
Abstract
Despite suggestions that tourniquet inflation during total knee replacement reduces bleeding and hence improves cement penetration, no studies exist supporting this widely held belief. In this single-blinded, single-surgeon, randomized controlled trial, the tourniquet inflation during cementation group (n = 20) did not have greater tibial cement penetration compared to a no tourniquet group (n = 20). No statistically significant differences in semiautomatic digitally measured average and central radiographic tibial plateau penetration values were observed between the two groups (p = 0.93; p = 0.84). Tourniquet inflation during cementation does not appear to improve tibial cementation penetration.
Introduction
Tourniquet use during total knee replacement (TKR) remains controversial with potential advantages and disadvantages. 1 –3 One potential disadvantage of not using a tourniquet in cemented TKR is reduced bone cement or polymethylmethacrylate (PMMA) penetration, due to increased cancellous bone bleeding or clot debris during cementing. As bone cement has no adhesive properties, adequate penetration is important to achieve component stability by mechanical interlock with bony trabecular spaces. 4 –8 It has been suggested that the main advantage of a tourniquet is the superior cementation that a blood-free field provides 2,3,9 ; however, the literature investigating this potential advantage of tourniquet use has been sparse till date.
There is a lack of clinical data of tourniquet’s effect on cement penetration, with most prior studies focusing on bleeding during total hip cementing. Earlier simulated laboratory, 10,11 in vitro 12 and in vivo 13 animal studies reported that intraoperative bleeding and intramedullary bleeding pressure during cement penetration may compromise the shear strength of bone–cement interface.
A bovine total hip replacement (THR) model investigation by Majkowski et al. 12 suggested that bleeding did not exert a negative influence on the depth of cement penetration; however other studies 10 have suggested that blood has a negative effect on cementation undertaken at low pressures in THR models. To date, the clinical utility of tourniquet use in knee arthroplasty cement penetration remains uncertain. 3
Adequate cement penetration provides adequate implant stability; 4 –8 however, wide variations in cementing techniques among surgeons can affect the final penetration and its related sequelae, such as implant stability, migration, and aseptic loosening. 5,14 Aseptic loosening has been described as having a multifactorial etiology, including stress shielding, micromotion, high joint fluid pressure, and macrophage activation by wear particles at the bone–implant interface. 15
Cement penetration is a function of pressure applied, resistance, and cement viscosity. 7,16,17 The most common factors that provide resistance to cement penetration are the combination of intramedullary fluid pressure, blood product debris, 11 and cancellous bone debris. 6 Several studies 16,18 –20 have suggested that optimal prosthesis fixation requires cement penetration into the proximal tibia by 3–4 mm at least. Walker et al. 16 proposed a requirement of 3–4-mm mantle thickness to engage at least one level of transverse trabecular and sufficient vertical channel curves. Optimal cement penetration can be achieved by uniform bone density with an absence of sclerosis, 21 sufficient drill-hole interdigitation, 22 pulsed lavage, 11,22 –24 absence of bone debris in cancellous bone, 6,24 –26 absence of blood at the cement–bone interface, 11 and reduced intraoperative bleeding. 10,12,27
Our hypothesis was that tourniquet use will improve cement penetration in TKR by reducing the intramedullary bleeding pressure and blood clot. Hence, the purpose of this single-blinded, prospective randomized superiority trial was to evaluate the influence of using or not using a tourniquet in achieving adequate cement penetration (average and central) during TKR.
Methods
Study objective and design
Informed consent was obtained by a clinical nurse from the potential participants prior to their final preoperative consultation with the operating surgeon. All the participants were operated by the same surgeon, using the same cementation technique, the same implant, and in an operating theatre with the same ambient temperature (19°C). Just prior to prosthesis cementation and implantation, patients were randomized intraoperatively into the tourniquet or no tourniquet groups by the anesthetist using a computer-generated random number program, “Random Num Generator for Iphone” (Bice Applications, California, USA). A blinded-independent assessor measured the cement penetration depth for each group.
Participants
Subjects with severe end-stage knee osteoarthritis who had failed nonoperative management and were booked for primary TKR were recruited over a 4-month period. Participants were excluded if they had a history of peripheral vascular disease that precluded tourniquet use or required a semi-constrained prosthesis due to ligament instability necessitating a fixed bearing tibial component with tibial stem.
