
Abstract
Background:
Lumbar spinal canal stenosis surgery has recently improved with the use of minimally invasive techniques. Less invasive procedures have emerged, and microendoscopic decompression through smaller incisions is frequently performed. Tubular surgery with the assistance of endoscopic surgery procedures has led to particularly remarkable changes in surgery, with reduced tissue trauma and morbidity.
Purpose:
The purpose of this study was to compare the clinical outcomes of two different minimally invasive decompressive surgical techniques (microendoscopic bilateral decompression surgery using the unilateral approach [microendoscopic laminectomy (MEL)] and microendoscopy-assisted muscle-preserving interlaminar decompression (MILD; ME-MILD)) using spinal endoscopy for lumbar spinal canal stenosis measured using a visual analog scale (VAS), the Japanese Orthopedic Association (JOA) score, and the JOA Back Pain Evaluation Questionnaire (JOABPEQ), which is based on a patient-oriented scoring system.
Study design:
This study was a retrospective review of prospectively collected surgical data.
Methods:
The study included 81 patients (MEL 39 patients, 20 men and 19 women, mean age 68.9 years; and ME-MILD 42 patients, 22 men and 20 women, mean age 73.1 years) with lumbar spinal stenosis (LSS). The indications for surgery were moderate-to-severe stenosis, persistent neurological symptoms, and failure of conservative treatment over 3 months, with a JOA score under 15 points or intermittent claudication at 100 m. This study included patients having LSS at a single vertebral level (L4/5).
Results:
Low back pain, buttock-leg pain, and numbness were significantly improved in terms of the VAS score from 3 months with both MEL and ME-MILD. In all periods, JOA scores over 3 years of follow-up were significantly higher than those obtained before surgery with both MEL and ME-MILD, and there were improvements of low back pain and walking function.
Conclusions:
These observations demonstrate that ME-MILD is a safe and very effective minimally invasive technique for degenerative LSS, similar to MEL.
Keywords
Introduction
Lumbar spinal canal stenosis is one of the most common causes of spinal disorders in an aging society, causing claudication, buttock or lower extremity pain, and disability. 1 Deformity of the facet joints, hypertrophy of the ligamentum flavum, disc degeneration, and osteophytes cause the spinal canal to constrict and result in spinal cord and nerve root compression. The aim of lumbar spinal canal stenosis surgery is healing of leg pain and improved walking ability by decompression of the spinal canal. 2 There has been an increase in the number of lumbar spine decompression procedures performed for lumbar stenosis over the past decade. 3 The conventional approach for decompression is open laminectomy, which is often combined with medial facetectomy and foraminotomy, and has traditionally been the standard treatment. This technique involves stripping deep paraspinal muscles away from the spinous processes with retraction to expose the lamina. Concerns regarding the invasiveness of spinal procedures have been discussed previously. 4 –6 The long duration of retraction can result in multifidus atrophy and a disturbed arteriolar blood supply, which can cause postoperative chronic low back pain due to altered biomechanics of the posterior supporting ligamentous structures. 7
Lumbar spinal canal stenosis surgery has recently improved with the use of minimally invasive techniques. Less invasive procedures have emerged, and microendoscopic decompression through smaller incisions is frequently performed. Tubular surgery with the assistance of endoscopic surgery procedures has led to particularly remarkable changes in surgery, 8,9 with reduced tissue trauma and morbidity. Additionally, in spinal surgeries, minimally invasive modalities, including percutaneous and image-guided procedures, can be applied to treat several conditions. As a result of advances in surgical techniques and instruments, spinal microendoscopy has also been used to treat various diseases, such as lumbar spinal stenosis (LSS) and lumbar foraminal stenosis. 10,11
The microendoscopic technique is advantageous for decompression of lumbar stenosis because the lens of the endoscope is positioned at a 25° inclination, which provides superior visualization of lateral recesses and foramina compared with a surgical microscope. Because the camera is set inside the surgical field, it is possible to obtain an expanded visual field by positioning next to the target area. Blind areas are also eliminated compared with the visual field from outside the surgical field. This is thought to be useful in terms of safety, surgical progress, and education, because the entire surgical staff can share the same visual field.
