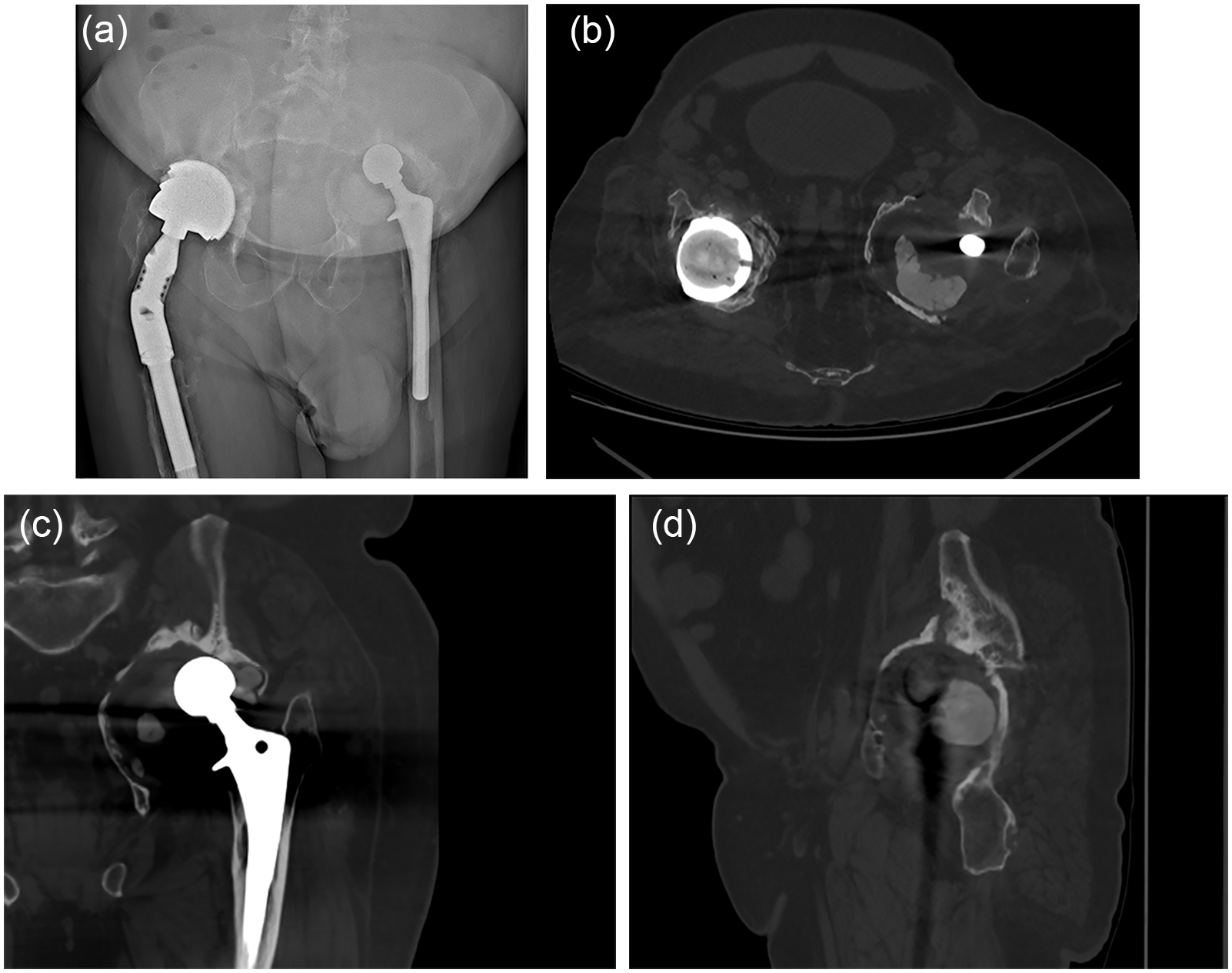
(a) Standing AP radiograph demonstrates massive acetabular bone loss in the left pelvis. (b) CT axial view showing retained cement in a prior hemi-resection for prosthetic joint infection with medial wall deficiency and large AP diameter (74 mm), demonstrating massive acetabular bone loss. (c) CT coronal view shows superior migration of femoral head without dislodged cemented acetabular component. Multiple defects in the medial wall are noted. (d) CT sagittal view shows intact ischium, but deficient anterior wall and fracture line in posterior column that extends through entire column, confirming pelvic discontinuity. AP anteroposterior, CT computed tomography.
The primary limitation of CT is the image distortion created by the metal artifact of the existing implant, although metal artifact reduction techniques have mitigated this problem [72,192]. Subtle pelvic discontinuities might be missed with CT due to either artifact or out-of-plane assessment of the fracture line. A sagittal reformat that represents a pelvic orientation similar to that of a Judet view may detect pelvic discontinuity better than standard CT sagittal reconstruction [154]. An additional disadvantage of CT is the increased amount of radiation (compared with a standard radiograph), although newer lower radiation dose CT technology has reduced this risk [253].
Three-dimensional CT reconstruction
Computed tomography reconstructions that allow for the pelvis to be rotated in 3D provide a 360° assessment of acetabular bone loss. These 3D reconstructions are helpful in more advanced cases of bone loss and provide visualization of bone loss that cannot be easily identified with standard radiographs, magnetic resonance imaging (MRI), or CT [73,95,165]. In addition, segmentation can be performed to evaluate the pelvis with the implant subtracted (Fig. 8a–c).
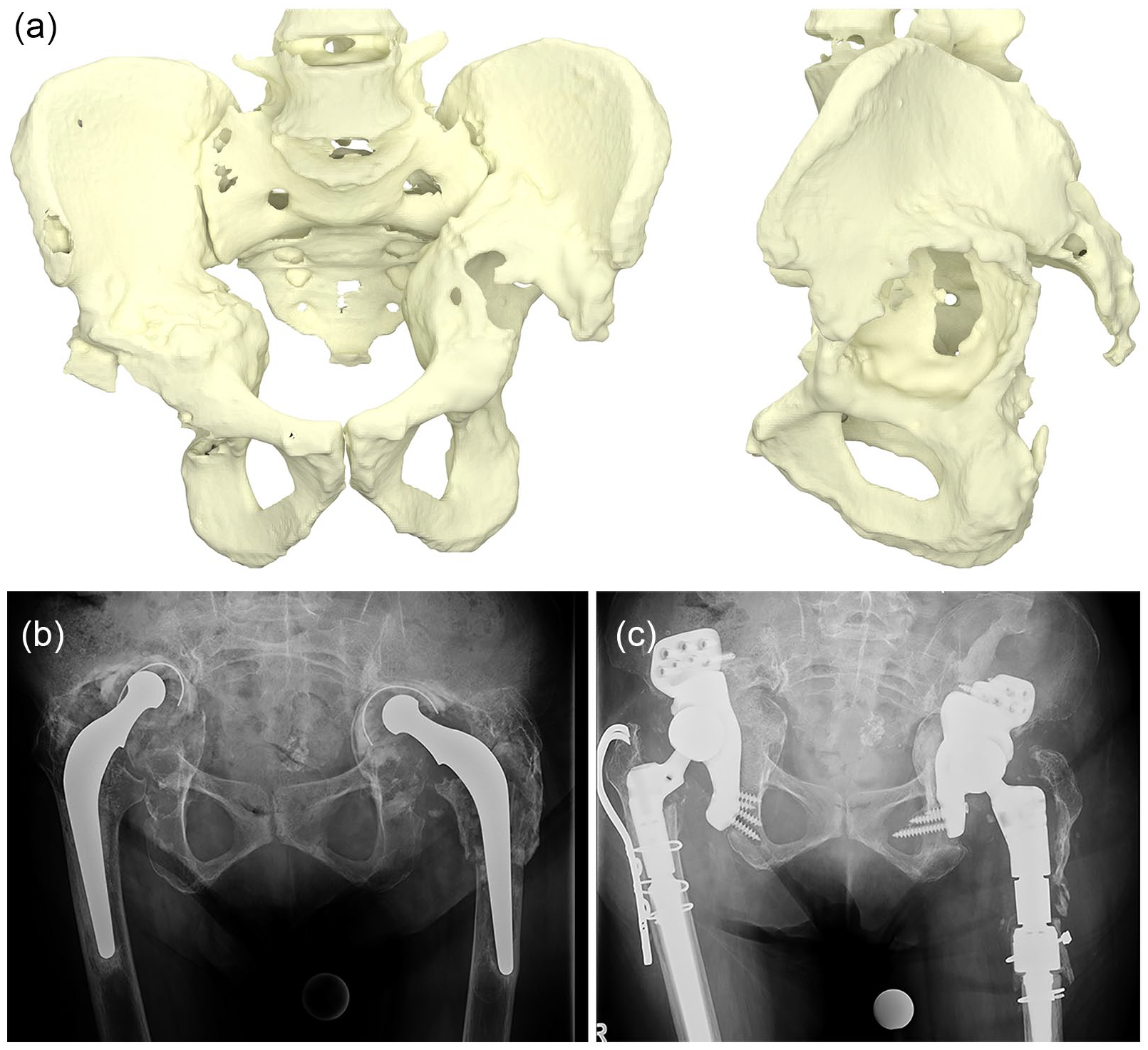
(a) Preoperative computed tomography 3D reconstruction model, AP and lateral, shows bilateral massive acetabular bone loss after implants were segmented and removed (product manufactured by LimaCorporate S.p.A., Italy). (b) AP pelvic X-ray does not as clearly evaluate these defects and areas of intact host bone compared with the 3D reconstruction model. (c) AP pelvis postoperative radiograph demonstrating bilateral custom acetabular components. AP anteroposterior.
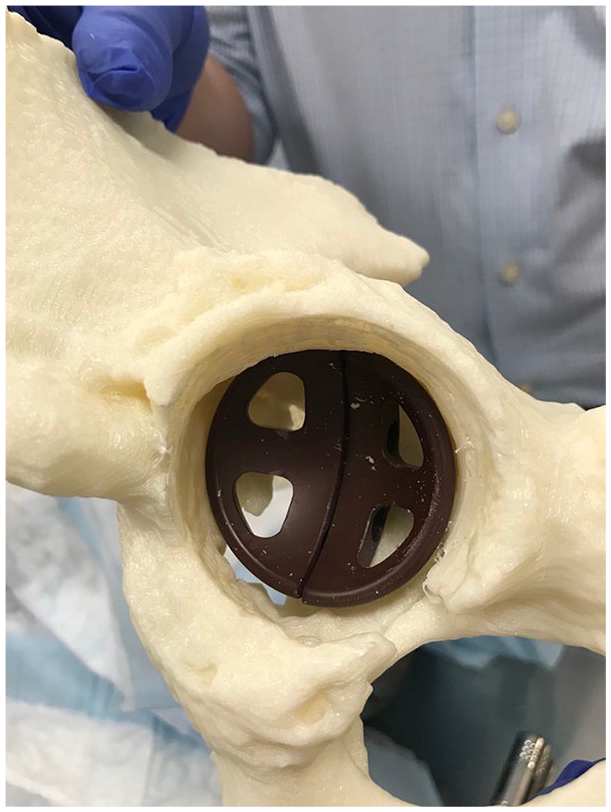
Computed tomography reconstructions can also be used to generate 3D printed plastic models [65,204]. These life-size plastic pelvic models allow for enhanced surgical preparation so that reaming and implantation can be practiced on the model prior to surgery [66]. Models can also assist in deciding whether an “off the shelf” implant can be used or if the creation of a patient-specific implant is required [261]. A preoperative CT reconstruction is also required to plan and fabricate custom acetabular components [76] (Fig. 9).

Three-dimensional printed plastic model allowing for preoperative planning with multiple augments for a complex acetabular reconstruction.