Statistical analysis
A priori power analysis with G*Power 28 was undertaken for an unpaired Student’s t-test with two independent means (two tailed), α at 0.05 and β at 0.2, i.e. Power (1−β) or 0.8. A difference of 0.75 mm (SD ± 0.8) in the mean cement penetration between each group was determined to be clinically relevant, suggesting a minimum of 19 patients in each group was required. Thus, 42 subjects were recruited to have an optimal attrition rate. Refer to Figure 1, CONSORT flow chart of participants in the trial, for further details of the sampling process. Among the 42 eligible subjects, n = 40 were randomly allocated to group A (tourniquet group, n = 20) and group B (non-tourniquet group, n = 20), and two participants were excluded.

CONSORT flow chart of participants in the trial.
Tourniquet and surgical procedure
In both groups, the knee replacement procedure was commenced with a tourniquet applied but without inflation. The patient’s blood pressure was maintained hypotensive if no contraindications applied, else normotensive. Proximal tibial osteotomy was undertaken using a computerized navigation system, with all resections at 90° to the tibial long axis, removing a planned 10-mm resection of the lateral tibial plateau. After the bone resection and preparation were undertaken, the patients were randomized to group A or B. In group A, the leg was elevated for 1 min, and then, the tourniquet was inflated to 300 mmHg for the duration of the cementing procedure. In group B, the tourniquet was not inflated. NexGen Posterior Stabilized LPS Mobile Bearing knees (Zimmer, Warsaw, Indiana, USA) were performed in all patients by the same 12-year post arthroplasty fellowship surgeon. In both groups, pulse lavage was utilized to copiously irrigate the femoral and tibial bony resected surfaces to remove bone debris and clot, and then, the surfaces were dried with cotton lint-free surgical swabs. Tibial cementation was undertaken with the knee maximally flexed and subluxed forward using a blunt Hohmann retractor placed posterior to the tibia. Tibial and femoral components were implanted within 2 min of mixing using 80 g of vacuum mixed Palacos R+G PMMA (Zimmer). Sufficient PMMA was applied to the tibial component undersurface, the distal femoral bony surface, and the posterior femoral components undersurface, so that excess PMMA would be expressed hydrodynamically from the prosthesis edge. Component impaction was achieved using the supplied tibial impactor and a mallet, using a standardized increasing force in a sequential load pattern until the component was seated flush onto the proximal tibial surface, and no further PMMA egress occurred. Excess PMMA was removed, the tibial polyethylene was inserted, and then axial load was applied via a leg lift technique to the components during PMMA polymerization. In group A, the tourniquet was released after polymerization had occurred, prior to wound closure.
Outcome measurement
Cement penetration depth in the tibial plateau side with the least osteoarthritis was chosen as the outcome measure for a number of reasons. First, the tibial cement penetration was easily measured on postoperative anteroposterior radiographs, compared to femoral penetration depth. Second, using penetration in the least osteoarthritic tibial plateau removed subchondral sclerosis as a confounding factor in penetration. The primary outcome was measured using 16-bit digital anteroposterior postoperative radiographs, taken on the second postoperative day. The radiograph was taken parallel to the tibial tray 16 to enhance the accurate measurement of cement penetration for the entire width of the tibial baseplate. To remove sclerotic subchondral bone as a confounding variable, cement penetration was measured as a primary outcome in the tibial plateau opposite the most arthritic compartment, that is, the lateral plateau penetration was measured in a varus knee with medial osteoarthritis and the medial tibial plateau penetration was measured in a valgus knee. Preoperative long leg radiographs were utilized to assess coronal plane alignment intraoperatively.
The digital radiographs were analyzed with image analysis software (ImageJ 1.45, US National Institute of Health, Bethesda, Maryland, USA) and a personal computer (MacBook Pro, Apple Corporation, Cupertino, CA, USA) by the single-blinded assessor using a semiautomatic technique. 29 Cement penetration measurements undertaken using previously described techniques, 29,30 with the tibial plateau being respectively divided equally into three columns (medial, central, and lateral) and measurements, were undertaken for each column separately. Digital image analysis software (ImageJ 1.45) was used to objectively infer the penetration of the cement by evaluating gradient of grayscale intensity over the cement: osseous interface using a software thresholding technique 31 (See Figure 2, for a diagrammatic representation of the cement: bone thresholding technique). The reliability of using digital radiographic software in the evaluation cement–bone junctions has been previously reported. 32,33 A pixel with an intensity of 0 is black, a pixel with a value of 255 is white, and everything in-between is a shade of gray. Images with 16 bits have 65,536 (216) intensity graduations, with 0 still representing black but 65,536 representing white. Thresholding separates pixels, which fall within a desired range of intensity values from those which do not (also known as ‘segmentation’), in the rectangular region of interest (ROI). The blinded assessor selects the ROI manually under the tibial tray, then selects the cement pixel intensity, with the software defining the cement–bone interface. The distance from the tibial tray to the interface was then manually measured by the observer, using a scale correction base on the know constant of the tibial post diameter.