First introduced by Foley and Smith in 1997, microendoscopic discectomy has been widely used for the treatment of lumbar disc herniation. 8 Minimally invasive laminectomy uses smaller incisions with the hope of reducing blood loss and pain, and shortening hospitalization compared with conventional open laminectomy procedures. In 2002, Palmer et al. also applied this technique for lumbar spinal canal stenosis. 9 Microendoscopic laminectomy (MEL) with surgical bilateral decompression (laminectomy) through a unilateral approach assisted by a tubular retractor and an endoscopic system was used for posterior decompression with a unilateral paramedian approach (Figure 1(a)). Microendoscopy provided wide visualization through oblique lenses and allowed bilateral decompression via a unilateral approach, through partial resection of the base of the spinous process, thereby preserving the supraspinous and interspinous ligaments and contralateral musculature. 12,13 Despite the increasing use of these minimally invasive techniques, few studies have directly compared the safety, efficacy, and outcomes of these procedures with conventional and microsurgical technique laminectomies. 14,15 The possibility of early postoperative ambulation is another advantage of endoscopic surgery. In elderly patients in particular, endoscopic laminectomy makes decompression possible with minimal invasion to the muscle and minimal bone resection, even in cases when fixation is difficult. Thus, it is thought to be a surgical technique that can be used for many spinal stenosis patients. However, there was concern that the use of the microendoscope required more surgical skills, 14,16 resulted in longer operative time, more intraoperative bleeding, more complications, and, thus, unfavorable outcomes.
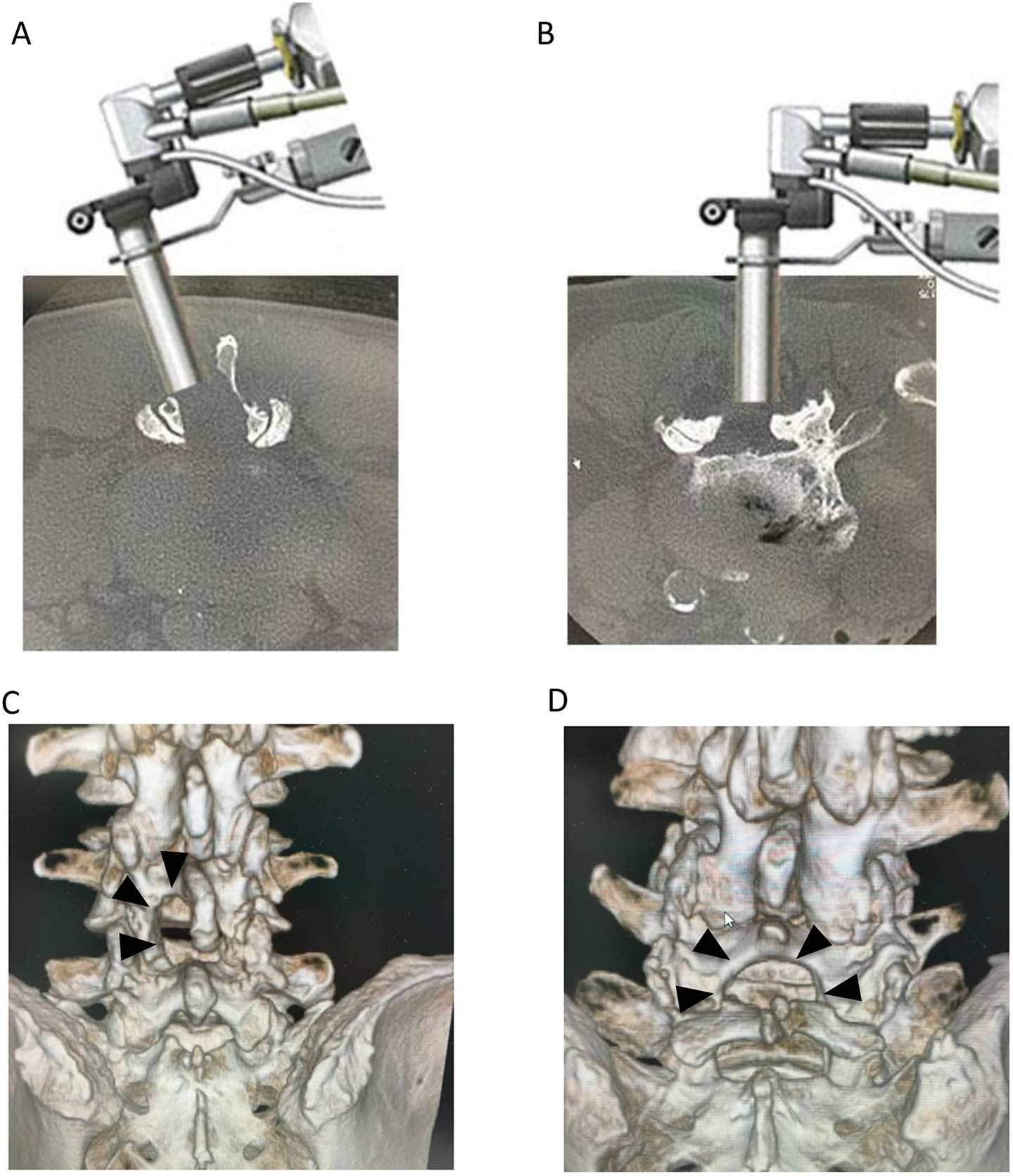
Details of the technique and postoperative 3D-CT image of the patients show decompression at L4-5 level.
