
Abstract
Purpose:
The objective of this study was to assess the outcome of patients treated with magnetically controlled growing rods (MCGRs) using a standardized distraction procedure with intended distraction-to-stall and to compare the outcomes between idiopathic and nonidiopathic patients.
Methods:
This was a retrospective single-center cohort study. Conversion cases were excluded. Distractions were performed with 2- to 3-month intervals with the intention of distraction-to-stall on both rods. Distraction length was measured on X-rays every 6 months. Spinal height was assessed using T1-T12 and T1-S1 annual increase.
Results:
19 patients (eight idiopathic and 11 nonidiopathic) were included. Mean age at surgery was 9.7 ± 1.9 years, and median follow-up was 1.9 years (interquartile range (IQR): 1.3–2.2). Major curve improved from median 76° (IQR: 64–83) preoperatively to 42° (IQR: 32–51) postoperatively (p < 0.001) corresponding to a curve correction of 43% (IQR: 33–51). Correction was maintained at 1- and 2-year follow-up. Median annual T1-T12 and T1-S1 height increase were 10 mm (IQR: 6–16) and 11 mm (IQR: 7–33), respectively. A total of 159 distraction procedures were performed; 83.5% of these were distracted-to-stall, and 16.5% were stopped due to discomfort. Median rod distraction per procedure was 2.0 mm (IQR: 1.6–2.7) for the concave side and 1.7 mm (IQR: 1.4–2.5) for the convex side. Five patients had implant-related complications. Patients with nonidiopathic etiology were significantly younger and had lower flexibility compared with idiopathic patients (p ≤ 0.040). However, we found no statistically significant difference in curve correction, spinal height increase, distraction length, or complications between the two groups (p ≥ 0.109).
Conclusion:
MCGR effectively corrected the deformity and increased spinal height using a distraction procedure with intended distraction-to-stall. Five of 19 patients had implant-related complications, and we found no difference in the outcomes between idiopathic and nonidiopathic patients.
Keywords
Introduction
Magnetically controlled growing rod (MCGR) surgery is a recently developed technique for treating early-onset scoliosis (EOS). EOS is defined as scoliosis diagnosed before the age of ten, 1 and if left untreated, EOS is associated with increased mortality. 2 The patients often have a substantial remaining skeletal and pulmonary growth potential, and therefore, the main goal of treatment is to halt curve progression while allowing spinal growth to preserve pulmonary function. 3 Bracing and casting are first choices as they allow continuous growth of the spine and can delay final surgery. 4 However, in patients with curve progression, despite bracing, surgery may be indicated. 3 Because early thoracic fusion can lead to a restrictive decreased lung function, 5,6 different growth-friendly surgical techniques have been developed. 7 Traditional growing rods are a distraction-based technique that corrects the deformity and prevents curve progression, 8 but it requires repetitive surgical procedures leading to high complication rates. 9 To avoid repeated surgical procedures, the MCGR system was developed allowing lengthening with an external remote control (ERC). 10 –12 Preliminary results are promising as the MCGR procedure corrects the deformity while allowing continuous growth of the spine. However, despite reducing the number of surgical procedures compared with traditional growing rods, 13,14 the rate of implant-related complications remains high. 13 –16
Consensus is lacking regarding distraction frequency, amount, and technique. 17 Different distraction protocols have been described where the desired distraction length is based on estimated growth (“tail-gating”) or a set distraction amount and monitored with X-ray or ultrasound measurements. 16,18 –22 No studies so far have described the use of a distraction procedure with intended distraction-to-stall (distraction to “clunking”) and not relying on a set distraction amount or estimated growth.
The primary purpose of this study was to assess curve correction and complications in patients operated with MCGR and to evaluate the efficacy of a standardized distraction procedure. The secondary purpose was to compare the outcomes for idiopathic patients with that of nonidiopathic patients.
