
Abstract
Cervical endoscopic spinal surgery (CESS) is now regularly performed in some centres in the Far East, yet rarely in Europe and the United States. This review describes the application of CESS through anterior and posterior approaches with analysis of the available evidence supporting current techniques. An electronic literature search identified 52 papers and proceedings’ abstracts of which 25 (16 anterior approach and 9 posterior approach) provided comparable clinical outcomes. The results revealed a good or excellent outcome from CESS in 91% (range 74–100%) with a complication rate of 5%. In a local cohort study, patients had 72% less neck pain (visual analogue scale rating) and 81% less arm pain at 6 months when CESS was used as an isolated procedure, and 74% less neck pain and 83% less arm pain when coupled with disc replacement or fusion at an adjacent level.
Keywords
Introduction
In the last 20 years, surgeons advocated minimally invasive surgical approaches to the spine, with the aim of lessening paraspinal muscle damage and hastening recovery. In contrast to traditional surgery that necessitates complete disc excision, the new techniques aim to preserve disc function by resecting only the material causing cord or exiting nerve root compression. These approaches aim to maintain segmental function and lordotic sagittal balance, reducing stress on adjacent discs and premature or enhanced segmental degenerative change. 1,2
Although some attempts were made in the 1990s to resect cervical discs by minimally invasive anterior approaches, 3,4 the techniques used were not widely taken up due to the inherent dangers associated with the surgical approach and lack of well-designed equipment. More popular were intradiscal percutaneous techniques in which the centre of the disc was targeted, 5,6 including chemonucleolysis, 7 automated percutaneous discectomy 4 and laser discectomy. 8 It was not until 2005, on the back of successful resection of lumbar discs using direct and transforaminal endoscopic techniques, 9,10 that surgeons again focused on disc preservation. 11,12
Although it is well recognized that posterior cervical lamino-foraminotomy for disc resection and/or root foramen widening will minimize blood loss and enhance patient recovery compared to most forms of anterior surgery, 13 the benefits in terms of clinical outcome are less well established. The reason behind this is that different posterior surgical methods have been employed by surgeons, 14 ranging from microsurgery via tubular retractors to purely endoscopic techniques. It is uncertain whether the latter leads to better patient outcomes than the former. In this article, the techniques of anterior and posterior cervical endoscopic spinal surgery (CESS) are described with a review of the evidence supporting these interventions.
Approaches and CESS techniques
Anterior cervical discectomy and foraminotomy
The route of surgical approach to the cervical spine is generally determined by the site of major spinal pathology identified by magnetic resonance imaging. For resection of a soft disc prolapse with anterior cord compression, or foraminal compromise from the uncovertebral articulation, the spine is approached percutaneously via a classical anterolateral neck incision. The patient is laid supine with the neck extended and the shoulders taped down. Although it is possible to perform CESS with the patient under analgo-sedation, with similar regimes to those described for lumbar endoscopic procedures, 15 general anaesthesia limits any potential neck movement and is probably safer.
While retracting the carotid sheath laterally and the oesophagus medially, an 18-gauge needle is inserted down to the margin of the disc. A mini-open approach (1.5-cm skin incision) ensures that damage to the carotid artery, or one of the small thyroid venous branches is avoided. The tip of the needle is carefully advanced 50% across the disc under X-ray image intensifier guidance and a guide wire inserted. Over the wire, 2 and 3 mm dilators are passed to allow placement of a 4.8-mm diameter working channel.
In a young patient with a soft prolapse and normal disc height, a direct approach may be made either from the ipsilateral side or obliquely across the disc. Once the working cannula is correctly sited at the posterior disc margin, a 3.9-mm endoscope (Figures 1 and 2) connected to a high-definition camera system is introduced and the prolapsed disc material identified. In a patient with a narrow disc space, or with a purely foraminal stenosis, it is necessary to ream the uncinate process from the inferior margin of the superior vertebral body with a hollow reamer or endoscopic diamond burr before intra-foraminal material may be removed (Figure 2). Fluid irrigation provides tissue cooling.

Cervical endoscope (joimax GmbH).

Anteroposterior and lateral image intensifier radiographs showing positioning of cervical cannula. 45° oblique views showing reaming of uncinate process with a diamond burr and removal of intra-foraminal disc material with rongeurs.
Posterior cervical foraminotomy and discectomy
Open posterior cervical foraminotomy is frequently used by surgeons when the primary focus of pathology leading to cervicalgia is foraminal stenosis in the presence or absence of an associated disc protrusion. 16 Open surgery however requires detachment of the paraspinal muscles, and this may be associated with post-operative neck pain and spinal instability. 17 To minimize muscle damage clearly, a minimally invasive approach is attractive. Through a stab incision with anteroposterior spinal imaging, a 2-mm diameter dilator tube is placed directly onto the medial margin of the facet joint at the affected intervertebral level. Progressive dilators are then inserted to allow placement of a 7.5-mm working cannula for a 6.3-mm endoscope. A diamond endoscopic burr may then be used to remove the medial margin of the facet and expose the underlying nerve root. To follow the root medially and expose any disc prolapse, the ligamentum flavum is raised like a curtain as shown in Figure 3(a). The exiting root is exposed with rongeurs laterally to its division, taking care to protect the vertebral artery (Figure 3(b)).