Magnetic resonance imaging
Magnetic resonance imaging is primarily useful for imaging soft tissue, making it beneficial in evaluating muscle damage, particularly to the abductors. It is also useful for assessing soft tissue, synovial, and osteolytic collections around the hip. Hip infection with soft tissue extension and osteomyelitis can also be visualized on MRI. Pseudotumor secondary to metal-on-metal articulations can be identified with MRI, and capsular thickening and synovitis can be quantified [150,169]. While MRI can provide information on acetabular bone loss [252], CT remains the most definitive modality for bone loss assessment [2,211]. Magnetic resonance imaging may have a role in assessing both the quality and viability of remaining acetabular bone [49], but further investigation and validation is necessary (Fig. 10a and b).
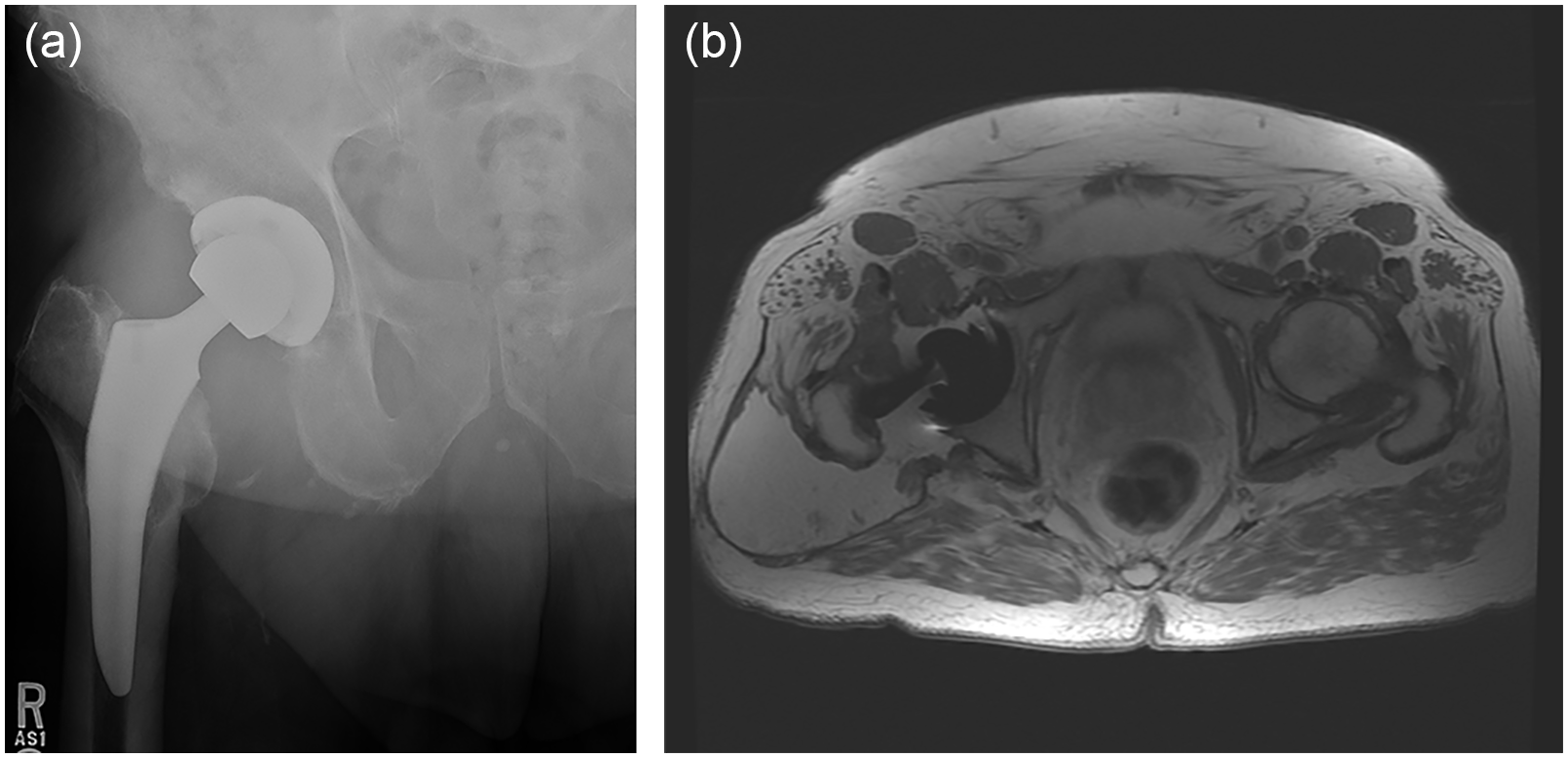
(a) Anteroposterior right hip X-ray demonstrates well-fixed uncemented components in a patient with increasing right hip pain with cobalt-chrome femoral head and elevated metal ions. (b) Magnetic resonance axial image demonstrates large cystic collection with metal debris consistent with aseptic lymphocyte-dominant vasculitis-associated lesion (ALVAL).
Magnetic resonance/CT angiography
A preoperative magnetic resonance/computed tomography angiography (MRA/CTA) is indicated when acetabular component migration in the setting of severe acetabular bone loss places neural or vascular structures at risk during acetabular component revision [63]. An MRA/CTA should be considered when significant component migration of greater than 1 cm exists medial to the ilioischial line, especially in cases without chronic remodeling or new bone at the floor of the socket [75]. Magnetic resonance/computed tomography angiography is also useful when screws or cement protrude outside the pelvic floor or when severe heterotopic bone has developed and incorporation of the adjacent neurovascular structures may have occurred [57]. In severe cases, the ureter and intrapelvic organs may be displaced. These studies can also help in planning the removal of intrapelvic collections, especially in cases of infection (Fig. 11a and b).
(a) AP pelvis X-ray demonstrates greater than 1-cm intrapelvic migration without medial osseous remodeling. (b) Consideration for computed tomographic angiography to delineate intrapelvic vasculature in relation to acetabular component and screws. AP anteroposterior.
In summary, a hierarchy of techniques can be considered preoperatively to assess complex acetabular defects. An AP pelvic radiograph produces fundamental information regarding acetabular bone loss and implant migration. Cross-table lateral and Judet views provide additional information on the status of the ischium and posterior/anterior columns, respectively. Advanced cross-sectional imaging should always be obtained when (1) a pelvic fracture is visible on standard images and the fracture extends through Kohler line, (2) concomitant rotation of the hemipelvis (suggesting a pelvic discontinuity) exists, (3) osteolysis is significant, extending into the ischium on the AP radiograph, and (4) medial migration of the acetabular component, which may indicate column disruption.
While the quantity of remaining host bone can be readily assessed with preoperative CT scans, assessing host bone quality and viability remains a challenge. Preoperative assessment and radiographic evaluation should provide insight into expected bone quality and potential bone viability at the time of acetabular reconstruction. For bone quality, particularly useful details from the patient history include patient age, sex, history of metabolic bone disease (including osteoporosis), and lab abnormalities (calcium, vitamin D, and elevated thyroid hormone). A history of pelvic radiation, joint infection, or failure secondary to metallosis may all lead to reduced bone quality and/or bone biology. Computed tomography metal reduction protocols combined with implant segmentation may allow for periacetabular bone quality to be assessed with Hounsfield units, but there is currently no standard practice and these techniques still remain susceptible to implant artifact.
For preoperative planning purposes, poor bone viability (eg, prior radiation to bone and osteonecrosis) is considered separately from poor bone quality (eg, low bone mineral density and osteoporosis). However, both bone quality and viability are difficult to assess with current imaging modalities. A combination of plain radiographs and a CT scan allows for excellent assessment of bone quantity but provides only an estimation of bone viability and quality [211,246]. Thickness of the cortical bone, bone density, and the presence of sclerotic bone surrounding the existing implant component can be assessed by CT imaging. Determining that a patient has poor bone quality and healing potential will influence implant choice and reconstruction technique. Chronic pelvic discontinuities with poor bone quality are unlikely to heal primarily and should rather be treated with bridging constructs with fixation to the iliac wing and ischium. While studies in this area are limited, poor bone quality may require increased host bone-implant contact and consideration for spanning constructs that gain screw or flange fixation in the iliac wing and ischium [146]. In addition, for osteonecrotic bone or bone that has undergone prior radiation treatment, improved results have been shown from high friction, highly porous materials compared with conventional surface coatings [47,109].
Preoperative Planning of Surgical Approach
Many factors must be considered when planning a surgical approach for patients with acetabular bone loss. The approach must be extensile and allow for complete visualization of the acetabular rim and the posterior and anterior columns. It must also allow for the insertion of a large hemispherical shell, a cage, an augment, or a patient-specific triflange as indicated in the operative plan. The selected surgical approach—including posterior, direct lateral, or anterolateral—may be used depending on surgical preference and experience. The direct anterior approach may also be used by surgeons who are experienced with this approach, but has limitations in exposure and is much less extensile.
Intrapelvic approaches may be needed for vascular control of significant hemorrhage, intrapelvic abscess, and pseudotumor [78,232]. Patients with intrapelvic protrusion of the existing acetabular implant or screws should undergo MRI/CTA prior to surgery to determine if vessels will be at risk [57]. If a major vascular structure is at risk, a vascular surgeon should be available to assist during extraction of existing components. A retroperitoneal approach to gain proximal vascular control prior to extraction is mandatory in these extreme cases.
Extensive exposures are frequently necessary to visualize a badly damaged acetabular socket when the femoral component is solidly fixed. While a sliding trochanteric osteotomy can improve visualization, if the preoperative plan is to maintain the femoral component, a standard trochanteric osteotomy usually provides adequate 3-column exposure.
Femoral component revision of a well-fixed implant may be required in the rare circumstance that the hip cannot be reduced after acetabular reconstruction. However, this should be accounted for in preoperative planning and intraoperative assessment. A high hip center is preferable to the morbidity associated with removing a well-fixed femoral component. More commonly, a femoral component may be removed when the acetabular component is intrapelvic and the hip cannot be dislocated. In this instance, retrograde removal through an extended trochanteric osteotomy is necessary.
Postoperative Weight Bearing and Radiographic Assessment
Weight bearing status after complex revision for acetabular bone loss should be individualized based on initial fixation quality. Most patients should be using protected weight bearing for 6 to 12 weeks. Progression of weight bearing status is dependent on serial imaging and assessment of implant stability and bone quality. If femoral revision with an extended trochanteric osteotomy was performed, further limitations such as trochanteric precautions may be required.
Radiographic follow-up of complex acetabular revisions should be performed postoperatively at regular intervals (6 weeks, 3 months, 6 months, and 1 year) to confirm acetabular construct stability. While initial migration can occur without eventual construct failure, if present on radiologic follow-up, more frequent imaging should be performed and an extended period of protected weight bearing is indicated. Radiostereometric analysis (RSA) is a validated technology for careful assessment of component migration but is only available in selected academic centers [116,123]. However, longitudinal studies of acetabular revision constructs monitored with RSA technology provide valuable, detailed information on the amount of migration that can occur without eventual construct failure [164]. Superior and medial migration of greater than 5 mm or alteration in component inclination by 10° or greater is concerning and requires careful monitoring [215].
Plain radiographs are currently the standard of care to assess postoperative construct stability, osseous integration into acetabular components, and healing of pelvic discontinuities. Radiographic findings associated with failure of bone ingrowth after acetabular component revision include persistent and progressive radiolucency at the bone-implant interface in multiple DeLee and Charnley zones [10,70]. Porous surface shedding or other evidence of fragmentation and debonding of the porous coating of the acetabular component is suggestive of interface instability and loosening. Serial radiographs are essential to detect progressive migration of the component and should continue until implant stabilization and ingrowth are achieved.
