
Abstract
Background:
Zimmer iASSIST knee is an accelerometer-based navigation system with the aim of achieving better alignment in total knee arthroplasty (TKA). We have started using this system since early 2016. This is a retrospective case–control study, which aims to compare the radiological alignment, operation time, and blood loss of TKAs performed using the iASSIST system and those using conventional techniques.
Materials and Methods:
42 TKAs using Zimmer iASSIST and 44 TKAs using conventional instrumentation were recruited. The overall coronal alignment and the coronal and sagittal alignment of the femoral and tibial component were compared. For coronal alignment, additional analysis of the absolute deviation from neutral mechanical axis was performed to avoid canceling out of varus/valgus deviation. The number of outliers, operation time, and blood loss in terms of maximal hemoglobin drop were also compared.
Results:
When comparing the alignment of the iASSIST group with the conventional group, there were no significant differences (p > 0.05) in the number of outliers, mean coronal alignments, mean deviation from neutral coronal mechanical axis (2.9° vs. 2.9°), and femoral component flexion angle (4.9° vs. 4.7°). The difference in the mean tibial component posterior slope was significant (5.7° vs. 7.1°, p < 0.05). The mean operation time was significantly longer by 13 min (p < 0.05) in the iASSIST group. There were no significant differences in the mean hemoglobin drop between the two groups.
Conclusion:
The results demonstrated no significant differences in terms of coronal radiological alignment, femoral flexion angle, outliers, and blood loss between iASSIST and conventional technique. There was a small but statistically significant difference in tibial posterior slope. The iASSIST group needed a longer operation time.
Introduction
Improving the accuracy and mechanical alignment had been a key area of development in total knee arthroplasties (TKAs). Deviation of more than 3° from neutral mechanical axis had been associated with less satisfactory implant survival and functional outcome. 1 Some studies have shown that image-based navigation systems can give better results in terms of radiological alignment compared to conventional techniques. 2,3 However, these systems typically require dedicated preoperative or intraoperative imaging and sometimes need to utilize instruments that are outside the surgical field. Placement of additional pins and line-of-sight problems may also be a source of inconvenience when using these systems. 4,5
Zimmer iASSIST knee system (Zimmer, Warsaw, Indiana, USA) is an accelerometer-based navigation system that became commercially available in 2012. The system aims to achieve more accurate femoral and tibial cuts using navigation while avoiding the issues that limit the use of other image-based systems. It also has the added benefit of using an extramedullary technique for both tibia and femur, which is associated with less blood loss. 6 Compared to conventional techniques, iASSIST can be used even when there are preexisting implants within the medullary canal or when marked deformity makes it difficult to use conventional instrumentation. Our department has started using this system since early 2016. This is a retrospective case–control study, which aims to compare the radiological alignment, operation time, and blood loss of TKAs performed using the iASSIST system and those using conventional techniques.
Materials and methods
This is a retrospective review of all the primary TKAs performed using iASSIST in 2016–2017. 42 TKAs using Zimmer iASSIST were recruited. They were compared to 44 TKAs using conventional instrumentation performed in the same period selected using the same criteria. All cases were primary tricompartmental knee osteoarthritis with neutral or varus alignment of not more than 15°, less than 10° fixed flexion contracture, and more than 90° of flexion range. Exclusion criteria include valgus knee deformity and previous hip surgery or replacement to avoid potential interference in limb alignment registration.
For both groups, cuts were set to achieve neutral coronal alignment, 3° femoral flexion angle, and 7° tibia posterior slope. The overall coronal alignments, the coronal and sagittal alignment of the femoral and tibial components, and the number of outliers with respect to coronal alignment were compared.
A total of four iASSIST cases were excluded. For two cases, significant medial laxity resulting from medial collateral ligament injury was noted intraoperatively. They were converted to constrained implants and were excluded. One excluded case had a history of femoral fracture and navigation was used only for the femoral side. Conventional technique was used for the tibial side as intended preoperatively. One patient had previous total hip replacement performed on the same limb and was therefore excluded.
The study was approved by the Hong Kong Hospital Authority New Territories West Cluster Research Ethics Committee (ref. no. NTWC/REC/19008).
Surgical techniques
All surgeries were performed by the same group of surgeons in a Joint Replacement Center of a regional hospital. The medial parapatellar approach was used. All the implants used were Zimmer Nexgen LPS flex posterior stabilized total knee prosthesis.
For the conventional group, intramedullary guides for femur and extramedullary guides for tibia were used.