Materials and methods
We conducted a retrospective study on all patients surgically treated with MCGRs at a single institution. Patients were prospectively registered from November 2013 through August 2017. Exclusion criteria were single-rod constructs or conversion cases with former growth instrumentation. Age at diagnosis was registered, and etiology was recorded according to the Classification of Early-Onset Scoliosis (C-EOS). 1 A total of 21 patients were treated with MCGR in the study period. Two were excluded from the study as they were converted from former growth instrumentation. Mean age at index surgery was 9.7 years (SD: 1.9, range: 6.2–12.7), and median follow-up was 1.9 years (inter quartile range (IQR): 1.3–2.2, range: 0.3–3.6); 17 patients had minimum 1-year radiological follow-up. The study was approved by the local health authorities and data protection agency (journal no.: 2012-58-0004).
Surgical procedure
All patients underwent surgery with two attending spine surgeons through a posterior-only approach according to the technique described by Akbarnia et al. 10 Initially, the patients received two standard rods. Later in the study period, we used one standard rod on the concave side of the major curve and one offset rod on the convex side. Primary intended fixation method for proximal and distal anchor sites was pedicle screws; this could be changed at the discretion of the treating surgeon in case of poorly developed pedicles or similar. Likewise, the use of cross-links was at the discretion of the treating surgeon. Facetectomies were performed on the fixation levels, and local bone tissue mixed with bone substitute was used for fusion. In the majority of procedures, the rods were passed intramuscularly in the craniocaudal direction to avoid surgical exposure between the cranial and caudal fixation levels. The distraction ability of the rods was manually tested before insertion and after any contouring of the rods. We intended to achieve maximal correction with primary surgery respecting overall balance; hence, maximal distraction was applied on both rods intraoperatively. Postoperative bracing was used in selected cases at the discretion of the surgeon.
Distraction procedures
Distractions were mainly performed in an outpatient clinic setting with the patient in a prone position or lying on the side and without the need for pain killers or sedation. All distractions were performed by one of two experienced spine surgeons in a standardized approach with the intention of distracting-to-stall, also referred to as “clunking” or rod slippage. The two actuators were identified with a magnet, and distractions were performed on each rod separately, starting on the concave side of the major curve. If further distraction on the concavity could be achieved, a second lengthening on the concavity was attempted as a third step. The procedure was interrupted before clunking if the patient expressed discomfort or showed signs of such. Distractions were categorized as not specified if information of distraction stop was insufficient. First distraction was performed 3 months after the index surgery. Distractions were generally performed with 2- to 3-month intervals and achieved lengthening monitored with full-spine X-rays every half a year. For patients with congenital/structural etiology, a shorter distraction interval was preferred in the beginning of the treatment. Distraction interval was recorded as number of days since last intervention, either surgery or distraction.
Radiological assessment
Radiographs were obtained in the international Digital Imaging and Communications in Medicine format and uploaded to the validated online imaging system KEOPS (SMAIO, Lyon, France) 23 where radiographic measurements were performed. Radiographs were taken in the most upright position preoperatively and postoperatively; at 3, 6, and 12 months postoperatively, and onward every 6 months. On coronal radiographs, the following variables were recorded: major curve and secondary curve angle (defined as the largest secondary curve >20°), supine lateral bending major curve, coronal balance (the horizontal distance from the C7 plumb line to the central sacral vertical line), and upper and lower instrumented level. A preoperative annual progression rate (APR) was calculated according to the C-EOS. 1 On sagittal radiographs, kyphosis was recorded as the maximum Cobb angle between any two vertebrae in consistency with the C-EOS. Lordosis was recorded as the underlying Cobb angle to S1. From coronal measures, the following were calculated and expressed in percentages as described in former studies 24,25 :



Thoracic (T1-T12) and total spine (T1-S1) heights were measured preoperatively and postoperatively and at the latest radiological follow-up prior to final fusion surgery in accordance with former studies 13 (Figure 1). Annual T1-T12 and T1-S1 height gain were calculated together with T1-T12 and T1-S1 height gain per distraction procedure. All images were calibrated with the known rod diameter ensuring consistency in the measurement and comparison of multiple radiographs. Rod distractions were assessed on radiographs and measured on each rod separately not taking into account the distraction performed intraoperatively (Figure 1). A yearly distraction and a per-procedure distraction length were calculated.