Radiographic findings that are indicative of construct failure include rotational migration of the component (most common vertically), as well as changes in screw position, screw fracture, and circumferential radiolucency around an acetabular screw. As needed, additional information can be obtained with postoperative CT that can better delineate the host bone/implant interface for evidence of osseous integration. Conversely, construct stability and osseous ingrowth can be defined as a lack of radiolucencies, absence of component migration, and/or evidence of spot welds on plain radiograph or cross-section imaging. For impaction grafting, a progressive loss of graft bone density and areas of frank bone resorption in association with significant component migration is concerning for graft failure.
In evaluating the healing of a pelvic discontinuity, Judet views and/or a CT scan provide a more comprehensive assessment of discontinuity healing [154]. Radiographs should also demonstrate an absence of prior periacetabular fracture lines and no evidence of migration.
Novel technologies including dynamic CT-based micromotion analysis and advances in CT and RSA technologies may prove helpful in determining bone ingrowth and the degree of component migration. Nonunion of a pelvic discontinuity does not indicate construct failure and depends on the type of construct fixation, mechanical or biologic. For mechanical constructs such as ilioischial cages and reconstruction rings, the failure rate may be greater when used in the treatment of pelvic discontinuity [146], although Taunton et al [231] reported 98% revision free for loosening and 81% healed discontinuity. Biologic constructs that involve osseous integration into a titanium component may not require discontinuity healing for implant survivorship. A biologic construct may be adequately fixed to the ilium alone (without inferior ischial ingrowth) or can unitize the superior and inferior hemipelvis as a bridging biologic construct with osseointegration both above and below the area of discontinuity; pelvic distraction often achieves this type of biologic construct stability [146]. The participants felt that MRI is not useful for examining failure of osseointegration but it is useful in evaluating soft tissue.
Clinical Outcome Measures
No specific outcome scores exist to evaluate acetabular component revision specifically, although current validated specific outcome scores can be applied including the hip disability and osteoarthritis outcome score (HOOS/HOOS Jr) and the D’Aubigne scales. Preoperative and postoperative scores should be obtained for comparison. Development of revision-specific outcome scores may be a future area of research as specific variables separate from the reconstruction itself may influence (abductor dysfunction) and clinical outcomes may not adequately reflect the relevant variables in outcome scores designed for primary joint replacement or osteoarthritis pain and dysfunction.
Panel 2: Implant Selection, Management of Osteolysis, and the Management of Massive Bone Loss
Implant Selection
Regardless of the mode of failure, the goal of acetabular reconstruction in the setting of acetabular bone loss is to obtain initial rigid fixation that allows for biologic and mechanical stability to permit full weight bearing and long-term construct survivorship [217]. For biologic constructs, the initial fixation should ensure minimal micromotion (<400 µm), which promotes osseous ingrowth into the acetabular component and long-term durability [177,185,217]. For mechanical constructs, such as cages and reconstruction rings, the initial fixation must be secure enough for long-term implant survivorship because biologic fixation does not occur. In these cases, enhanced screw fixation and discontinuity healing will influence implant survivorship, and these mechanical constructs should be placed in optimal biomechanical position (inferior and medial instead of superior lateral) to optimize long-term implant durability. A secondary goal of acetabular reconstruction is restoration of the native acetabular center of rotation [9], but achieving this goal should not compromise rigid fixation to host bone [55]. Whenever possible, restoration of the hip center of rotation should be restored, leading to improved hip stability and abductor function, as well as optimized hip range of motion and biomechanics.
Allograft bone augmentation combined with implant selection can be used in acetabular bone loss. The reconstruction principles for impaction grafting are a combination of both mechanical and biologic. Cancellous allograft packed into osseous defects with a cemented cup should have the stability to allow for gradual graft incorporation into host bone with creeping substitution [35,117]. In addition, the cemented strength must be enough for long-term construct success as no osseous ingrowth occurs into the all-polyethylene component.
If the failure mode is infection, then the principles of infection management prevail. This may include thorough debridement, implant removal, and reimplantation as a single stage or a 2-stage procedure with intervening use of an articulating antibiotic coated spacer. Alternatively, an approach used less often includes a static nonarticulating spacer or Girdlestone, with delayed reimplantation after treatment with antibiotics and retesting for infection. In select cases in which areas of dead bone remain in the pelvis due to prior radiation or bone necrosis secondary to metal-on-metal failure, nonviable bone may be resected or, if possible, it can be used as structural support for tantalum cups [221]. Reconstruction techniques could include larger hemispherical shells, acetabular augments that contact viable host bone, bone graft or bone graft substitute, or fabrication of a spanning patient-specific acetabular component [89,105]. Similarly, in cases in which significant abductor insufficiency exists, bearing selection should consider dual mobility or constrained acetabular components. In these cases, using a larger femoral head is usually not as successful in achieving long-term stability [148]. Acute acetabular failure and accompanying marked pain and disability may not allow the time needed for the design and fabrication of a patient-specific device; in such cases, an alternative selection of pelvic reconstruction may be required. However, clinical success should not be compromised for surgical expediency.
Hemispherical acetabular shells
Approximately 95% of acetabular revisions can be satisfactorily treated with a hemispherical cup with screw fixation [41,68,105,249]. Historically, the minimum amount of host bone contact against a hemispherical shell is approximately 50% [133]. While this percentage provides a general guideline, the introduction of high-friction, highly porous, multihole revision shells may be successful with less than 50% of autogenous bone/implant initial fixation. The location and quality of the remaining host bone plays an important role in determining whether the defect can be treated with a hemispherical shell or if it requires additional augmentation or cage stabilization.
However, a large hemispherical socket has limitations and is not adequate for all types of bone loss [176]. For example, as mentioned earlier, converting an elliptical shaped defect (superior cup migration) to a hemispherical shape is more challenging in a patient with a small anterior-posterior acetabular diameter. In these patients, the AP dimension required for obtaining a press fit between the ilium and the ischium may not be possible without sacrificing the anterior and posterior columns. In addition, reaming an elliptical defect into a hemisphere can raise the joint’s center of rotation [132,175]. This can produce a stable and ingrown socket and excellent function [83,118,158,244]; however, an important secondary goal of acetabular reconstruction is restoration of the native hip center [9], and from a biomechanical perspective, this is preferable to creating a high hip center [56,268]. For a smaller pelvis with a superior defect, the use of a superior augment or structural allograft allows for restoration of the hip center, and the use of anatomically sized acetabular component reduces the risk of overreaming the anterior and posterior columns [102] (Fig. 12a–c).
(a) Anteroposterior (AP) pelvis X-ray demonstrates femoral head migration through the acetabular component with significant periacetabular osteolysis. (b) Computed tomography coronal view shows periacetabular osteolysis, 50% host bone contact successfully treated with highly porous cup with screws. (c) AP pelvis X-ray 1 year post-operative demonstrates well fixed acetabular component with approximately 50% host bone contact successfully treated with highly porous cup with screws.
An area for future research is to predict the need for acetabular augmentation based on a ratio of the AP and the superior-inferior dimensions of an elliptical defect. Irradiated/devitalized bone is a concern when using a hemispherical socket alone, but advanced ingrowth surfaces with increased friction and porosity have demonstrated excellent results [47].
The use of augments has been a significant advance in acetabular bone loss and may prove more reliable long term than allograft [51,52,80,106,143,178].
Although augments currently come with a higher cost than allograft, they can provide the excellent anterosuperior to posteroinferior “pinch” fixation that is crucial for stable socket fixation [4,43,53,255]. They are also useful in posterior wall defects and other defects of the acetabular rim. In addition, they help optimize host bone-implant contact and can downgrade defects from more severe to less severe while maintaining the optimal hip center [137,173,196,212,242]. They can convert an uncontained defect to a contained defect and decrease the overall volume of acetabular bone loss [160,173,196,212]. However, a disadvantage of augments is that they do not restore bone in cases in which rerevision may be necessary.
Hemispherical shaped augments of varying diameter and height are popular because they are available in many sizes and can address bony defects; they can also be fixed with screws, except in cases of severe medial defects [136]. A contained elliptical shaped acetabular defect can be addressed with an augment placed in a wedge orientation (Fig. 13a and b). For uncontained segmental defects that do not involve the posterior column, a “flying buttress” augment configuration can be used to provide superior cup coverage and prevent superolateral cup failure (Fig. 14).
(a) AP pelvis X-ray demonstrates aseptic loosening of acetabular component with superior bone loss and broken screws, creating elliptical defect. (b) AP pelvis X-ray demonstrates an uncemented hemispherical cup with a superior augment for superior dome support and restoration of acetabular center of rotation. AP anteroposterior.
Anteroposterior standing radiograph demonstrates a superior augment placed in a “flying buttress” position for increased superolateral cup coverage.
For severe medial acetabular defects in which a hemispherical cup will be used, 2 wedge augments may be placed side by side as a medial “footing” (Fig. 15).
Printed 3D pelvis with 2 augments placed medially without screws in a “medial footing” configuration.
Another option for a larger medial wall defect is a smaller acetabular cup as medial support, or a cup-on-cup configuration. The medial cup is impacted first to achieve medial support. The second cup is then reamed and impacted with supplemental screw fixation through both cups (Fig. 16a–c).
(a) AP standing radiograph demonstrates medial migration of the acetabular component. CT confirms intact acetabular rim without evidence of pelvic discontinuity. (b) Sagittal CT demonstrates preoperative templating for use of double cup configuration. (c) Postoperative AP standing radiograph demonstrates cup-on-cup configuration and restoration of anatomic hip center. AP anteroposterior, CT computed tomography.
Augments can be fixed first, while a trial acetabular component is in position. The final acetabular component is then tucked in against the fixed augment. Another option is placing the cup first and gaining initial stability with a combination of press fit and screws and then placing the augment secondarily. In this case, augments used in wedge orientation can be impacted and wedged against the positioned final acetabular component. In either case, the augments should be unitized to the component with bone cement where the augment and cup are in contact [4,43,51,80,137,178,196,242,255].
Buttress or column augments can be used when inadequate bone exists to restore the acetabular rim and when the column(s) must be reconstructed in the presence of poor-quality remaining bone [97]. Column augments achieve screw fixation in the iliac wing, bypassing deficient acetabular bone stock. In general, defects large than 3 cm in height from the native hip center or greater than 50% of the dome, which indicates column involvement, are best addressed with column augments rather than the smaller acetabular wedge augments discussed previously (Fig. 17a–b).
(a) Preoperative radiograph demonstrates the catastrophic failure of a revision acetabular construct with massive acetabular bone loss. (b) A 2-year postoperative radiograph demonstrates biologic fixation of hemispherical shell and column augment; a dual mobility bearing was used to reduce early stress on bone-implant interface, despite increased risk for dislocation in the setting of abductor insufficiency.
Large complex acetabular defects can also be addressed with a combination of simple wedge augments and column augments. Preoperative planning including the use of 3D printed pelvic models to determine augment placement and size is very beneficial and likely improves operative efficiency and execution (Fig. 18a and b).
(a) Preoperative anteroposterior radiograph demonstrating aseptic loosening of a cage construct with superior migration and osteolysis. (b) Postoperative radiograph demonstrates a highly porous revision cup with screws combined with 2 augments, an acetabular augment in a wedge position and a column buttress augment providing columnar support and fixation into the iliac wing. A dual mobility bearing was used.
In all cases of complex acetabular bone loss, CT scanning with 3D reconstruction can aid in the templating of augments and allow the surgeon to template for the size and shape of the augment [111].
Cages and rings
Although still used with evidence of moderate mid-term to long-term success [139,193,200], cages and rings are no longer considered the first choice for management of significant acetabular bone loss, especially in patients with pelvic discontinuity [146]. The lack of a bone ingrowth surface means that these components often loosen and fail over time [89,128]. Cages and rings can be used in older patients with limited life expectancy, radiation necrosis, and metastatic disease (Fig. 19).
Postoperative radiograph shows pelvic discontinuity and medial wall deficiency in a 95-year-old woman (Fig. 11 radiograph) treated with a primary cage and cemented monoblock cup with a dual mobility bearing.