For the iASSIST group, registration of mechanical axis and adjustments were made using specialized electronic pods. For the femoral side, the electronic pod was attached to a bone spike that was impacted at the distal end of the femur. The position was registered by accelerating and stopping the lower limb multiple times in a star-shaped or circular manner. The cutting guide was attached and adjustments were made according to the calculations made by the system. After the resection, a pod was placed on the cutting surface to validate the cut using calculations made with the lower limb in abduction, adduction, and neutral position. Tibial registration was performed using a pod attached to an extramedullary guide rod. The lower limb was brought to adduction, abduction, and neutral position. After the registration, the cutting guide was placed taking into account the calculated adjustment suggestions. After the resection, the cut was again validated by attaching a pod to the cut surface.
X-Ray measurements
The coronal alignments were measured using standing lower limb alignment films. The films were taken with the beam centered at the knee joint. The beam was shined as perpendicularly as possible to the joint line. Positive values were used to denote varus alignment, while negative values were used to denote valgus alignment. The overall mechanical axis was the angle measured between a line drawn from the center of the femoral head to the midpoint of a line drawn between the most distal part of the femoral condyles (mid-condylar point) and a line from the middle of the tibiotalar joint to the mid-condylar point (Figure 1).

Overall coronal alignment.
The coronal alignment of the femoral component was represented by the angle between a line drawn from the femoral head to the mid-condylar point and a line perpendicular to the line joining the most distal points of the femoral condyles (Figure 2).

Femoral coronal alignment.
The coronal alignment of the tibial component was represented by the angle between a line drawn from the midpoint of the tibiotalar joint to the midpoint of the tibial tray and a line perpendicular to the tibial tray (Figure 3).

Tibial coronal alignment.
The mean deviation from neutral mechanical axis was analyzed to avoid canceling out of varus/valgus deviation. For example, a 3° varus and a 3° valgus malalignment would both be considered as 3° in the calculation of the mean deviation from neutral.
Sagittal alignment of femoral and tibial components which translate to flexion angle of femoral implant and posterior sloping of tibial implant was measured using standard lateral X-rays of the knee. The femoral flexion angle was the angle measured between the mid-intramedullary axis and the distal bone-implant contact surface. The tibial posterior slope was the angle between the mid-intramedullary axis and the bone-implant contact surface of the tibia (Figure 4).
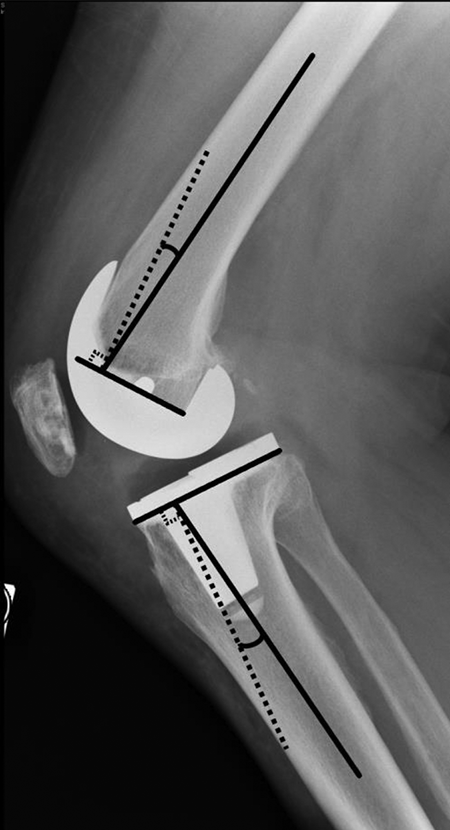
Femoral and tibial sagittal alignment.
Other measurements
Blood loss was estimated using the maximal difference between preoperative hemoglobin concentration and postoperative hemoglobin concentration. Hemoglobin concentration was routinely measured on day 0, day 1, and day 5 postoperatively. All cases adhered to standardized perioperative blood management and intraoperative intra-articular transamin injection protocol. Operation time was taken from the operation records.
Statistical analysis
The data were analyzed using statistical package for the Social Sciences (SPSS) version 16.0.
In this study, continuous variables, including age, alignment, operation time, and blood loss, were analyzed using the independent sample t-test, while categorical variables, including sex, transamin use, and number of outliers, were analyzed using the Pearson’s χ 2 test provided in the SPSS program.
Outliers were defined as cases with coronal plane measurements outside 3° varus or 3° valgus.
Analysis of the absolute deviation from neutral mechanical axis on the coronal plane was provided as an additional outcome measurement method. In this part of analysis, both varus deviation, denoted in positive values, and valgus deviation, denoted in negative values, were converted to their absolute values. The mean will then be generated from this absolute value and statistical analysis will proceed using the independent sample t-test as in other parts of this study. This method was intended to avoid canceling out of varus and valgus deviation in the mean value and should serve as a direct and quantitative measurement of how much deviation from neutral coronal alignment the studied cases had experienced.