A case showing an 8-year old boy with Cri-du-chat syndrome. Progression despite Boston bracing. Major curve improved from 75° preoperative to 32° postoperative and was 37° at 2-year follow-up. Kyphosis was 22°, 14°, and 16°, respectively. T1-T12 and T1-S1 annual growth values were 14 and 22 mm/year, respectively.
Statistics
Statistical analyses were performed using R, version 3.2.5. Distributions were assessed with histograms and quantile–quantile plots. Data are presented as proportions (%), means with standard deviation (SD) or medians with range or IQR. Repeated measures of slot length are presented in Spaghetti plots and radiographic outcomes in boxplots. Categorical data were compared using Fisher’s exact test and continuous data with two-tailed Student’s t-test or Wilcoxon’s test.
Results
Median preoperative APR was 14.4° (IQR: 7.4–18.9), and median flexibility was 37.0% (IQR: 24.4–51.4). Major curve and secondary curve were reduced from 76° (IQR: 64–83) and 44° (IQR: 37–52) preoperative to 42° (IQR: 32–51) and 32° (IQR: 22–40) postoperative, respectively (p < 0.001). This corresponded to a median major curve correction of 43% (IQR: 33–51) and a median CCI of 108% (IQR: 91–117). Correction was maintained throughout the distraction period. Compared with preoperative values, median major curve was 45° (IQR: 34–55) at 3-month, 45° (IQR: 38–53) at 1-year, and 52° (IQR: 41–54) at 2-year follow-ups (p < 0.001). Likewise, secondary curve was 36° (IQR: 28–44) at 3-month, 34° (IQR: 29–44) at 1-year, and 36° (IQR: 29–43) at 2-year follow-ups (p < 0.006; Figure 2). Kyphosis was significantly reduced from 42° (IQR: 30–55) preoperative to 32° (IQR: 23–40) postoperative (p < 0.001); however, we found no statistically significant difference compared with preoperative values at 3-month (median: 38°, IQR: 27–44), 1-year (median: 38°, IQR: 24–50), or 2-year (median: 37°, IQR: 26–49) follow-ups (p > 0.168; Figure 2). No difference was found regarding coronal balance (p > 0.441; Figure 2).

Boxplot of major curve angle, overall kyphosis, secondary curve, and lordosis. 17 patients were available for 1-year follow-up and 11 patients for 2-year follow-up.
Five patients had implant-related complications (three screw loosening, one rod breakage, and one iliac hook fixation failure). This led to four unplanned reoperations as one patient with screw loosening and proximal junctional kyphosis (PJK) was handled conservatively (Figure 3). Additionally, one patient underwent unplanned surgery due to distal adding on and pelvic obliquity, and further, one patient had a revision surgery as full distraction was reached after 23 months. Mean T1-T12 and T1-S1 height increased from 186 mm (SD: 31) and 301 mm (SD: 46) preoperatively to 207 mm (SD: 28) and 339 mm (SD: 43) postoperatively, respectively.

A case showing a 9-year old boy with neurofibromatosis type 1. Progression despite Boston bracing. Preoperative major curve of 72° was reduced to 42° postoperatively. At 1-year follow-up, a CT scan showed proximal screw loosening on the right rod, but symptoms disappeared, and distractions were continued until full distraction at 20-month follow-up. After replacement of the rods, the patient developed proximal junctional kyphosis and hook displacement, and final fusion was performed 3 years after initial implantation. CT: computed tomography.
A total of 159 distractions were performed during the study period; 83.5% were distracted to stall (Table 1). We saw only positive gains in distraction length indicating no cases with loss of distraction (Figure 4). Two distractions were performed in short general anesthesia. One distraction led to persistent pain in a patient where the actuator was reversed in an additional procedure.
Distraction procedures.