Cup-cage constructs
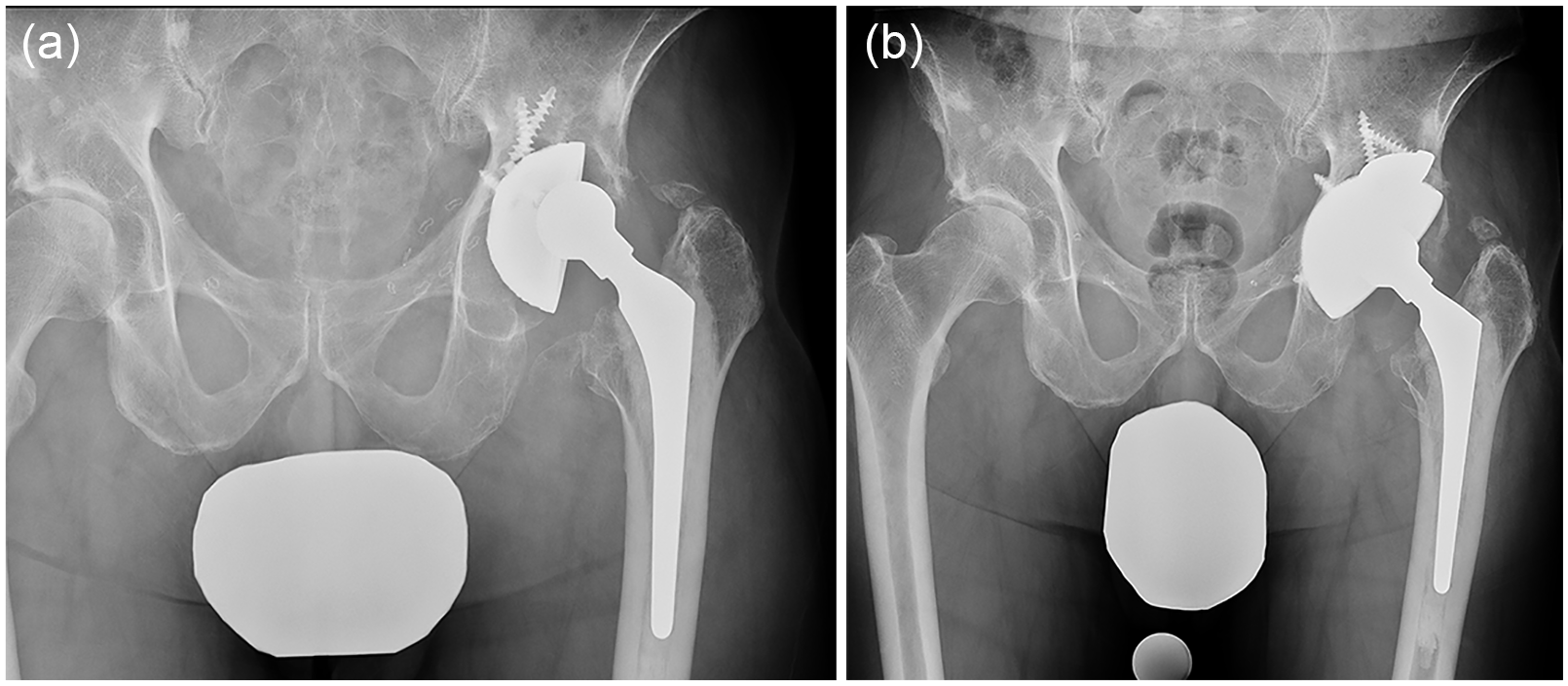
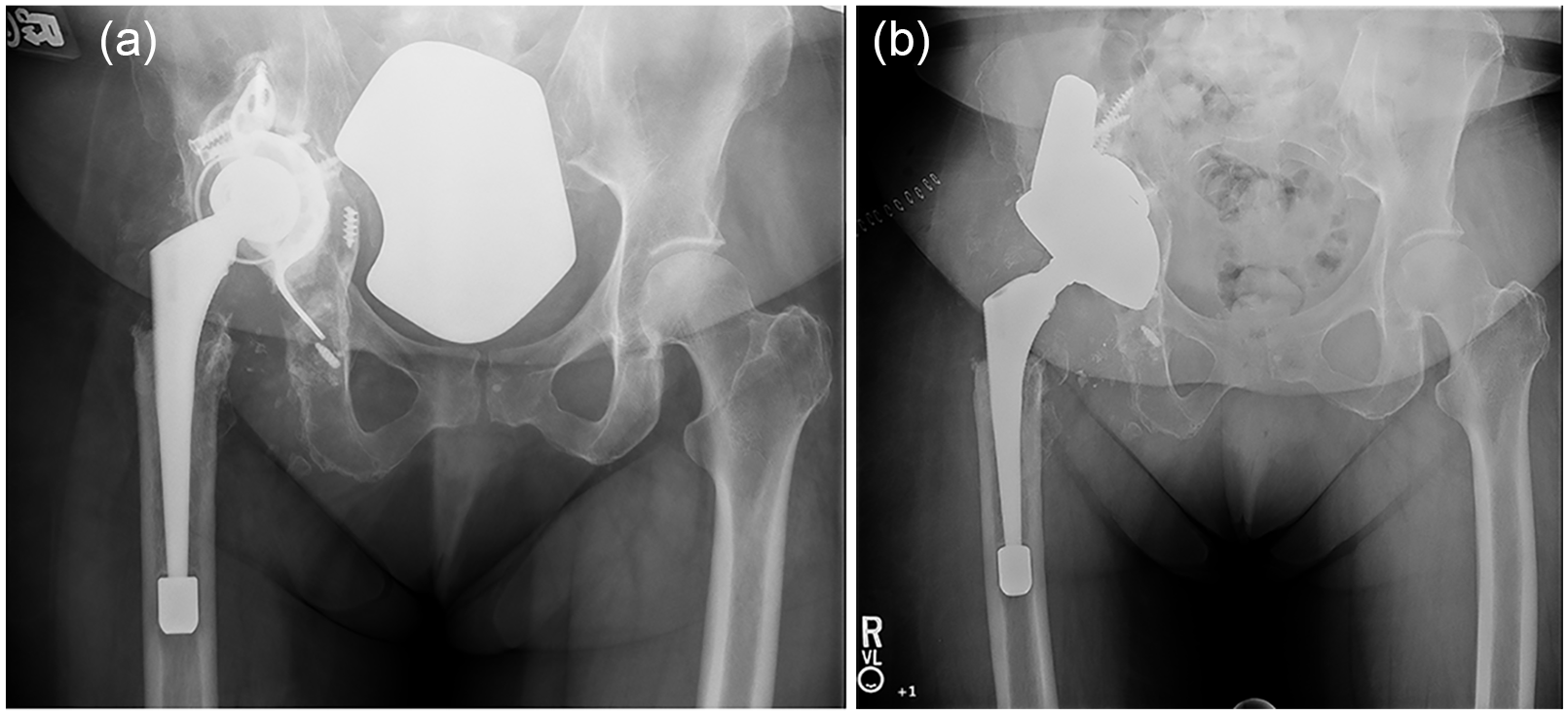
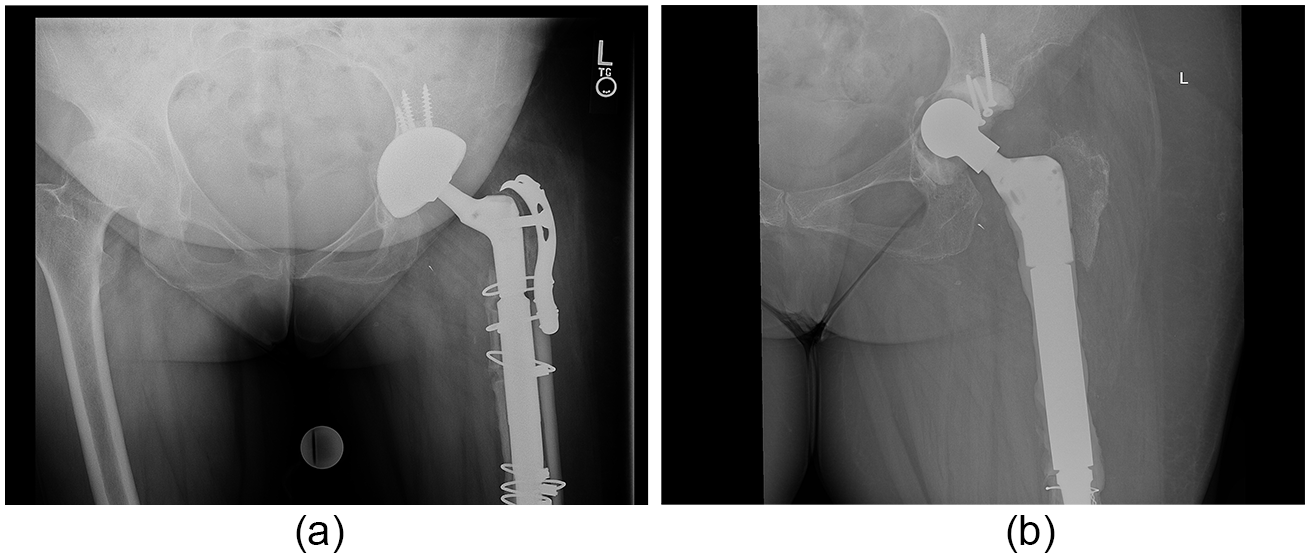
Patients with massive acetabular bone loss, particularly anteromedially, and those with pelvic discontinuity may be effectively managed with a cup-cage technique (half or full cup-cage) [3,45,93,127,152,208,220]. In these cases, the cup is placed first and serves as a biologic scaffold to assist with long-term implant fixation. The cage, either a half cage involving only the iliac flange or a full cage, is then placed over the cup, providing the immediate mechanical stability required for ingrowth. Recent data have shown equivalent results for both the half and full cage. Ischial fixation with screws is advised for all cup-cage constructs but especially when half cages are used (Fig. 20a and b).
(a) Preoperative AP radiograph demonstrates superomedial cup migration in a patient with prior posterior column fracture and associated pelvic discontinuity and medial wall deficiency. (b) Postoperative standing AP radiograph demonstrates half cup-cage reconstruction with replating of the posterior column with medial femoral head allograft. A monoblock cemented cup with dual mobility bearing was used. Replating of the posterior column was performed to provide provisional stability of an otherwise hypermobile pelvic discontinuity allowing for stable cup placement with a half cage for secondary mechanical stability. AP anteroposterior.
Cup-cages are especially suitable for patients who are unable to wait for the design and fabrication of a patient-specific device. Cup-cage reconstructions are technically difficult in patients with small acetabular sockets. Ischial fixation is a requirement for appropriate fixation of cup-cages; the ischial flange provides additional fixation but at the expense of potential complications including sciatic nerve injury. Recently, the use of half cup-cages has been advocated because they require less radical exposure and have less risk of complications, though only mid-term clinical results are available [208].
Bulk acetabular grafting
Use of bulk acetabular graft (eg, a femoral head or a “Fig. 7” graft [48,92,145,184]) is a less popular technique for severe cases due to lack of biologic incorporation and consequent fracture, migration, and resorption of grafts [71]. However, femoral head allografts are relatively inexpensive, easy to shape into more unusual defects, and may still have utility in severe cases in which they provide temporary stability while a hemispheric component achieves biologic ingrowth [239].
Impaction grafting
While impaction grafting has provided excellent results, it is a technically demanding procedure and should be performed by surgeons with experience in this technique [22,24,34,69,197,241,245]. Impaction grafting is best used when the acetabular bone loss is cavitary with contained defects. In noncontained defects, the grafting should be supplemented with mesh fixed with screws [16,30,33,62,94,113,259]. Impaction grafting can be used for rim and segmental defects but cannot be used in patients with pelvic discontinuity [33,113].