As a less invasive procedure for patients and operators, in 2009, Hatta et al. reported a microscopic posterior decompression procedure, muscle-preserving interlaminar decompression (MILD). 17,18 In this technique, because decompression is performed through the midline approach, invasiveness to paravertebral muscles can be minimized, and the difficult problem of preservation of the facet joint in cases with narrow lamina is expected to be resolved. Moreover, Mikami et al., in their study, applied spinal microendoscopy to the MILD procedure (i.e. microendoscopy-assisted MILD (ME-MILD)) and reported the details of the procedure. 18 This technique allows decompression similar to that of MILD to be achieved with less invasiveness. The ME-MILD approach is a minimally invasive surgical procedure that involves endoscopically assisted tubular surgery via a midline approach that preserves the paravertebral muscles and bilateral facet joints (Figure 1(B)). We have also felt that, with MEL, the amount of joint resection on the entry side increases and that proficient surgical skills are needed for patients with insufficient decompression or a narrow vertebral arch on the contralateral side or pain in the upper portion of the lower back.
Thus, the purpose of this study was to evaluate the clinical outcomes at more than 3-year follow-up of two different minimally invasive decompressive surgical techniques that use spinal endoscopy (MEL and ME-MILD) for lumbar spinal canal stenosis at a single vertebral level (L4/5), based on a visual analog scale (VAS), the Japanese Orthopaedic Association (JOA) scoring system (maximum score 29 points) (Table 1), 19 and the JOA Back Pain Evaluation Questionnaire (JOABPEQ), which is an objective, patient-oriented test that scores health-related quality of life (HRQOL) for patients with low back disorders. 20
Criteria of the Japanese Orthopaedic Association’s Evaluation System for Lower Back Pain Syndrome (JOA score) system.
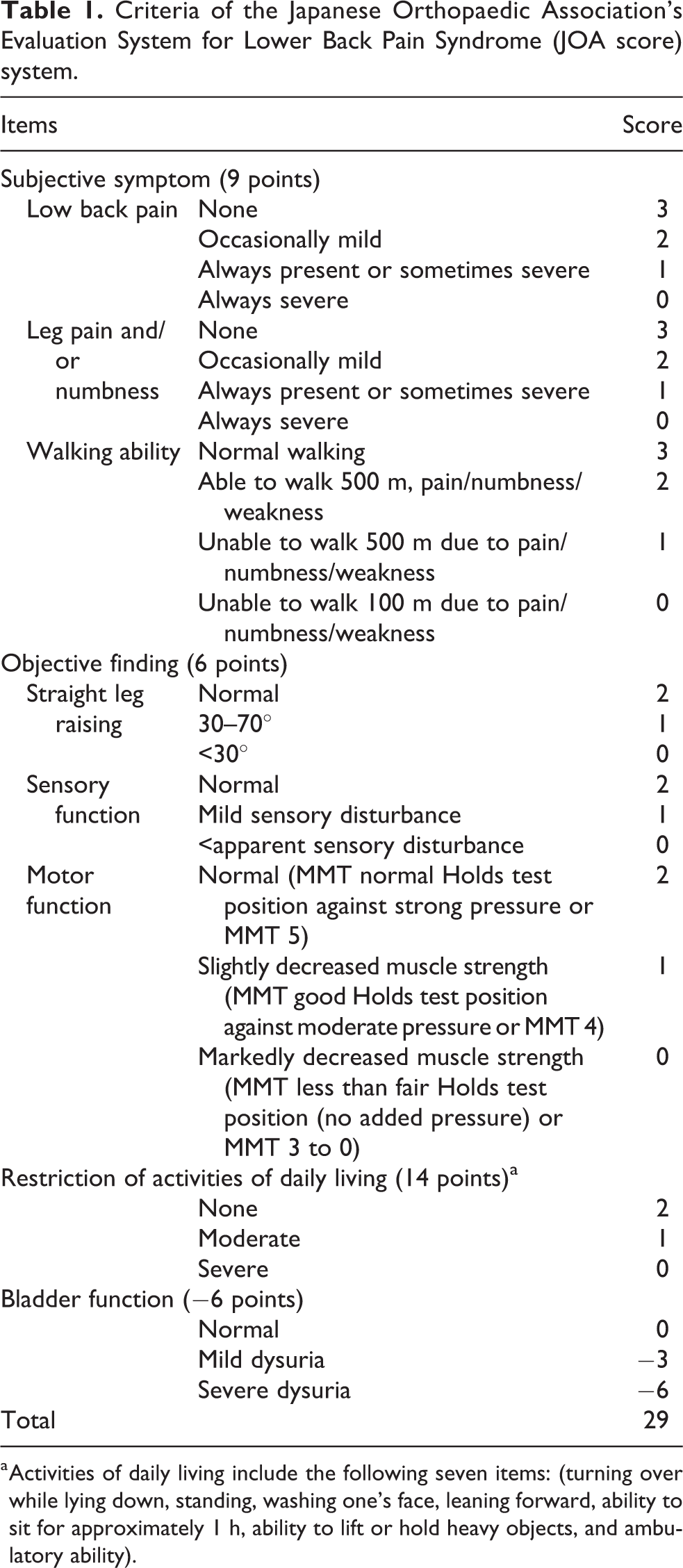
a Activities of daily living include the following seven items: (turning over while lying down, standing, washing one’s face, leaning forward, ability to sit for approximately 1 h, ability to lift or hold heavy objects, and ambulatory ability).