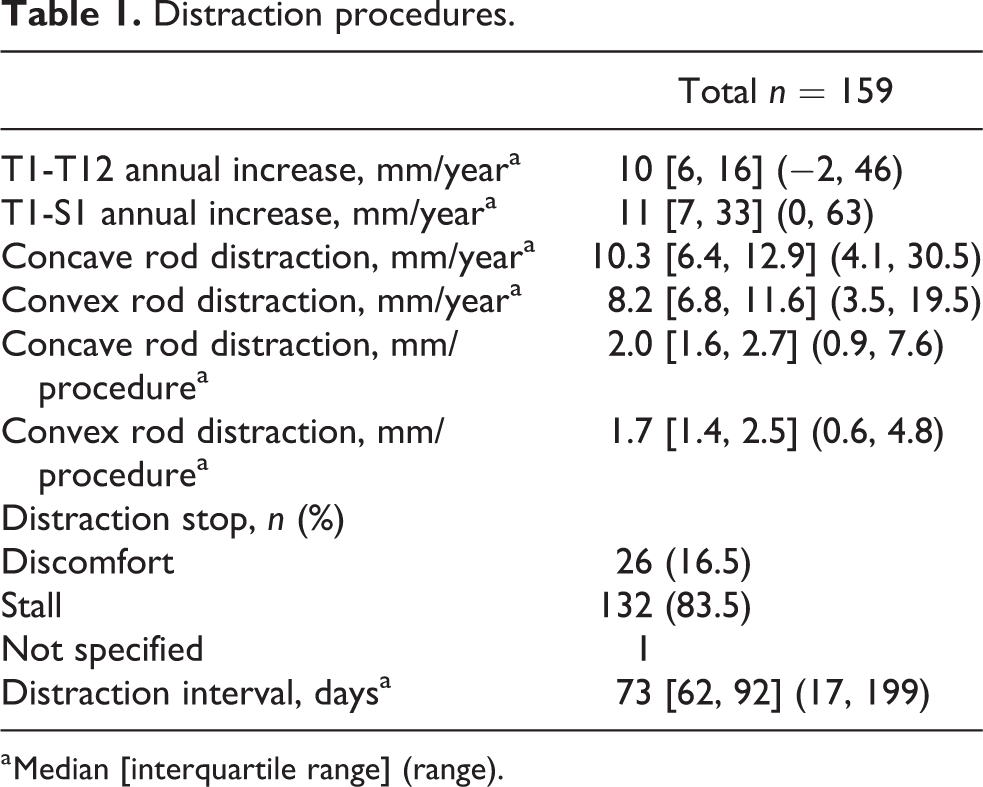
a Median [interquartile range] (range).

Spaghetti plots showing distraction length throughout the distraction period on the concave and convex rod, respectively.
Eight patients were characterized as idiopathic according to the C-EOS (Table 2). Patients with nonidiopathic etiology were significantly younger and had lower flexibility compared with idiopathic patients (p ≤ 0.040). We found no statistically significant difference in CCI, spinal height increase, distraction length, or complications between the two groups (p ≥ 0.109; Table 3).
Demographics.

ASA: American Society of Anesthesiologists.
a Mean (standard deviation).
b Totals exceed 100% as some patients had more than one indication.
Idiopathic vs. nonidiopathic etiology.