Results
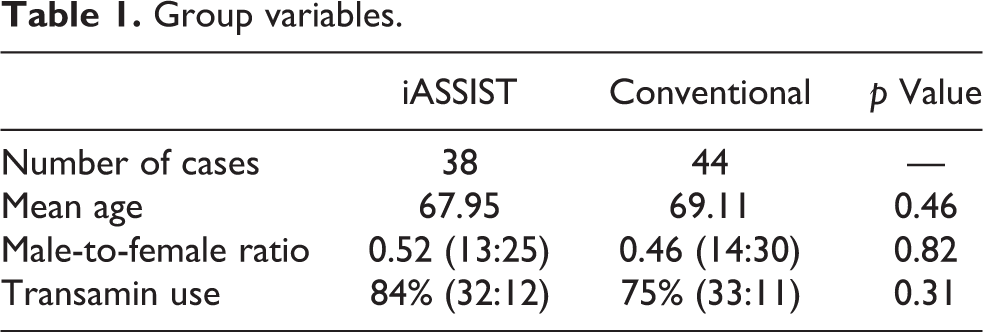
The iASSIST group and conventional group have no significant differences in age and sex distribution. They also have no significant differences in percentages of intra-articular transamin use (Table 1).
Group variables.
There were no significant differences (p > 0.05) in the mean overall and component coronal alignments and femoral component flexion angle (4.9° vs. 4.7°) between the two groups. The difference in the mean tibial component posterior slope was significant (5.7°vs. 7.1°, p < 0.05) (Table 2).
Perioperative outcomes: mean (standard deviation).a

a For coronal alignments, positive values denote varus and negative values denote valgus.
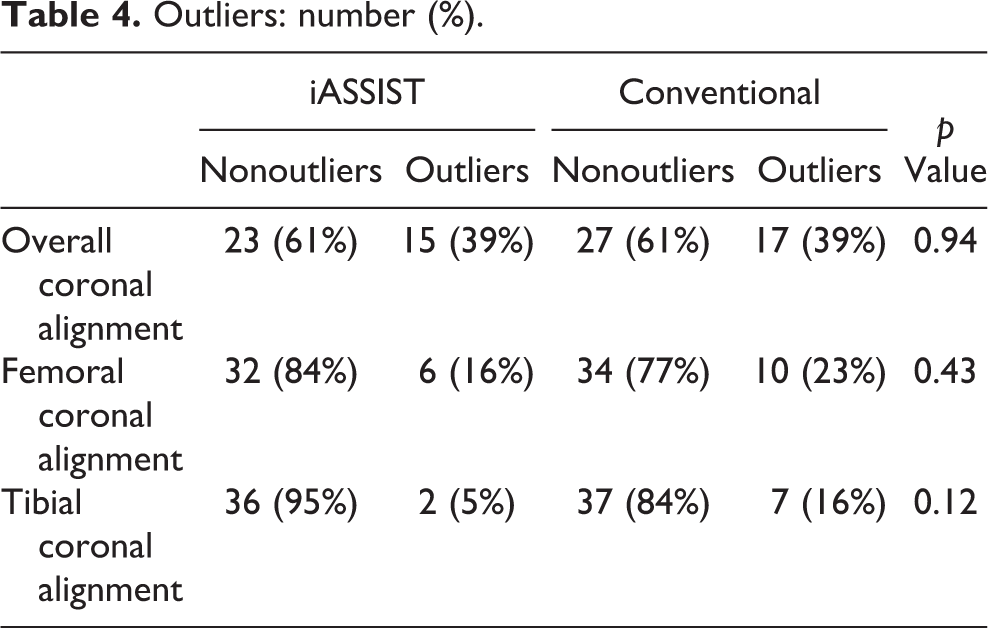
There were no significant differences (p > 0.05) in the percentage of outliers for overall coronal alignment (39% vs. 39%). There were fewer outliers for the iASSIST group in terms of femoral coronal alignment (16% vs. 23%) and tibial coronal alignment (5% vs 16%), however, the difference was not statistically significant (p > 0.05) (Table 4).
When absolute values were used to avoid canceling out of varus and valgus malalignments, there were no significant differences (p > 0.05) in the overall (2.9° vs. 2.9°), femoral component (1.9° vs. 2.1°)and tibial component (1.4° vs. 1.8°) mean deviation from neutral mechanical axis (Table 3).
Results using absolute values.