Patients and methods
This study was a retrospective review of prospectively collected surgical data. All the participants gave their written consent in accordance with the Helsinki Declaration, and written informed consent was obtained from the patient for publication and accompanying images. All procedures used in this research were approved by Japanese Red Cross Izu Hospital and Nakaizu Spring Rehabilitation Hospital. The study included 81 patients (MEL 39 patients, 20 men and 19 women; ME-MILD 42 patients, 22 men and 20 women) with LSS whose mean age was 68.9 years for MEL and 73.1 years for ME-MILD (Table 2). The indications for surgery were moderate-to-severe stenosis, persistent neurological symptoms, failure of conservative treatment over 3 months, and a JOA score under 15 points or intermittent claudication at 100 m. Moreover, this study investigated patients with LSS at a single (L4/5) vertebral level. Patients with mechanical back pain, more than grade 2 spondylolisthesis, or radiographic signs of instability, were not included. Clinical symptoms and signs of low back pain were evaluated prior to and following surgical intervention by a VAS, the JOA scoring system, and the JOABPEQ. These items were evaluated preoperatively and 3 years postoperatively. Postoperative care was standardized for all patients, who were allowed to sit up and walk without lumbar support on postoperative day (POD) 1. After the drainage tube was removed on POD 3, walking exercises and muscle training of the lower extremities were started.
Baseline Characteristics of the MEL Group Versus ME-MILD Group.
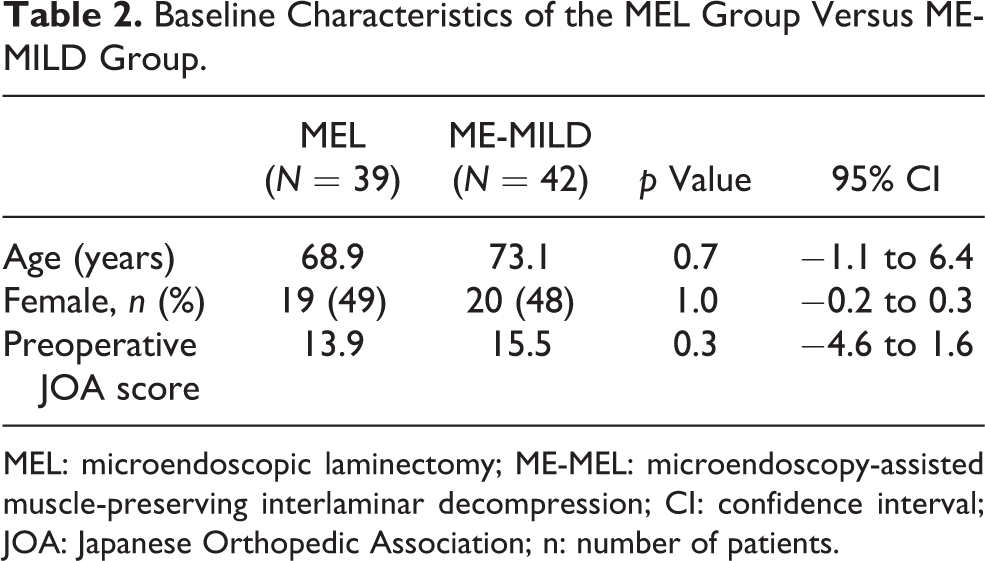
MEL: microendoscopic laminectomy; ME-MEL: microendoscopy-assisted muscle-preserving interlaminar decompression; CI: confidence interval; JOA: Japanese Orthopedic Association; n: number of patients.
The VAS scores included three VASs for current low back pain, buttock-leg pain, and leg numbness with a range of 0–10 (0 = no pain or numbness, 10 = worst pain imaginable or numbness). The JOA score was used to evaluate neurological status and clinical results. The authors examined the patients before surgery and 3 years after surgery to assess neurological findings and score the examination results. The JOABPEQ is a patient-oriented scoring of HRQOL for patients with low back disorders. From the answers to 25 questions, the examiner calculated five functional scores (low back pain, lumbar function, walking ability, social life function, and mental health). 20
Statistical analysis
Data were presented as mean and standard deviation (SD). We assumed that there were three outcomes, which were a VAS, JOA score, and JOABPEQ as essential measures for lumbar spinal canal stenosis, and compared the differences in the scores of each outcome with the unilateral group. For a priori power analysis, we decided the sample size of this study destination using G* power version 3.010 software. 21 Calculations using this software input data as mean and SD found that a minimum of 70 patients (35 patients each) were needed for the difference between the two group independent means in this study as a using significance level 0.05 and effect size 0.8. We thought that the number of samples in our study was sufficient to compare MEL and ME-MILD. Statistical analysis was performed using the Student’s t test, χ 2 test, and Fisher’s exact test. Values of p < 0.05 were considered significant.