(a) Posterior endoscopic foraminotomy showing exiting cervical nerve root and (b) lateral resection revealing the vertebral artery.
Methods
Literature review
Relevant published data from randomized controlled trials (RCTs), controlled clinical trials and cohort studies in any language were identified by the following search strategies: Computer-aided searching of PUBMED (www.ncbi.nlm.nih.gov/pubmed) with the following search terms: cervical disc prolapse, cervical endoscopy, cervical myelopathy, discectomy and endoscopy. Personal bibliographies held by the authors. Citation tracking from all papers identified by the above strategies.
The methodological quality of each study found was assessed and for any randomized trials the risk of pre-allocation disclosure of assignment, any intention to treat analysis and blinding of the outcome assessors noted. 18,19
Results
Literature search – to 31 May 2017
The literature search identified 52 studies but 27 were technical descriptions, case reports, series containing less than five patients, results from disc nucleoplasty (electrical dissolution), or use of a tubular retractor purely to facilitate access to the spine. Of the 16 with substantive clinical data regarding the use of an anterior approach (Table 1), there was only one single-blind (patient aware, independently assessed) RCT 26 comparing the results of full-endoscopic decompression versus conventional anterior decompression and fusion for cervical disc herniations. Similar outcomes were obtained from the two procedures including the number who were able to return to work within 3 months. One cohort study compared the results of full-endoscopic cervical discectomy using an anterior versus a posterior approach. 33 The authors concluded that the clinical outcomes at times up to 18 months were not significantly different but noted that the posterior approach might be preferable when considering the volume of disc removed, length of hospital stay and the postoperative radiographic changes. All the remaining anterior surgical trials were cohort studies mainly describing surgeons’ initial clinical experiences. Nine included the use of laser for thermodiskoplasty, 20,22 removal of residual disc tissue, 23 –25,27,28,34 or selective discectomy, foraminoplasty and annular debridement. 29,30 The remainder used manual endoscopic instruments.
Anterior endoscopic studies.

RCT: randomized controlled trial; ACDF: anterior cervical decompression and fusion; Dec: decrease; NDI: neck disability index; VAS: visual analogue scale; Ho:YAG: Holmium: Yttrium–aluminium–garnet; PECD: percutaneous endoscopic cervical discectomy; PEEK: polyetheretherketone.
aSatisfaction – excellent or good.
Nine trials described posterior endoscopic techniques, of which five provided patient reported outcome data. 11,35 –38 One trial was quasi-randomized with the patients alternately assigned to conventional anterior cervical decompression and fusion (ACDF) or full-endoscopic posterior surgery 11 (Table 2). The rate of complication in the 486 patients was 6.4% with 4.5% requiring revision surgery.
Posterior endoscopic studies.

RCT: randomized controlled trial; ACDF: anterior cervical decompression and fusion; NDI: neck disability index; VAS: visual analogue scale.
aSatisfaction – excellent or good.
Considering all the trials as a group, excellent or good outcomes were apparent for up to 24 months in the majority of the 1643 patients reported, with 4.6% incidence of reported complications and a 3.4% incidence of reported revision surgery.
In a local series, 41 9 patients were treated with single-level disease (1 C4/5, 7 C5/6 and 1 C6/7) and in 12 endoscopy was used as an adjunctive therapy to disc fusion/arthroplasty at adjacent or interval levels (seven single and five double; four ACDF and eight disc arthroplasty – Figure 4). Patients with multilevel disease were slightly older (mean ages 45 ± 10 and 55 ± 10 yrs, respectively) and had slightly higher disability scores (Table 3). Both groups improved to a similar final level with respect to disability, with marked lessening of their neck and arm symptoms.