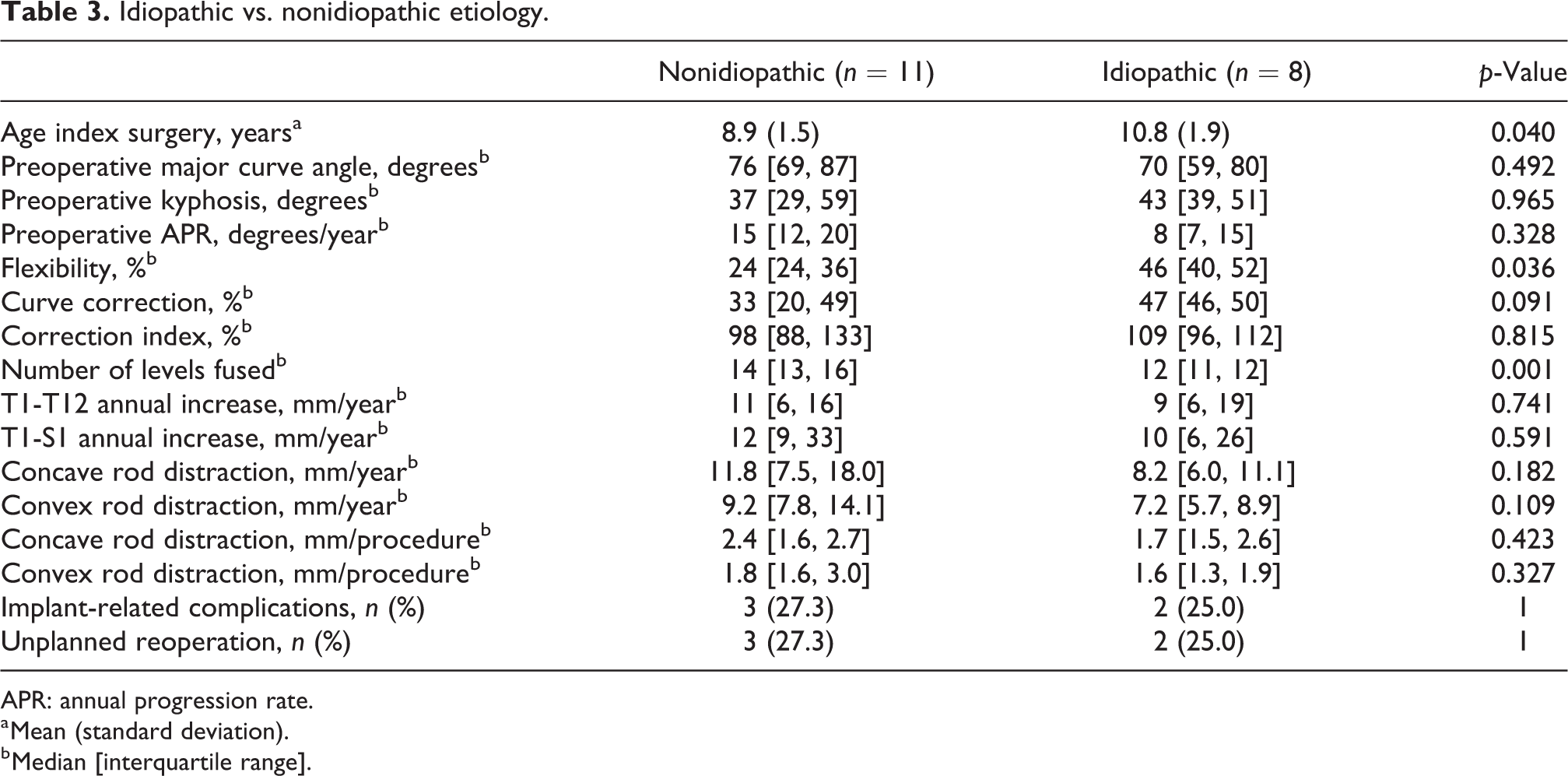
APR: annual progression rate.
a Mean (standard deviation).
b Median [interquartile range].
Discussion
In a single-center cohort of mainly EOS patients, we demonstrate the efficacy of MCGR to correct deformity and maintain curve correction through the distraction period. A standardized distraction procedure with intended distraction-to-stall ensured spinal growth throughout treatment without increasing the complication rate compared with results reported in the literature. We found no difference in radiographic or clinical outcomes between patients with idiopathic and nonidiopathic deformities.
The overall goal of surgical treatment is to preserve lung function by allowing continuous growth of the spine and secondarily to reduce pain and improve quality of life for these children. As such, the timing of surgery relies on two main indicators: a severe curve or curve progression despite bracing and an estimated substantial remaining growth potential. Various inclusion criteria are listed in previous studies of MCGRs. 10,11,14 –16,18,20,26 –29 Age at index surgery and etiology in our study did not differ considerably from these. Some studies have indicated that single-rod MCGR constructs and conversion from former growth instrumentation are associated with higher complication rates, poorer curve correction, and less spinal growth. 10,18,22,26,29 For these reasons, we excluded these patients from our study.