Results
Low back pain was significantly improved in terms of the VAS score with MEL (p < 0.05) from 3 months, and there were significant differences with MEL (p < 0.001) and ME-MILD (p < 0.01) from 12 months compared with the preoperative baseline (Figure 2). Buttock-leg pain and numbness were significantly improved in terms of the VAS score from 3 months with both MEL (p < 0.001) and ME-MILD (p < 0.05).
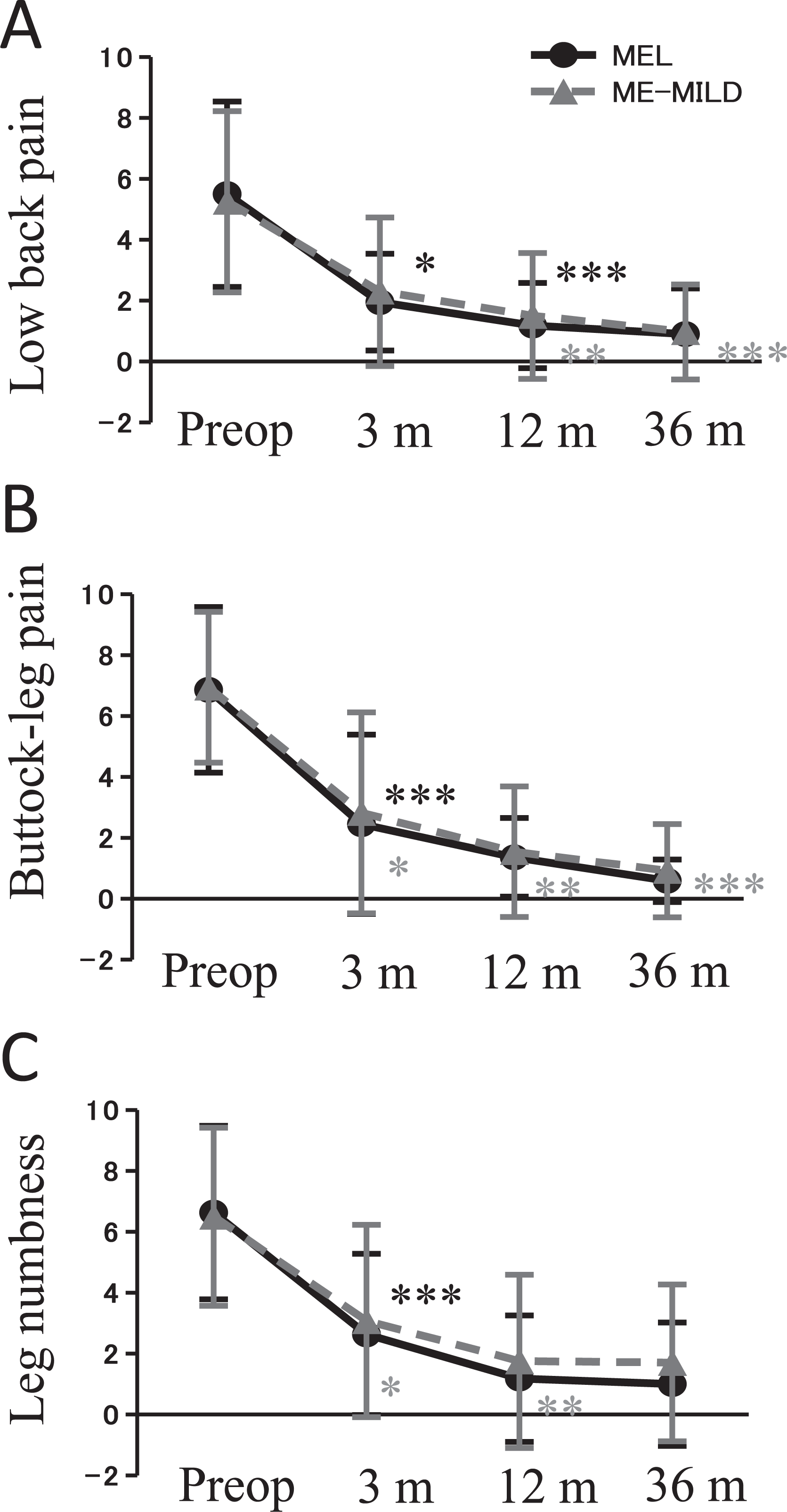
VAS scores for low back pain, buttock-leg pain, and leg numbness. VAS: visual analog scale.