Patient-specific implants
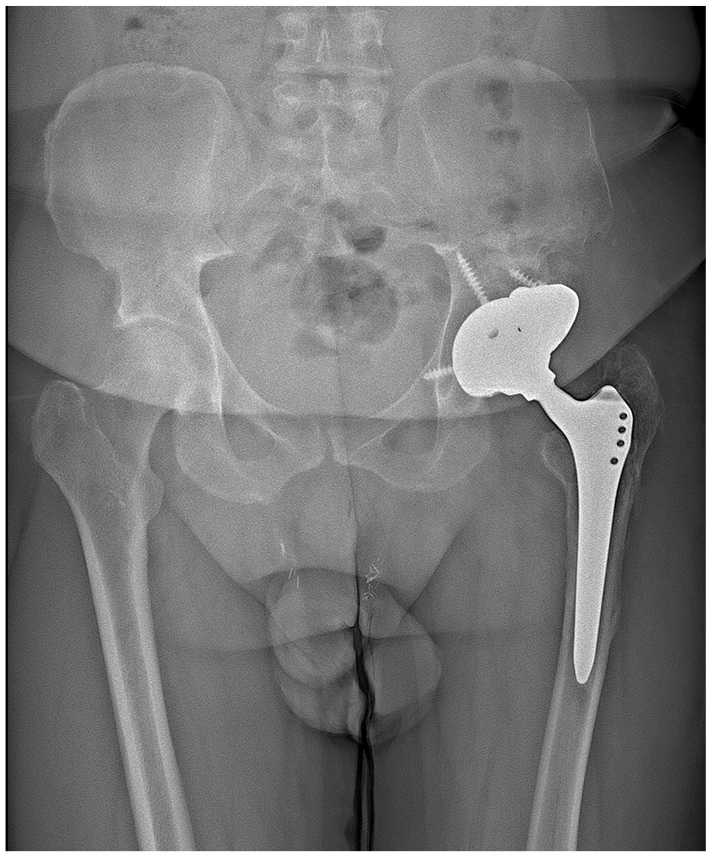
In massive acetabular bone loss with or without pelvic discontinuity, cup-cage and patient-specific triflange implants are the preferred treatments [146,220]. Patient-specific devices require extensive planning with engineers prior to surgery to create an implant that will span and reinforce the pelvic deficiency [6,8,13,17,31,86,110,115,120,147,166,170,171,247]. Severe pelvic bone loss in a patient with a small pelvis is a definite indication for a custom device because of the inability to obtain fixation with a large hemispherical acetabular component with or without augments. Limitations to the use of custom devices include the time delay required for design and fabrication, the high cost (although cup-cages can be similarly costly [231]), and the tendency to lateralize the hip center [126], which can be reduced with careful preoperative planning and custom fabrication [231]. Injury to the superior gluteal nerve may occur because of the need for extensive dissection to fix these devices into the ilium with multiple screws. To minimize this risk, the length of the iliac flange can be shortened to a length necessary to obtain adequate fixation. Also, angling the iliac screws superiorly helps limit iliac dissection. Iliac retractor placement should be minimized, slipping the iliac flange under the neurovascular bundle. If undue tension occurs, a flip trochanteric osteotomy should be used. Improvements are needed in bone growth surfaces and screw options, as well as improved design techniques that allow better implant-bone contact [195] (Fig. 21).
Postoperative standing radiograph demonstrates right custom acetabular component addressing a large complex acetabular defect (Fig. 7 case).
Management of Osteolysis
Debate exists over how often routine follow-up should be performed after total hip replacement, especially in patients who have asymptomatic osteolysis. Patients with conventional (nonhighly cross-linked) polyethylene should be followed up more frequently than patients with highly cross-linked polyethylene. In patients with conventional polyethylene, early follow-up is recommended at 8 to 12 weeks, and then yearly for 1 to 2 years and every 5 years thereafter. In patients with a highly cross-linked polyethylene as a bearing surface, routine follow-up may be unnecessary after the first year, so the next return could be at 10 years. In general, younger and more active patients should be followed up more frequently. Revision hip patients should be seen more frequently than primary hip patients to ensure the long-term fixation of revised components.
Once an osteolytic lesion is identified postoperatively, follow-up should be more frequent, as often as every 6 to 12 months, until a progression pattern for the osteolysis has been identified. Advanced imaging (MRI or CT) can be performed to define the extent of the lesion. The use of bisphosphonates has not been helpful in the treatment of asymptomatic osteolysis. If wear is significant, a femoral head and acetabular liner can be exchanged, with an attempt at grafting the lesions; the long-term results with this technique are unclear as there is limited evidence that the bone graft incorporates to underlying bone [198,222,225,262]. Scant data exist to suggest that bone grafting provides any lasting bone incorporation when placed into lesions behind a well-fixed acetabular component [19,81,207]. Sacrificing host bone by creating a bone window to access osteolytic areas, while an attractive approach, has not been efficacious and may be detrimental both to fixation and to adequately addressing the entire osteolytic lesion. Fixation of the acetabular component should never be compromised to allow better attempts at bone grafting.
A well-fixed acetabular shell should be preserved so that the femoral head size used at revision can be maximized to minimize risk of instability [198,262]. If the locking mechanism between the metallic shell and the polyethylene insert has been damaged or the available liner has a long shelf life and is not highly cross-linked polyethylene, a new highly cross-linked polyethylene liner can be cemented into the existing liner with good results, if done properly [44,90,186].
The following additional criteria should be considered for early intervention in asymptomatic osteolysis:
Significant eccentric wear such that the femoral head seems at risk of wearing through the polyethylene insert
Damage to the acetabular component locking mechanism
Significant progressive bone loss
Osteolytic lesions that jeopardize or have destroyed the posterior column and ischium
Osteolytic lesions in the load bearing region of the acetabulum
Lesions that may jeopardize future pelvic reconstruction and lesions large enough to involve more than 50% of the surface area of the implant-bone interface should be treated aggressively. Judet views and advanced imaging with a CT scan can be helpful in demonstrating the extent and location of osteolysis (Fig. 22a-b).
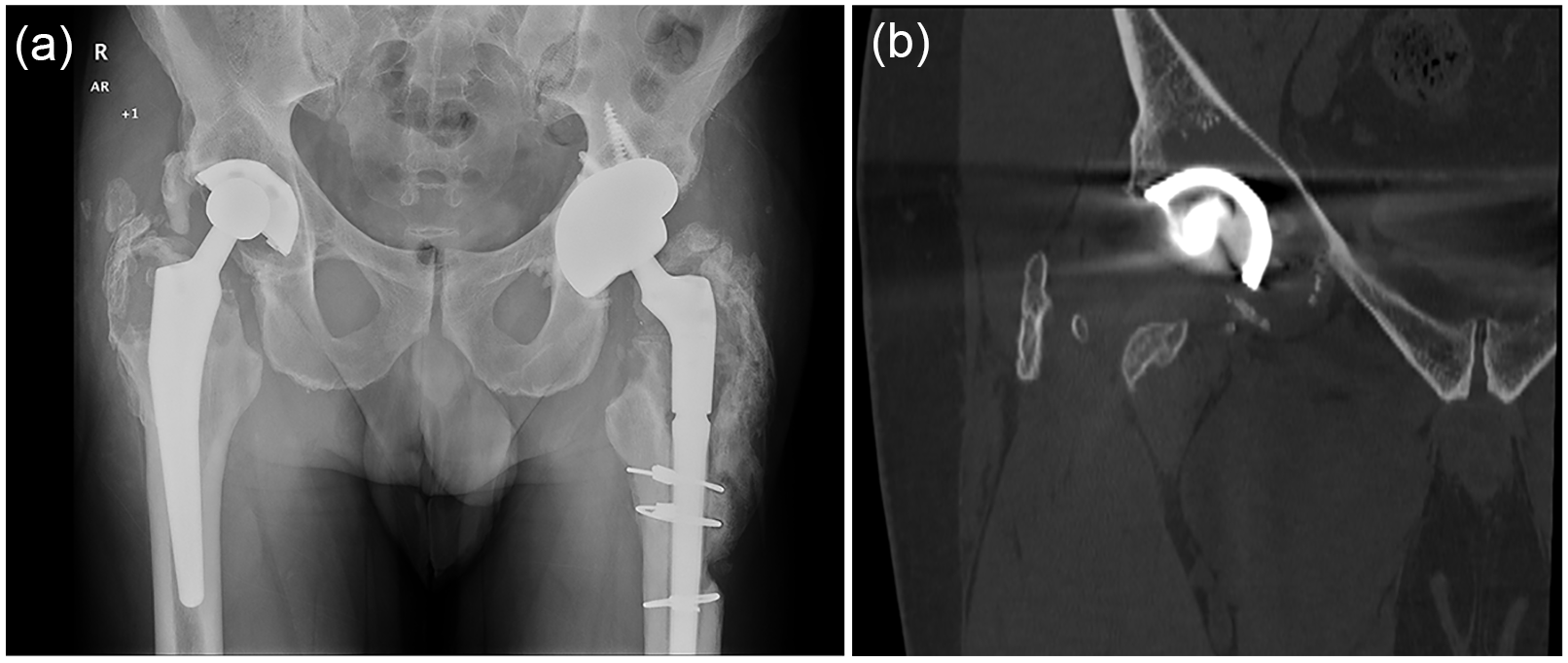
(a) Anteroposterior pelvis radiograph and (b) computed tomography coronal image demonstrating anteromedial osteolysis in an otherwise well-fixed acetabular component that was treated successfully with bone graft and cup retention.
All efforts should be made to retain the acetabular component if it is well fixed and well positioned [198,262], if no radiolucent lines or migration of the implant are seen on serial radiographs, or if radiographic evidence exists of spot welds between the bone and the component [19]. When revising an acetabular liner in a well-fixed component, the largest femoral head size available should be considered to maximize stability [18,262].
In addition, the acetabular component should be revised if the metallic shell cannot accommodate insertion of a new polyethylene liner using the existing locking mechanisms or if cementation of a new liner into the shell is not feasible [198,262]. As a rule, a well-fixed component should not be removed for the sole purpose of accessing osteolytic lesions. Conversely, if a component is malpositioned so that a cemented liner cannot be placed in an appropriate position, component removal is warranted [198,262]. If the shell is retained and a small head (28-mm diameter) is used, stringent hip precautions should be followed for as long as 3 months, and the patient should be counseled on dislocation risk.
Bone bed preparation, removal of particulate debris, and surgical technique are paramount to successful bone grafting of an osteolytic lesion [298,262]. Large particle (4–5 mm in diameter), fresh frozen allograft bone (eg, a femoral head) vigorously impacted into host bone has proven to be most effective [81,90,179,207]. The priority intraoperatively should be to achieve adequate rigid fixation of the implant onto host bone (often with multiple screw fixation in multiple quadrants). The graft should not interfere with component contact to host bone as fixation of the component onto the graft alone is insufficient to produce osseous integration and acceptable fixation. Cementless porous metal components are preferred.
Surgical Treatment of Massive Bone Loss
Contact between the anterior inferior iliac spine and the ischium is fundamental to a stable reconstruction in patients with marked acetabular bone loss. Data exist demonstrating inferior results with poor ischial fixation [195]. The status of the ischial bone is critical, and therefore, CT scanning with 3D reconstructions and modeling are quite helpful in these cases [195]. If ischial bone support is poor, bone grafting or augmentation can be useful in improving implant fixation to the ischium. Alternatively, reconstruction with a higher hip center can be performed as long as cup stability is achieved between the anterior inferior spine and the junction of anterior column and ilium.