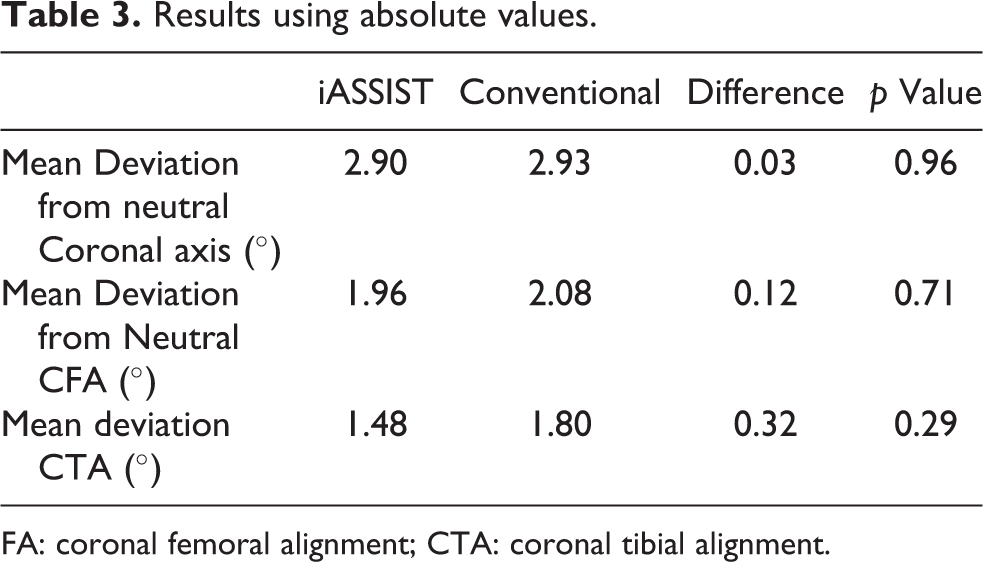
FA: coronal femoral alignment; CTA: coronal tibial alignment.
Outliers: number (%).
The mean operation time was significantly longer by 13 min (100 min vs. 87 min, p < 0.05) in the iASSIST group. There were no significant differences in the mean hemoglobin drop between the two groups.
Discussion
Zimmer iASSIST is a new type of imageless navigation system. It relies on accelerometers to estimate the lower limb alignment intraoperatively. Its advantage over older navigation systems lies in the fact that it does not require dedicated preoperative computed tomography/magnetic resonance imaging. It also avoids the use of additional pins and is not affected by line-of-sight problems intraoperatively. 4,5 Currently, there is still limited amount of literature on this subject, but the results thus far are promising and are at least comparable 7,8,9 or superior in terms of coronal alignment when compared to other navigation systems 10 or conventional techniques. 11 –13 Overall, comparable results can be demonstrated in cases performed in our center in terms of alignment. The system is also relatively easy to use. The two cases that required conversion to conventional implants were due to medial collateral ligament injury during dissection and not related to the iASSIST equipment.
Our results showed no significant differences in terms of the number of outliers and mean coronal alignment between iASSIST and conventional technique. These findings were consistent with that of Moo et al. 7 We have also provided an additional analysis method using absolute values of varus and valgus malalignment similar to that provided by Desseaux et al. 10 The aim of this method was to avoid canceling out of varus and valgus malalignment and to provide a direct and quantitative measurement of how much deviation from neutral coronal alignment the studied cases had experienced. Using this technique, the results also showed no significant differences in coronal alignment between both iASSIST and conventional techniques.
There was a small but statistically significant difference in terms of the posterior sloping of the tibial component between the two groups. The mean posterior sloping measured on the films in our study was 5.7° for iASSIST and 7° for conventional. It was noted that some degree of freedom on the sagittal plane was possible during the placement of the extramedullary guide rod for conventional technique. Surgeons in our center tended to shift the distal attachment of the rod more anteriorly to ensure adequate posterior slope, this may explain the larger posterior slope in the conventional group.
Although iASSIST does not require intramedullary guide and therefore blood loss due to bone bleeding should be theoretically less, the authors were unable to demonstrate a significant difference in terms of drop in hemoglobin concentration measured following a fixed schedule postoperatively.
The mean operation time using iASSIST was significantly longer by 13 min. This may be because of the surgeons’ learning curve and also the additional steps required for the alignment registration when using the iASSIST navigation system.
Limitations
This is a retrospective case–control study conducted in a regional hospital. In our center, the majority of total knee replacements are performed using non-navigated techniques, with iASSIST only accounting for a small proportion of TKAs performed each year. This led to the limited sample size in the current study.
The focus of the current study is to establish whether the radiological alignment in TKAs performed using iASSIST has any significant differences when compared to conventional techniques. The functional outcomes of the patients including knee scores were not analyzed.
Cases with valgus knee or gross deformities (e.g. excessive femur bowing) were not included in this study, and thus, the results may not be applicable for more complex cases requiring TKAs.
Conclusion
The results demonstrated no significant differences in terms of coronal radiological alignment, femoral flexion angle, outliers, and blood loss between iASSIST and conventional technique. There was a small but statistically significant difference in tibial posterior slope. The iASSIST group needed a longer operation time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.