The 3-year follow-up evaluation was completed for 76 patients. The JOA score improved from 13.9 to 25.5 with MEL and 15.5 to 26.4 with ME-MILD (Figure 3). The average recovery rate based on the JOA score was 76.4% with MEL and 83.2% with ME-MILD. All categories of JOA scores at the 3-year follow-up were significantly higher than those obtained before surgery (all p < 0.001) for both MEL and ME-MILD (Figure 4).
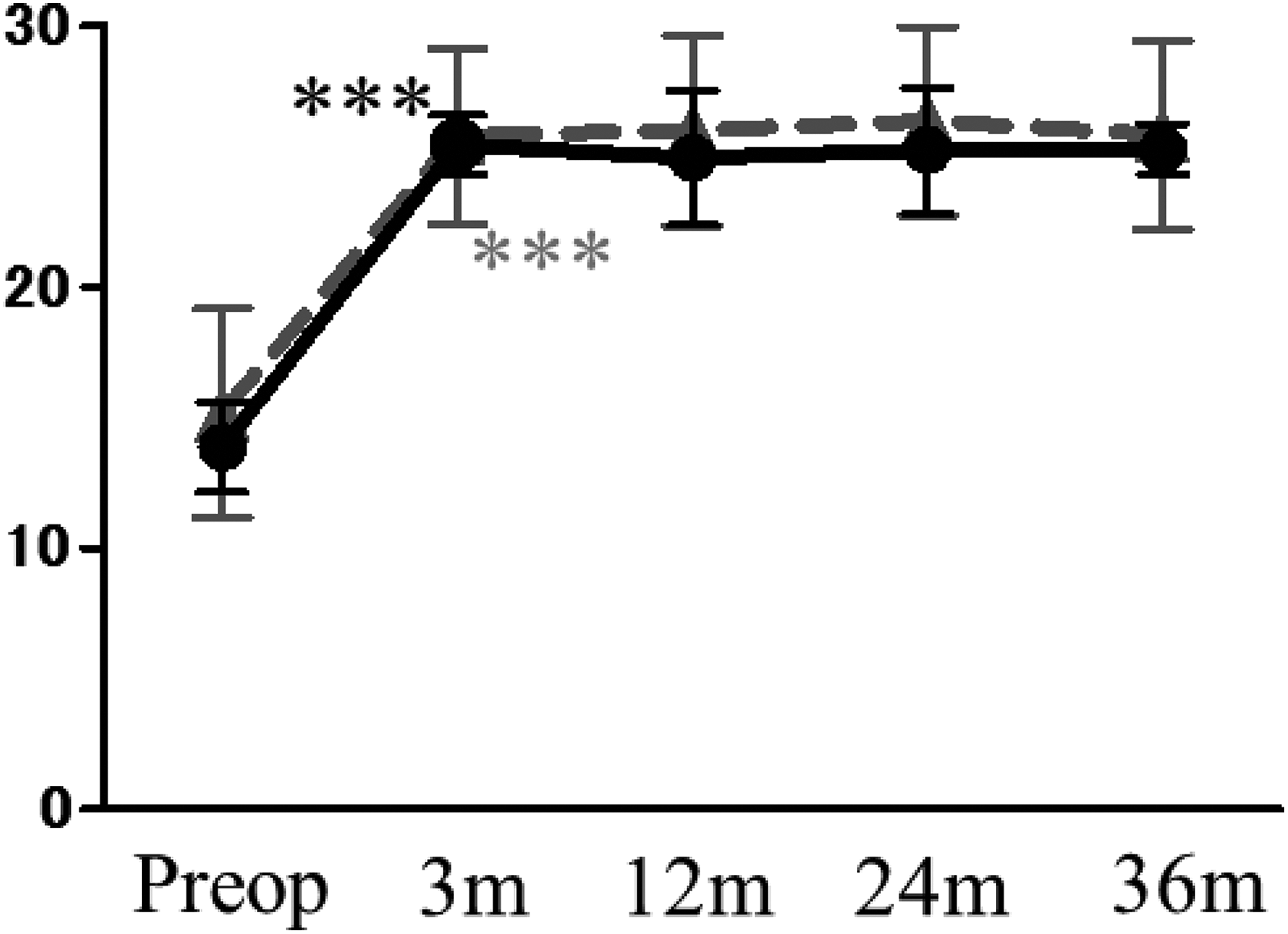
Japanese Orthopedic Association scores.