As a rule, most massive acetabular bone loss cases can be reconstructed. Cases are made most challenging by pelvic discontinuity, severe ischial or iliopubic osteolysis, an inability to easily achieve 3-point fixation about the socket, and component migration greater than 2 cm above the base of the original reconstruction (from the top of the obturator foramen). The most difficult pelvic reconstructions are in patients with poor host bone and nonviable or irradiated bone that must be bypassed by the fixation. Patients with persistent and current infection who have poor soft tissue coverage are also difficult reconstruction cases, and for them, the priority is to eradicate the infection. An algorithm using CT scan data to determine the AP dimension of a hemisphere and to evaluate the surrounding bone loss volume and the quality of the remaining bone can be useful to guide the choices of implants and augments required to fill the defect.
Panel 3: Additional Treatment Challenges: Pelvic Discontinuity, Periprosthetic Joint Infection, Instability, Poor Bone Biology
Treatment of Acetabular Bone Loss With Pelvic Discontinuity
The definition of an acute pelvic discontinuity is an intraoperative fracture and/or a perioperative acetabular fracture that occurs in previously viable and structural acetabular bone stock [181]. For acute discontinuities that occur and are identified intraoperatively, consideration should be given to cup removal and inspection of the fracture, combined with internal fixation if feasible [144]. The selected hemispherical cup may then be inserted. If identified postoperatively, nondisplaced discontinuities may be treated initially with limited weight bearing. Operative treatment should be with open reduction and internal fixation using a compression plate and screws if the fracture can be reduced with enough bone stock and adequate bone biology to support fixation and primary fracture healing [218]. In cases of acute discontinuity with poor bone stock, treatment with a cup-cage using supplemental fixation (eg, superior and inferior screws) or a jumbo cup (also with supplemental fixation) should be considered [208,210].
Treatment modalities with the greatest efficacy for chronic pelvic discontinuity
The surgical goal when treating a chronic pelvic discontinuity is obtaining rigid acetabular component fixation and stabilizing the discontinuity to allow for eventual implant osseointegration and possible healing of the discontinuity, or at least unitization of the inferior and superior hemipelvis [2,16]. The advantages in using a cup-cage are versatility, the potential for biologic fixation, and availability (thus eliminating the production time required for a patient-specific implant) [3,45,40,61,93,98,127,152,153,208]. The disadvantages of a cup-cage are that the surgery is technically demanding and the use of a full cage may dictate the orientation and position of the component [61]. The half cup-cage, in which the ischial flange is removed and inferior fixation is achieved with screw fixation through the acetabular shell, has had some favorable reports [50,199] and may be considered a surgical option. Potential benefits include more limited ischial dissection, avoidance of ischial bone fracture with flange insertion, and minimal adjustments in cup placement to accommodate iliac flange placement [199].
The pelvic distraction technique can be used with a hemispherical cup alone, a cup and an augment, or a cup-cage reconstruction [15,50]. The goal is to gain an interference fit across the mobile discontinuity through distraction and ligamentous recoil [50]. For this reason, pelvic distraction should be used with caution in hypermobile pelvic discontinuity. It is contraindicated in bilateral pelvic discontinuities because overdistraction can occur in these unique cases due to insufficient elastic recoil. The current literature on distraction is limited, but early results with this technique have been encouraging [17,50,146]. Patient-specific implants (eg, triflange or biflange acetabular components) also have advantages and disadvantages [195,220,253]. They are expensive, although Taunton et al [231] reported that the costs of patient-specific triflange implants and trabecular metal cup-cage constructs were equivalent. Patient-specific implants require long preparation times (2–4 months) for design and production, require active participation with input from the surgeon and an engineer in planning, and usually require a more extensive surgical exposure [126]. Conversely, the advantages of patient-specific devices are the ability to accommodate many sizes and shapes of acetabular bone loss, the ability to accurately restore the hip center of rotation and precisely control acetabular component orientation, and the ability to incorporate different bearing options, such as dual mobility and constrained components [58,170,231].
Special considerations when managing chronic pelvic discontinuity
Acetabular hypermobility that can occur in the setting of chronic pelvic discontinuity requires rigid fixation that bridges the discontinuity. A highly porous acetabular component or custom implant should be employed with supplemental fixation (eg, screws, flanges, or augments), and the fixation should be extended both above and below the area of discontinuity. Acetabular distraction should be used with caution in patients with hypermobility across the pelvic discontinuity as overdistraction may occur leading to neurovascular compromise with excessive ischial distraction.
Acetabular Bone Loss in the Setting of Periprosthetic Joint Infection
Constructing an antibiotic-impregnated cement spacer as part of a 2-stage exchange
Infection eradication takes priority over bone loss management when faced with a periprosthetic joint infection [235]. Articulating spacers have a role in contained or semi-contained defects, with the advantages of maintaining length during treatment, increasing patient comfort, and, of course, providing local treatment through antibiotic elution from the cement [1,84,130,213,235,236]. Disadvantages of spacers include risk of dislocation or spacer fracture and the persistent presence of a foreign body in the joint after antibiotic elution is complete [11,130,213,236].
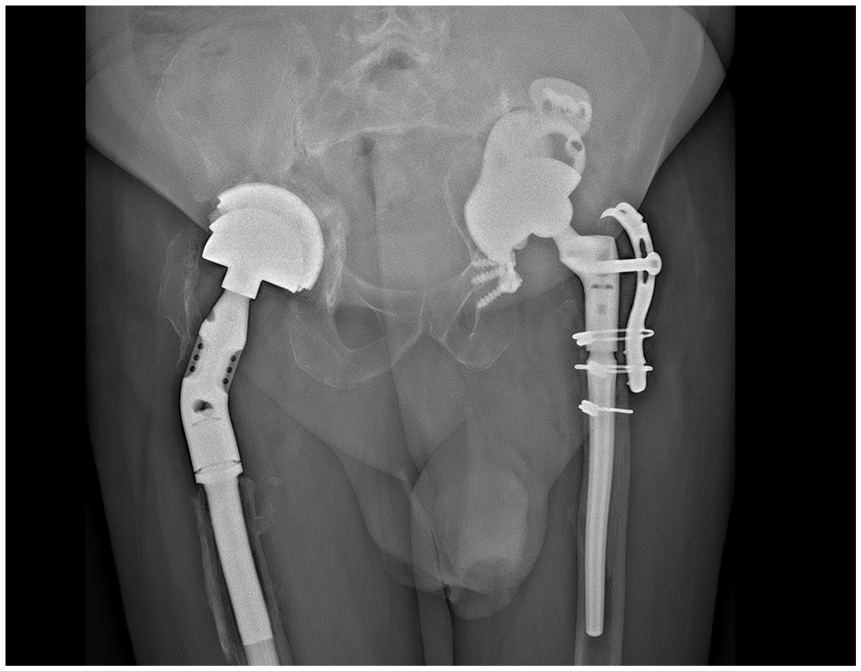
A nonarticulating spacer is most useful in the case of severe acetabular bone loss where weight bearing ambulation with an articulating spacer would compromise the second stage reconstruction. The disadvantages of nonarticulating spacers include patient discomfort, inferior function, and the difficulty at reimplantation secondary to more difficult surgical exposure, as well as restoring leg length due to proximal femoral shortening [36]. Nonarticulating spacers should not be used in the presence of uncontained defects, pelvic discontinuities, and in cases where the abductors and other soft tissues are significantly damaged and the risk of hip spacer instability is high, or when the host is poor or the bacterium is unknown or resistant [36,74] (Fig. 23).
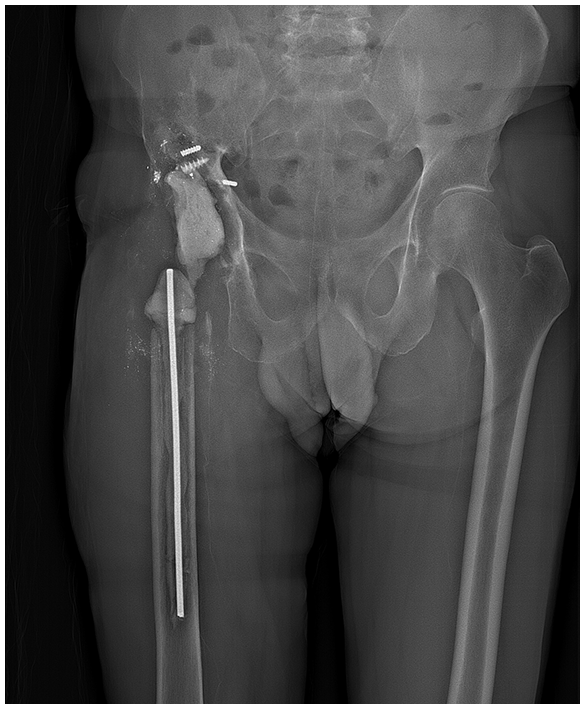
Anteroposterior standing radiograph of a static nonarticulating spacer shows massive acetabular bone loss and abductor deficiency.
Resection arthroplasty also has a limited role after multiple failed attempts at using a spacer. This approach eliminates both the presence of a foreign body and the risk of dislocation but is often painful and severely limits ambulation and limb shortening is a persistent problem [82]. It should be reserved for salvage cases only.
Creating a stable spacer in the setting of significant acetabular bone loss
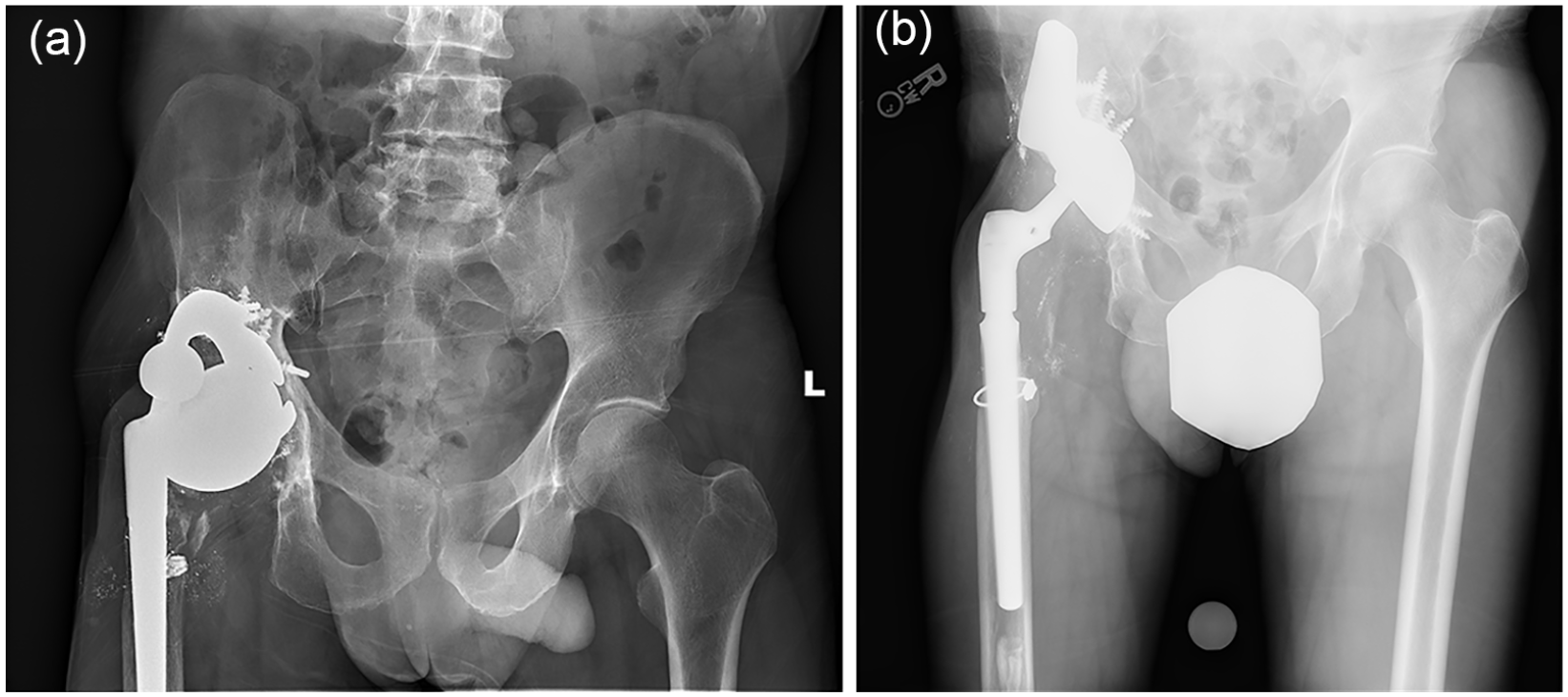
Hemispacers have the advantage of a large femoral head component filling the socket but can increase risk of further acetabular bone loss due to abrasive bone destruction and/or dislocation. An articulating spacer can be used, but ideally, a constrained element to the spacer is required. Screws or cement-staged augmentation may be required in severe acetabular bone loss cases [1,84,130,213,236] (Fig. 24a and b).