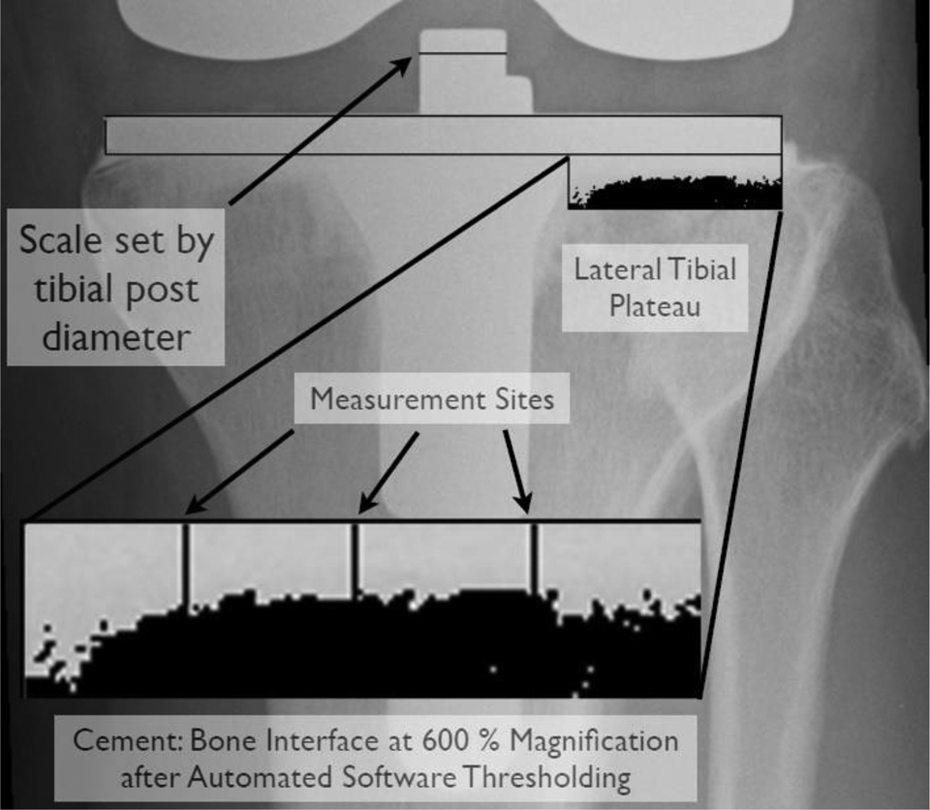
Diagrammatic representation of the software cement: bone interface thresholding technique.
The average penetration (mean of the three columns penetration values of the plateau) and the central penetration were, respectively, considered for the data analysis. Known tibial baseplate size characteristics, thickness, and stem diameter were used to normalize penetration measurements.
Statistical methods
The sample size and power calculation measures were analyzed for a two-tailed Student’s t-test (α = 0.05; β = 0.2 and power = 0.8) prior to the study using G*Power 28 analysis software. Demographic variables and key clinical characteristics are summarized (mean ± SD) with standard descriptive statistics (refer to Table 1). Table 1 presents the baseline characteristics of the participants, demonstrating uniform distributions between the participants in each group. Mean and SD were calculated for both groups on the least arthritic (contralateral) tibial plateau’s average and central penetrations. An unpaired Student’s t-test (two tailed) was used to analyze the intergroup differences (p = 0.05) of the cement penetration depth, respectively, of both groups, on the contralateral tibial plateaus. The estimated effect size 34 was calculated using standard mean differences (MDs) with 95% confidence interval (CI), to assure the accuracy of the tests of significance between the two groups.
Baseline characteristics of participants.

BMI: body mass index; RA: Rheumatoid Arthritis; M-L: media-lateral.