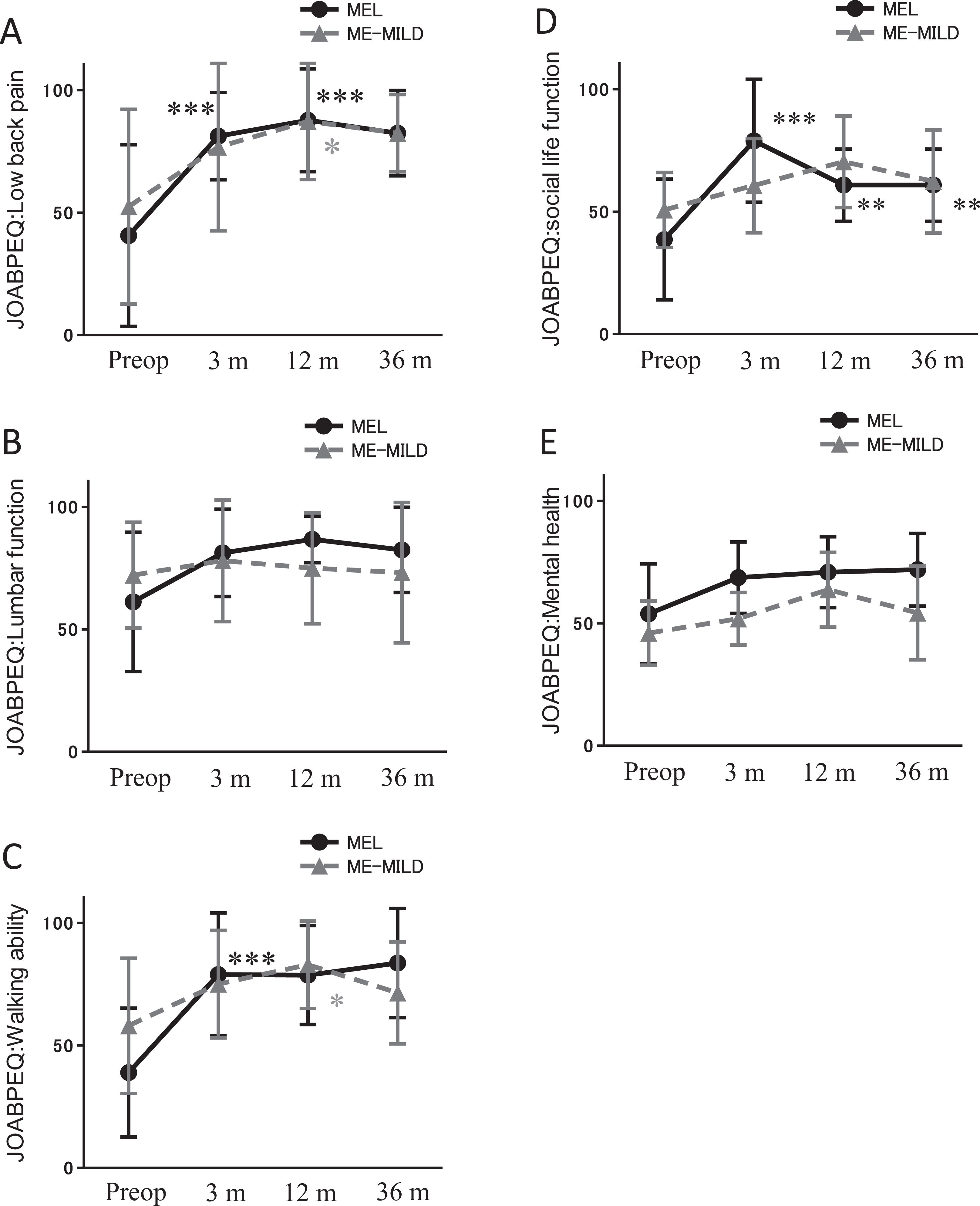
Japanese Orthopedic Association Back Pain Evaluation Questionnaire scores.
JOABPEQ Low back pain
Scores were significantly higher than the baseline preoperative score from 3 months to 36 months with MEL (p < 0.001). With ME-MILD, the scores increased at 3 months compared with preoperative score, but low back pain scores were significantly increased only at 12 months (p < 0.05).
Lumbar function
No significant differences were observed in lumbar function with both MEL and ME-MILD between preoperative period and each postoperative period.
Walking ability
Walking ability scores were significantly higher than the preoperative score from 3 months to 36 months with MEL (p < 0.001). With ME-MILD, the score was increased at 3 months compared with preoperative score, with a significant difference at 12 months (p < 0.05).
Social life function
Social life function scores were significantly higher than baseline preoperative scores from 3 months (p < 0.001) to 36 months (p < 0.01) with MEL. No significant differences were observed in lumbar function between preoperative period and each postoperative period with ME-MILD.
Mental health
No significant differences were observed in mental health with both MEL and ME-MILD between preoperative period and each postoperative period.
Complications included a dural tear in one patient in each group and infection in four ME-MILD patients (9.5% p = 0.06). There was no postoperative instability at the operated segment as evaluated with dynamic radiographs at the final follow-up.