Median curve correction in our study was comparable to other studies (range: 34–57%). 10,15,16,20,24,26,28,30 The surgical technique is inconsistently reported in these studies, and whether to perform maximal intraoperative distraction and curve correction is unknown. The concern is increased rod loading and the risk of early distraction failure or complications. 17 However, we performed maximal intraoperative distraction and experienced no distraction failures throughout the distraction period. Secondary curve was also reduced postoperatively, and so far, this is the first study to report results on the secondary curve with MCGRs.
Several studies show a tendency similar to our study with a reduction of kyphosis after surgery and a small increase during the distraction period. 10,11,18,24,28,29 Akbarnia et al. hypothesized that increased overall kyphosis at follow-up was a result of increasing kyphosis outside the instrumented levels. 10 Rod contouring is limited around the actuator portion of the MCGR. Consequently, surgery results in a relative hypokyphosis at the instrumented levels, which leads to a compensatory kyphosis on top of the instrumentation. It may lead to PJK and associated proximal implant fixation failure. 29 This was probably the case for one patient in our study with a high thoracic major curve who underwent revision and subsequently final fusion addressing this issue (Figure 3). Two patients with distal screw loosening were more likely to be caused by suboptimal screw positioning at implantation. The rod fracture occurred in a patient with congenital fusion anomalies and hyperlordosis weighing 17 kilograms at implantation with 4.5-mm rods so no conclusions can be drawn from this. Overall, the rate of implant-related complications and unplanned surgery in our cohort was comparable to other studies 14,16,18,20,26,28 and with no deep infections.
Based on the results reported by Dimeglio et al., the normal spine growth has been established. The T1-T12 height increases with 0.7 cm/year from 5 to 10 years of age and 1.1 cm/year during puberty. T1-S1 height increases with 1 cm/year from 5 to 10 years of age and 1.8 cm/year between 10 years of age and skeletal maturity. 31 Compared with this, T1-T12 and T1-S1 annual increases in our study were satisfying, however, with a wide range. Other studies using a distraction protocol relying on expected growth and ERC measurements report T1-T12 and T1-S1 height increase rates of 3.6–9.6 and 6.3–10.6 mm/year, respectively. 15,27 –29 Only one patient in our cohort had no increase in spinal height despite rod distractions were successful (T1-T12 was −2 mm/year), most likely due to PJK (Figure 3). This case underlines that sagittal deformity needs to be taken into consideration when assessing spinal height on an anterior–posterior radiographs.
Different distraction protocols have been suggested using either ultrasound or radiographs to measure the achieved distraction length. 10,17 Ultrasound was introduced to reduce the amount of radiation exposure from repeated radiography and shows excellent correlation with distraction length measured on radiographs. 19 However, ultrasound has a learning curve and is only able to measure the achieved distraction length. Radiographs are still performed every 6 months to monitor curve correction and implant-related complications. 17,24 Distraction protocols described so far have relied on Dimeglio’s data on normal spine growth 31 and the surgeons’ estimate of the desired distraction. 10,11,15,16,18,20,24,27 –29 Recent studies by Lebon et al., 16 Cheung et al., 24 and Ahmad et al. 32 all showed that the achieved distraction length was less than that expected from the amount read on the ERC. Only one study by Hickey et al. including eight patients (four single rods and four double rods) described distraction performed “as much as the ERC would allow” within the first 6 postoperative weeks. 30 Our study is the first to describe in detail a distraction procedure relying on distraction-to-stall or “clunking” and not on estimated growth rate and ERC measurements. We performed a total of 159 distraction procedures, and 83.5% were distracted-to-stall. If the patient felt any pain or discomfort, distraction was stopped before (16.5%). In some distractions, “clunking” occurred early. Generally, we did not change the distraction interval due to early “clunking,” and patients were seen at the next regular distraction. However, if early “clunking” continues in repeated distractions, increasing the distraction interval could be a solution. Also, it needs to be considered together with standing height, menarche, or other growth assessments if maximal spinal growth is achieved and the patient is ready for final surgery. This was in fact the case for one patient in our study who was 1.5 years postmenarche and Risser grade 4 by the end of the study period and planned for final fusion after three consecutive distractions with early “clunking” and unchanged standing height. Future studies of MCGR graduates will have to look into this issue.