Results
The measures of variability (mean, SD, between groups MD with 95% CI) are summarized in Table 2. No statistically significant differences in average and central penetration values were observed between the two groups. In group A, the mean penetration was 2.78 ± 0.62 mm compared to group B, which was 2.82 ± 0.68 (p = 0.93). In group A, the central penetration was 2.93 ± 0.67 mm compared to group B, which was 3.01 ± 1.17 mm (p = 0.84). The estimated effect size on the average and central penetration depth on the lateral tibial plateau between the groups demonstrated 100% overlap (effect size, −0.06 and −0.08), which shows no differences in cement penetration depth between the experimental groups. No intraoperative adverse events occurred, and no postoperative adverse events were reported. No radiolucent lines were noted on the immediate postoperative X-ray of any of the participants.
Results of average and central cement penetration depth between the tourniquet (A) and no tourniquet (B) groups.

MDs: mean differences; CI: confidence interval.
Discussion
The advantages of using a tourniquet remain controversial in TKR. Improved cement penetration due to the absence of bleeding has been suggested as one unproven advantage of tourniquet use; however, our results do not support this.
A recent meta-analysis by Li et al. 1 of tourniquet use in TKR recommended the need for future high-quality randomized control trials to validate its effectiveness and identified the potential benefits of tourniquet use as reduced intraoperative blood loss and improved surgical field visualization. The authors also reported inconclusive evidence or no significant difference in other important clinical parameters, including operative time, total blood loss, thromboembolic events, length of hospital stay, pain and range of motion, or return to activities of daily living when comparing tourniquet use or nonuse. Another meta-analysis by Smith et al. 3 reported less manipulations under anesthesia were required and reduced postoperative complications, including bleeding, hematoma, infection, blisters, swelling, and nerve injuries without tourniquet use. In a randomized trial by Tai et al. 35 not using a tourniquet revealed reduced biomarkers of soft tissue trauma and clinical superiority in achieving short-term functional progress, such as earlier straight leg raising and greater knee flexion angle; however, the length of hospital stay was similar when compared to tourniquet use. Not using a tourniquet also has economic consequences with reportedly increased operative time. 36 The tourniquet inflation pressure is also a variable, with recent studies 35,37,38 suggesting a reduced incidence of nerve injury and enhanced postoperative functional recovery with the use of a low-pressure tourniquet. A recent meta-analysis by Alcelik et al. suggested the need for further studies focusing long-term benefits of a tourniquet use. 2
Given that adequate cement penetration and resultant bony microlock provide sufficient implant stability to decrease component migration and subsequent loosening, our results are in agreement with Ledin et al. 39 who recently performed a radiostereometric analysis trial of 50 patients with and without tourniquet. They found no difference between the two groups in regards component migration at two years.
Hence, while tourniquet use provides advantages, such as reduced total and intraoperative blood loss, in this article, greater tibial cement penetration did not occur. This is the first study to clinically evaluate the influence of tourniquet use on cement penetration depth. Our study result revealed level II clinical evidence of no superiority from tourniquet use in improving the cement penetration depth of the tibial component. While cement penetration is only an indirect measure of component stability, inadequate cement penetration has been shown to result in component instability. 40,41
Confounder adjustments were not considered in the data analysis, since demographic findings were uniform in terms of age, sex, body mass index, and type of knee deformity. Our study had a sufficient sample size for construction of relevant effect size (with 95% CI) specific to the trial outcome. There is a lack of prior validation studies of bone: cement interface measurement using digital image analysis software. However, we utilized a previously described semiautomated cement penetration assessment technique on each group, 30 by a blinded independent observer, on the less arthritic tibial side. Measurement of tibial cement penetration on the non-arthritic tibial plateau represents a reasonable in vivo model of cement penetration into non-sclerotic bone as previously described and removes the confounder of sclerosis decreasing penetration. 30 Edge detection measurement software on digitized radiographs has been reported to be 6.4 times more accurate than manual techniques, with error rates of 3.6% versus 23.1%. 31
Our results are potentially not transferrable to the femoral component cement penetration without tourniquet. Femoral component penetration is not measurable on plain radiographs in a posterior stabilized TKR, such as the prosthesis routinely used by the senior author, and would require computerized tomography to visualize, with much greater irradiation as a result.
Based on our data, it would appear that copious saline lavage, knee hyper-flexion during component insertion, drying of the bony surfaces during cementation, and maintenance of leg lift pressure during polymerization sufficiently cleared the cancellous spaces of blood and bone debris during the cementation process, allowing adequate cement penetration.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.