Discussion
The microendoscopic decompression technique for lumbar disorders is a well-established method for the treatment of LSS; however, there is a concern that tubular surgery with the assistance of endoscopic decompression requires a skilled spine surgeon. The microendoscopic decompression technique for bilateral decompression surgery generally uses a unilateral approach. However, in cases where the lamina is narrow, it may sometimes be difficult to preserve the facet joint on the approach side, and limited working space may make it difficult to exfoliate nerves and achieve good anatomical orientation. 14 With MEL using a unilateral approach, there is more facet joint resection on the entry side. This is a cause of instability and makes insufficient decompression more likely to occur on the contralateral side. On the other hand, the ME-MILD approach involves tubular surgery with the assistance of endoscopic surgery via a midline approach; it is a minimally invasive surgical procedure with favorable results that enables preservation of paravertebral muscles and bilateral facet joints, and it provides an ample and symmetrical surgical field that is similar to conventional open procedures. 22 However, there have been no reports comparing surgical invasiveness between MEL and ME-MILD. Therefore, this study aimed to evaluate the effectiveness of MEL and ME-MILD based on clinical outcome scoring systems: a VAS, the JOA score, and the JOABPEQ. The results indicated that MEL and ME-MILD for lumbar decompression are less destructive to the paraspinous muscles and may have better clinical outcomes. In addition, the results demonstrated that ME-MILD is a safe and very effective minimally invasive technique for degenerative LSS, similar to MEL. Low back pain in terms of the VAS score and walking ability were significantly improved compared with preoperative period by both MEL and ME-MILD.
The patients of this study were diagnosed with LSS, and the indications for surgery were moderate-to-severe stenosis, persistent neurological symptoms, and failure of conservative treatment over 3 months with a JOA score under 15 points or intermittent claudication at 100 m. Moreover, this study investigated patients with a single vertebral level (L4/5) of LSS. Previous studies indicated that MEL is a safe and effective surgical alternative to classic laminectomy and laminotomy procedures, because it is possible to attain complete decompression with minimal invasion of the surrounding tissue. 12,13,14,16 On the other hand, ME-MILD is a minimally invasive procedure for LSS with which favorable clinical results can be expected. 22
In the present study, low back pain was significantly improved in terms of the VAS score with MEL from 3 months, and there were significant differences with ME-MILD from 12 months compared with preoperative period. Buttock-leg pain and numbness were significantly improved in terms of the VAS score from 3 months with both MEL and ME-MILD. At all periods during the 3 years of follow-up, the JOA scores of both MEL and ME-MILD were significantly higher than those obtained before surgery. Thus, there were no differences in improvement of the VAS and JOA scores between MEL and ME-MILD. However, evaluating the clinical outcomes with patient-oriented scoring systems indicated that MEL tended to be superior to ME-MILD.
Because there were improvements of low back pain and walking function, it appears that low back pain, activities of daily living (ADL), and neurological status were improved by microendoscopic decompression surgery.
In contrast, there were no significant differences in lumbar function and mental health on the JOABPEQ with both MEL and ME-MILD between preoperative period and each postoperative period. Therefore, there was no improvement in patient satisfaction with lumbar function and mental health. Lumbar function may already have a higher score at the preoperative period, so that the improvement rate may be small in the postoperative period. On the other hand, a previous study showed that all categories of the JOABPEQ scores were significantly higher after surgery than before surgery with 2 years of follow-up. 12
Complications included a dural tear in one patient in each group and infection in four ME-MILD patients (9.5%; p = 0.06). There were no serious complications, there was no difference in the presence of dural tear in both groups, and it did not lead to worsening of neurological symptoms. We believed that the cause of wound infection might be due to the use of electrocautery unit that we used for tissue cauterization; skin necrosis occurred only at the time of ME-MILD, and these surgical sites were small. However, these patients who had infections were superficial surgical site infections, did not require resurgery and healed immediately by washing and antibiotic administration. In addition, confirmation of wound margin carefully when closing wound, and if further injured, surgical margin resection was added during surgery, thereafter no surgical site infection occurred.
There are several limitations to this study, the most significant being the lack of a control group, and it is important to study patients undergoing tubular surgery with the assistance of endoscopic surgery and compare the outcomes with those of conventional open surgeries. Moreover, LSS decompression surgery may improve lumbar pain and walking ability more than lumbar function and mental health. Based on these results, it will be necessary to investigate patient history and current status of mental health.
To deal with the more diverse medical histories, complications, and anatomical deformations of patients as they age, it is important to learn a variety of operative procedures. Use of MEL, ME-MILD, or other spinal endoscopic procedures depending on the patient and the circumstances makes it possible to deal with advanced bony deformities or stenosis that is thought to present a high level of difficulty, and it will lead to the future spread and evolution of spinal endoscopic surgeries.
Conclusions
With MEL and ME-MILD, all categories of VAS scores and JOA scores over 3 years of follow-up were significantly higher than those obtained before surgery, and there were improvements of low back pain and walking function in JOABPEQ. Therefore, it appears that low back pain, ADL, and neurological status were improved by microendoscopic decompression with both MEL and ME-MILD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.