The discrepancy between the ERC measurement and the achieved distraction length is influenced by several factors. “Cross-talking” can be a problem if rods are placed too close to each other, which might have been an issue in the six patients in our study who had two standard rods implanted at primary surgery. We now use one standard rod and one offset rod as standard construction. Distance from the skin to the actuator and resistance in the tissue can also affect the achieved distraction length. 17,33 We found no loss of distraction, and only one distraction led to persistent pain where the actuator had to be reversed in an additional procedure. The two distractions performed under general anesthesia were not related to “clunking,” and subsequent distractions in these two patients were uncomplicated and performed as earlier described.
Overall, there seems to be different distraction procedures with comparable results in terms of successful distractions (“tail-gating,” “set distraction amount,” and “distraction-to-stall”). 21,24,29,32 For comparison with other studies, we presented an annual spinal height increase; however, there are issues influencing on this measure such as PJK 10,29 and decreased lengthening of the MCGR over time. 32 Whether this decreased lengthening is related to stiffness and autofusion of the spine (the law of diminishing returns), 16,32 the construct of the MCGR 24 or a result of skeletal maturity still needs to be examined in future studies. These issues also apply to our distraction method. Distraction-to-stall can generally be done without causing pain to the patients. The patients simply tell if they feel discomfort, and distraction is stopped or the patient is repositioned. However, one must not blindly trust “clunking,” but take into account the amount read on the ERC as there is a risk of causing pain. This might have been the case in the patient experiencing pain after a distraction although the achieved distraction length after the procedure leading to pain was only 3.6 mm. The rods were distracted to clunking at the next regular interval without any complications or pain. We do not find it necessary to take full-spine radiographs more frequently than every half a year to monitor curve control, complications, and achieved distraction length, thereby reducing unnecessary radiation to these children. However, radiographs are still needed in case of a patient presenting with pain, suspected complications, or repeated early clunking before further distraction is performed.
Few studies have compared the outcomes between patients with different etiologies. 16,20 They show no difference between etiologies, but the number of patients in each category is low. We found that nonidiopathic patients had lower flexibility and a tendency toward a lower curve correction. Correspondingly, CCIs were similar in idiopathic and nonidiopathic patients, indicating that flexibility can predict the correction achieved at primary MCGR implantation. 24 There was a tendency toward a larger spinal growth and distraction length in nonidiopathic patients, which can be explained by the relative number of extra instrumented levels compared with idiopathic patients. Still, numbers in each group are increasing the risk of a type 2 error. Future large multicenter studies will have to address if equally good results can be achieved across all etiologies.
Although this was a retrospective study, we are confident in the validity of the data since patients and distraction procedures were prospectively registered. It would have been preferable to compare different distraction protocols; however, the heterogeneity and small number of patients treated with MCGR make it difficult. This is one of the largest single-center cohort studies describing a homogenous EOS population without confounding factors such as single-rod constructs or conversion cases. It is the first study to report the efficacy of a distraction-to-stall procedure, which may aid surgeons in their clinical practice as it is simple, reproducible, and efficient in increasing spinal height in EOS patients.
Conclusion
We found that MCGR effectively corrected major and secondary curve, and correction was maintained throughout the distraction period. Using a standardized distraction procedure with intended distraction-to-stall on each rod separately resulted in satisfactory spinal height increase. Implant-related complications were comparable to the available literature, and we found no difference in the outcomes between idiopathic and nonidiopathic patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Institutional grants were received outside the submitted work from K2M and Medtronic.
Study approval
The study was approved by the Danish Patient Safety Authority and the Danish Data Protection Agency (journal no.: 2012-58-0004).