(a) Preoperative anteroposterior radiograph demonstrates a large hemispherical shell with medial wall deficiency. (b) Postoperative X-ray shows segmental implant coated with antibiotic cement and a cemented cup using multiple screws as “rebar” to reinforce the superior cement augmentation.
Severe acetabular bone loss in the setting of chronic periprosthetic joint infection treatment
The choice of whether to perform debridement, antibiotics, and implant retention (DAIR) or a 1-stage or a 2-stage exchange should not affect the primary goal of treatment: Infection must be treated first, and then, the acetabular bone loss must be addressed. Of course, DAIR applies only with well-fixed osseointegrated implants [155,251]; if mechanical loosening exists, an alternative treatment is required to deal with this problem. Occasions arise in which a 1-stage exchange must be converted to a 2-stage exchange because of an unexpected amount of acetabular bone loss [36]. However, while the size of the acetabular bone defect is not a contraindication to a 1-stage exchange, carrying out this procedure will require augmentation and advanced reconstruction techniques.
Acetabular Bone Loss and Minimizing the Risk of Instability
Femoral head diameter in revision surgeries
To ensure stability, the largest “effective” head size should be used with either a conventional or a dual mobility construct [190]. However, one must understand the minimum thickness of polyethylene for each head size and adjust decisions accordingly [38,46,194]. For example, a revision in an elderly patient versus in a young, active patient will have different polyethylene thickness requirements for long-term success.
Bone loss and increased risk of dislocation, bearing choice, and associated soft tissue and muscle damage
Both bony and soft tissue insufficiency play a role in hip instability. The indirect consequences of acetabular bone loss are the variability in the hip center and the orientation of the acetabular component. The amount of soft tissue damage is related to the primary pathology, for example, an infection or an ALTR, and to the previous surgical exposure. Dual mobility or constrained socket selection can help reduce dislocation risk in these cases [190].
Failure to restore the hip center and malpositioning of the acetabular component can both increase the postoperative risk for dislocation. Unfortunately, the inclination and version of the component is often dictated by the relative positions of the reconstructing device (eg, a cup-cage) and the remaining bone around the acetabulum. Intraoperative radiographs are helpful to adjust positioning before the final fixation of the acetabular component. Elevated rim liners can be used to adjust acetabular component position and provide additional stability [187]. Also, additional socket stability can be achieved with fully constrained or dual mobility bearings that can help in the setting of less optimal positioning or compromised soft tissue [190].
The use of dual mobility bearings and constrained acetabular liners in acetabular revision
When suitable, a dual mobility socket should be routinely considered in the revision setting [103,112,119,134,148,206,209,250,256,257]. In the case of cup-cages, polished dual mobility liners are being developed that can be cemented into the cage [85,258]. Constrained acetabular liners should be considered a salvage device, but optimal component position is critical to their success as the range of motion with these devices can be more limited [114,124]. Major abductor loss can be an indication for use of a constrained liner versus a dual mobility construct [21,190]. Constrained liners should be also considered when other options have previously failed (eg, a previous dual mobility construct). Secondary abductor reconstruction via tissue transfer can be used to manage soft tissue deficiency around the hip [21,25]; however, further research is needed to address how to best characterize deficiency and to define what the consequences of a deficiency are to clinical outcomes.
An acetabular construct with a constrained liner has a significant potential for failure [29,104,107]. An intraoperative judgment must be made to determine if adequate component fixation has been achieved. Limited range of motion and component impingement are major downsides of constrained sockets, which must be appreciated intraoperatively to lessen risk of failure of the constrained devices. While a high risk of failure with a constrained liner could be theoretically expected, little data exist to quantify this risk. A reasonable strategy to reduce potential failure of a constrained device is to emphasize the bony incorporation over stability by the use of a conventional bearing and bracing, in addition to patient education; a more constrained option can be chosen later if the need seems justifiable.
Cementing a new liner or a dual mobility liner into an existing well-fixed acetabular component
The results of cementing into a retained well-fixed acetabular component are quite good whether one uses a dual mobility type liner or a conventional polyethylene liner [42,44,90,129,156,186]. Crucial to the success of this procedure is to allow for an ample cement mantle (1–2 mm thick circumferentially) and to create adequate grooves or a roughened surface for cement interdigitation [121,157]. Increased failure has been reported if insufficient cement is available at the periphery of the new liner or if the liner is not well seated within the existing metal shell.
Acetabular Bone Loss With Compromised Bone Biology
The effect of prior radiation and its influence on choice of reconstruction
Prior irradiation of the acetabular bone can negatively affect the results of the subsequent reconstruction [59,131,248]. Two successful approaches include the use of a highly porous component with supplemental fixation (eg, screws or augments) or extending the fixation beyond the field of radiation (eg, with the use of a triflange or buttress) [47,59,167,168,247,266]. Use of a primary cup-cage construct can also be considered.
The effect of an ALTR failure on the results of acetabular reconstruction
The presence of an ALTR (eg, secondary to the presence of a metal-on-metal bearing or to corrosion at a taper or dual modular neck junction) can have a significant effect on bone loss and the biology of the remaining bone tissue (bone necrosis) [125]. Similarly, ALTR can profoundly affect soft tissues, which in turn affects surgical planning and outcomes, particularly joint stability and the risk of subsequent dislocation secondary to abductor damage and insufficiency [265,267].
Surgical techniques and implant and biologic materials to address poor bone quality
When faced with poor bone quality, solutions are limited but include use of the following:
A hemispherical cup with a highly porous ingrowth surface combined with supplemental screws, augments, or a cage, as needed;
Hydroxyapatite coating on a hemispherical cup with a roughened surface or on a cup with a highly porous ingrowth surface, again with supplemental screws and augments;
A patient-specific implant.
Additional considerations for patients with osteoporosis or other metabolic bone disorders
The more viable the underlying bony bed, the better the overall bone environment will be for implant fixation and stabilization [226]. Pharmacologic measures (such as teriparatide injections) to improve bone metabolism may be helpful, but additional research is needed to address this question [32,87,108,188,219,223,260].
Panel 4: Principles of Reconstruction and Classification of Bone Loss
Principles of Acetabular Reconstruction
Cementless fixation in acetabular revision
The primary principle of revision acetabular surgery with bone loss is to achieve stable fixation as a press fit or “pinch” between the anterior-superior and posterior-inferior regions of the acetabulum. This so-called “pinch” mechanism should then be supplemented with screw fixation. This, in effect, creates a third point of fixation. If screw fixation proves inadequate, additional techniques are necessary (eg, addition of a supplemental cage). The success of acetabular augments has allowed for the use of smaller components in a near anatomic position combined with augment restoration of missing bone stock.
The amount of host bone ingrowth required for long-term durability
The amount of contact between a revision component and the adjoining bone of the acetabulum that is necessary to secure adequate initial fixation and promote sufficient subsequent bone ingrowth is unknown. Assessing contact through imaging techniques is difficult, and therefore, no reliable data are available. Nonetheless, studies of the percentage of ingrowth around well-fixed primary acetabular components retrieved at autopsy with early generation titanium fiber mesh coatings were only 12% on average [243], suggesting that little ingrowth is necessary for adequate, stable fixation. More recently, a study of retrieved acetabular components with the more recent porous tantalum coatings also showed low percentage of ingrowth in stable implants [162].
Factors that influence the percentage of host bone contact
Several factors influence host bone contact with a revision acetabular component. These include the following:
Location of remaining host bone in the acetabulum;
Quality of the host bone tissue;
Quality of screw fixation that can be obtained to coapt remaining bone to the acetabular component; and
Features of the component and its fixation surface (eg, the overall stiffness and shape of the component, the amount and shape of the porosity on the fixation surfaces of the component, and the coefficient of friction of the porous surface that contacts the host bone).
Although contact with host bone is essential to fixation, coverage of the entire acetabular component with host bone is not. As discussed earlier, leaving part of the acetabular component uncovered superolaterally is acceptable, if doing so provides adequate positioning and orientation. As a rule, the focus should be on the best support by the host bone and not necessarily on the percentage of coverage of the component by bone. Bone loss can be thought of as a “glass half full or glass half empty” conundrum. Knowing the quality host bone available for reconstruction will guide the plan (eg, where to place screws for fixation or whether a patient-specific device will be necessary). Conversely, knowing what host bone is missing will guide the planning of what must be added to achieve adequate fixation.
Reconstructing the joint center of rotation
In the face of acetabular bone loss at revision surgery, it is not always necessary to reconstruct the native acetabular center of rotation. Nonetheless, clinical data show that moving the joint center laterally is associated with subsequent failure of the reconstruction [126]. Shifting the center of rotation superiorly is acceptable, but lateralizing the center of rotation should be avoided. Be aware of the neck length of the femoral component when considering the location of the hip center of rotation, especially in situations in which it is advantageous to maintain a well-fixed femoral component, even though it may have a long neck.
Avoid sacrificing structural bone that could be used for fixation, and place the component where the contacting host bone will be of the best quality. It is better to move toward a smaller component that allows preservation of high-quality remaining bone. In acetabular revision surgery, a trend has emerged in which far fewer acetabular components with diameters of 70 mm or greater are employed. Areas of bone loss in these settings can be augmented superiorly or, if necessary, defects can be filled with bone graft rather than losing bone with a larger component [174].
Achieving pubic-ischial fixation using a hemispherical cup
The failure mode for most acetabular components is “up and out” with loss of inferior fixation (DeLee and Charnley Zone 3) [77,147,99,185,228,230].
In acetabular revision, reestablishing solid and immediate zone 3 fixation is fundamental to long-term success of the reconstruction [77,230]. Zone 3 fixation can be achieved with the hemispherical shell alone if enough ischial bone stock exists for scratch interference fit. If ischial bone stock is nonsupportive, additional zone 3 fixation is required. Supplemental fixation can be achieved with ischial screw fixation through the acetabular component [229]. Rigid zone 1 fixation can also be achieved with the use of a cage placed over the cup with either impaction of the ischial flange into the ischium or screw fixation through the cage into the ischium when the ischial flange is laid on top of it [52,100,163]. Rarely, acetabular augments can be used to reestablish structural support of the ischium with the cup and then pressed fit into this augmented ischium [101]. Regardless of the technique used, the principle of achieving satisfactory zone 3 fixation for long-term durability of cementless acetabular components is the same.
Locking versus nonlocking screws for component fixation
The minimum number of screws needed for fixation is not defined, but as a rule, the more the better, and this number will vary depending upon the severity and location of the bone loss and the bite of the screws into the bone tissue during insertion [161,214,263]. To increase the strength of the fixation, bicortical screw purchase is preferred over cancellous or unicortical purchase [99]. The indication for the use of locking screws over conventional cancellous screws, even in a flanged acetabular component, is unknown [60,64,96,214]. Further research is required to determine the additional fixational benefit of locking screws versus nonlocking screws.
Optimal materials and design features for acetabular components in revision surgery
The implant components for acetabular reconstruction in the face of significant bone loss require more well-defined design specifications. Currently, the amount and type of porosity and the coefficient of friction of modern porous materials are considered to be more important design considerations than the overall stiffness of the component. There is controversy concerning the role of component stiffness in long-term clinical outcomes [12,27,28,151,161]. Indeed, less stiff components, because of their deformability, may “grab” the bone better during insertion than stiffer components, so that compliance of the component improves stable initial fixation. Fully porous titanium or tantalum shells that do not have a modular locking mechanism to allow for optimized elasticity may enhance initial fixation and subsequent bone ingrowth [11,12,23,37,67,151,180,191,201,202,233].
Highly porous, nonmodular revision acetabular shells
Acetabular shells through which holes can be drilled allow screws to be placed anywhere through the acetabular component [180,201]. This is beneficial for gaining ischial fixation, which often does not align with the allotted holes in a multihole shell. In addition, with significant bone loss, screw placement can be customized to target the best areas of remaining bone stock. The liner can then be cemented into the shell, which creates a fixed angle construct for the acetabular screws. The disadvantage of nonmodular revision shells is that they do not provide the options of modular liners, which can accommodate varying levels of constraint, from a large head to a dual mobility, or fully constrained, liner. Dual mobility shells designed for cement fixation are available, but if this construct were to fail, conversion to a constrained liner would require removal of the cemented dual mobility liner rather than a simple modular liner conversion.
Classification of Acetabular Bone Defects
Current classification systems
Classification systems are, in effect, tools for systematic categorization [246]. Their purpose is to help the surgeon choose an appropriate method of treatment for different situations; the classification tool should provide the surgeon with a reasonable estimation of treatment outcomes [254]. In addition, the classification should be reproducible and have good interobserver and intraobserver reliability and allow for reliable comparison of results across studies [20,254]. Most classification tools require a diagnostic image such as a radiograph, based on which observations or measurements are made [26,114,264]. These data are then compared with a published set of rules, which provides the instructions for determining the appropriate classification tools. This approach usually requires both subjective and objective interpretations. The output of the classification tool (the grade or class) is then used to suggest, hopefully based on well-documented scientific clinical evidence, a method of treatment and a most probable outcome [254].
A few classification systems exist for acetabular bone loss [20,26,182,273]. Their strengths include widespread familiarity, the need for only routine perioperative radiographs, and their application in many studies of mid-term and long-term outcomes in the literature [20,254]. Their weaknesses include the following:
A reliance on radiographs instead of more advanced imaging such as CT or MRI [39,79,95,203,269];
Limited usefulness intraoperatively after component removal;
A lack of clear guidelines to determine reconstruction with current techniques and implants [254];
Moderate to poor interobserver and intraobserver reliability (for most available classifications) [28,79,182,203,264].
Important factors for a classification system
Several other factors should be included to create a successful classification system that adequately assesses the host bone available for fixation. Ischial and teardrop lysis is an important warning sign to be heeded in planning reconstruction [192]. Pelvic discontinuity will also markedly affect reconstruction [146] as will the status of abductor muscles and other soft tissues surrounding the hip [149]. Other factors, such as the quality and the biology of the bone tissue, would be important to include; however, this may have to await better assessment tools. A revised classification system needs to be developed and was 1 of the strong recommendations of the group.
Treatment guidelines that could form the basis for a classification system
To improve the applicability of a classification system to guide treatment, it might be best to consider 2 sets of guidelines: 1 set for preoperative assessment and consideration of reconstruction options and a second set of guidelines for intraoperative decision-making and final reconstruction.
Preoperative assessment
Preoperative guidelines could be based on radiographic assessment of component migration, defined as the vertical distance from the base of the teardrop to the center of rotation of the component. The main goal of this assessment is to direct the need for advanced imaging as part of preoperative planning.
For example, 1 class of cases are those for which minimal vertical migration (eg, <2–3 cm) has occurred. These cases will not require advanced imaging. A second class of cases would be those with vertical migration that exceeds the minimal amount (eg, >2–3 cm). Adequate preoperative planning requires advanced imaging for these cases, especially to assess whether the migration is superolateral (so called “up and out”) or superomedial (so called “up and in”). A final class of cases would be those with pelvic discontinuity. These cases also require advance imaging.
The following considerations prompt the need for advanced imaging:
Medial migration of screws or cement (CTA is advised to locate and assess compromise of the intrapelvic vessels);
Obliteration of the teardrop;
Ischial lysis;
Lytic lesions measuring more than 2 to 3 cm in any of the 3 bones of the pelvis;
The presence of an oversized component;
Gross malpositioning of the existing component;
Asymmetry of the hemipelvis.
Intraoperative guidelines
Intraoperative findings and guidelines that drive treatment during revision surgery include the following:
If a large portion of the acetabular component is uncovered, consider supplemental fixation and/or augmentation. Evaluate the ability to achieve a “pinch” press fit.
If the previous component had migrated “up and in” by less than 2 to 3 cm, the treatment can be a press-fit jumbo hemispherical component.
If the previous component has migrated “up and out” by more than 2 to 3 cm, additional techniques should be considered to enhance fixation and/or coverage. This may include superior augmentation, which will improve component stability and coverage and restore the hip center of rotation.
If the treatment is for a failed acetabular component that has migrated “up and in” by more than 3 cm, a column augment with inferior screw fixation through the cup, a half or full cup-cage, or patient-specific custom component will probably be required.
Guidelines for choosing bearing surfaces
Preoperative and intraoperative classification systems do not address the choice of bearing surfaces. Constrained liners should be used with caution when component fixation is not optimal [190]. The general trend is toward increased usage of dual mobility to reduce the risk of dislocation, but long-term clinical data are not yet available [103,119,134,189,206,209,250,257]. A large ceramic femoral head bearing against highly cross-linked polyethylene remains the preferred bearing choice, despite increased utilization of dual mobility bearings.
Imaging
As a rule, advanced imaging with CT should be used for most patients with severe acetabular bone loss to determine the need for supplemental fixation based on 3D assessment. Radiographic assessment should generally include Judet views, which are extremely useful as a screening radiograph. Loss of the posterior column (with “up and out” migration) and excessive “up and in” component migration should always prompt advanced imaging (CT and/or MRI).
Straight medial (<2–3 cm of superior) migration from the obturator foramen usually reflects that the rim is intact, so CT imaging may not be useful for assessment of bone loss. When measuring for migration of greater than 2 to 3 cm, use the distance from the superior obturator foramen to the center of the femoral head.
Radiographic warning signs when considering the removal of a well-fixed component
Prepare for considerable iatrogenic bone loss when removing a well-fixed acetabular component. The following scenarios can be particularly problematic:
Oversized acetabular components, which on socket removal will likely lead to increased loss of the anterior or posterior walls;
A malpositioned component;
Contact with or violation of the medial wall.
Footnotes
Collaborators
The Acetabular Bone Loss Work Group consists of Matthew Abdel, MD, Friedrich Boettner, MD, Francesco Benazzo, MD, Martin Buttaro, MD, Daniel Choi, MD, Charles Anderson Engh, MD, Eduardo Garcia-Cimbrelo, MD, PhD, Eduardo Garcia-Rey, MD, Thorsten Gehrke, MD, William L. Griffin, MD, Erik Hansen, MD, William J. Hozack, MD, Stephen Jones, MD, Gwo-Chin Lee, MD, Joe Lipman, MS, Andrew Manktelow, MD, Alex C. McLaren, MD, Rob Nelissen, MD, PhD, Lawrence O’Hara, MD, Carsten Perka, MD, and Scott Sporer, MD.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter K. Sculco, MD, reports relationships with EOS Imaging, DePuy Synthes, Intellijoint Surgical, and Parvizi Surgical Innovation. Timothy Wright, PhD, reports relationships with Exactech and LimaCorporate. Mathias Bostrom, MD, reports relationships with Smith & Nephew and Ines Mandl Research Foundation. Farres Haddad, MD, reports relationships with Smith & Nephew, Corin, MatOrtho, Stryker, Bone & Joint Journal, and Annals of the Royal College of Surgeons. Seth Jerabek, MD, reports a relationship with Stryker. Michael Bolognesi, MD, reports relationships with Zimmer Biomet, Exactech, DePuy Synthes, Stryker, American Association of Hip and Knee Surgeons, Total Joint Orthopedics, Eastern Orthopaedic Association, Smith & Nephew, the Pulmonary Embolism Prevention after Hip and Knee Replacement trial funded by Patient-Centered Outcomes Research Institute. Thomas Fehring, MD, reports a relationship with DePuy Synthes. William Jiranek, MD, reports relationships with DePuy Synthes, Moximed, Hip Society, and BioMech Sensor LLC. William Walter, MD, reports relationships with DePuy Synthes, MatOrtho, and NavBit, and has several patents pending or issued. Wayne Papropsky, MD, reports relationships with Zimmer Biomet, Innomed, MicroPort Orthopedics, Intellijoint Surgical, and CeramTec. Thomas Sculco, MD, reports relationships with Exactech and LimaCorporate. Matthew Abdel, MD, reports relationships with Stryker and American Academy of Orthopedic Surgeons. Friedrich Boettner, MD, reports relationships with Smith & Nephew, Ortho Development, and DePuy Synthes. Francesco Benazzo, MD, reports relationships with Zimmer Biomet, LimaCorporate, Fidia, and JACE Medical. Charles Anderson Engh, MD, reports relationships with DePuy Synthes, Smith & Nephew, and Zimmer Biomet. William L. Griffin, MD, reports relationships with DePuy Synthes and Hyalex Corporation. Eric Hansen, MD, reports a relationship with Corin. William Hozack, MD, reports a relationship with Stryker. Stephen Jones, MD, reports relationships with Smith & Nephew, Adler, DePuy Synthes, Zimmer Biomet, Orthofix, and British Hip Society. Gwo-Chin Lee, MD, reports relationships with Stryker, Corin, Heron Therapeutics, Smith & Nephew, DePuy Synthes, KCI USA, Journal of Arthroplasty, Clinical Orthopaedics and Related Research, Journal of Bone & Joint Surgery, Bone & Joint Journal, and the Knee Society. Andrew Manktelow, MD, reports relationships with Zimmer Biomet, MatOrtho, Orthofix, British Hip Society, British Orthopaedic Association, International Hip Society, and European Hip Society. Alex C. McLaren, MD, reports relationships with Arizona Governor’s Grant, National Institutes of Health, Orthopaedic Trauma Association, MusculoSkeletal Infection Society, Sonoran Biosciences, and Hayes Diagnostics. Lawrence O’Hara, MD, reports relationships with Zimmer Biomet. Carsten Perka, MD, reports relationships with DePuy Synthes, Zimmer Biomet, Smith & Nephew, German Society for Orthopaedics and Orthopaedic Surgery, and General Secretary German Arthroplasty Society. Scott Sporer, MD, reports relationships with DJO Surgical, Osteoremedies, Hip Society, Knee Society, and Myoscience. Michael-Alexander Malahias, MD, Alexander Gu, MD, Alejandro Gonzalez Della Valle, MD, Donald Garbuz, MD, Martin Buttaro, MD, Daniel Choi, MD, Eduardo Garcia-Cimbrelo, MD, PhD, Eduardo Garcia-Rey, MD, Thorsten Gehrke, MD, Joe Lipman, MS, and Rob Nelissen, MD, PhD, declare they have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Acetabular Bone Loss Work Group and HSS Journal received financial support for the research, writing, and publication of this article from the Stavros Niarchos Foundation Complex Joint Reconstruction Center at Hospital for Special Surgery.
Level of Evidence
Level IV: Opinion of expert consensus panel based on scientific evidence.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.