Preoperative sagittal/axial T2 images and post-operative lateral radiographs of patient treated by discarthroplasty at C5/6 (M6, Lindare Medical, UK) and CESS at C6/7. CESS: cervical endoscopic spinal surgery.
Results from cohort study.
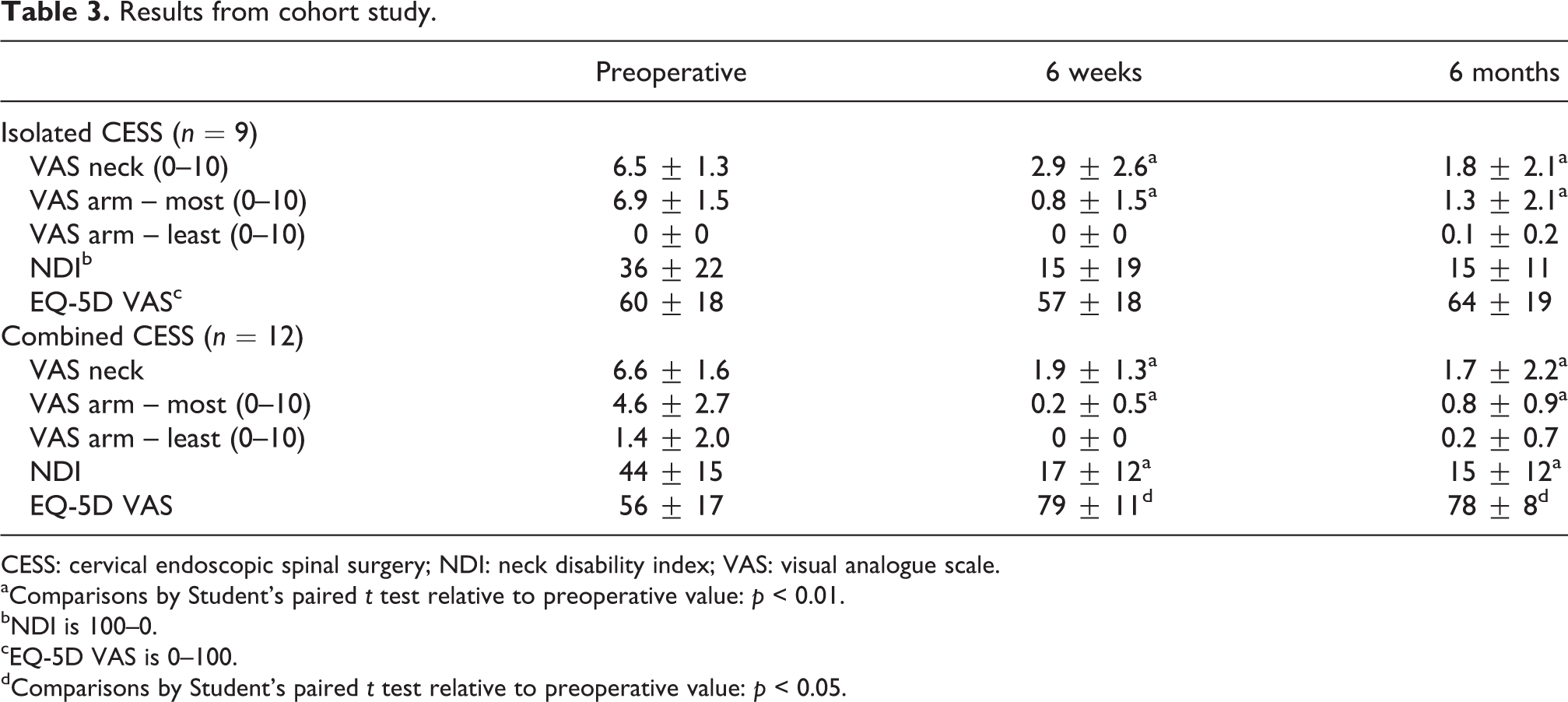
CESS: cervical endoscopic spinal surgery; NDI: neck disability index; VAS: visual analogue scale.
aComparisons by Student’s paired t test relative to preoperative value: p < 0.01.
bNDI is 100–0.
cEQ-5D VAS is 0–100.
dComparisons by Student’s paired t test relative to preoperative value: p < 0.05.
Discussion
There still remains a paucity of data from high-quality studies of CESS with long-term follow-up. However, with respect to the anterior approach to the cervical spine, it is clear from the available data that CESS is associated with satisfactory outcomes in terms of clinical response to surgery, patient satisfaction and improvement in quality of life. Data suggest that radiating arm pain and lateral disc herniation are the most important factors by which a surgeon may predict an excellent outcome. 22 The complications of surgery at approximately 5% with both anterior and posterior approaches had an incidence equivalent to that expected from open cervical surgery 11,26,42 and there appeared to be a low rate of procedure revision. The latter may have been a reflection of a generally short clinical follow-up.
Although a loss of disc height was evident in some trials following surgery, despite the minimally invasive nature of the procedure, sagittal alignment may actually improve when the range of motion is maintained. 31 Universally, the literature indicated that patients could expect a shorter hospital stay and more rapid rehabilitation than after an anterior cervical discectomy and fusion. It is reasonable to expect therefore that CESS would be a cost-effective procedure, although this was not factored into any of the studies.
The literature review unfortunately only provided evidence from one RCT 26 and one quasi-randomized RCT. 11 In consequence, meta-analysis of multiple trials could not be provided and any conclusions from our analyses do have to be interpreted with caution. It is particularly important to note that the current data did not prove that the reported short-term benefits of CESS will be maintained or reduce the requirement for revision surgery. However, it is shown in one study that neither loss of any disc height nor progression of degeneration of the disc itself compromised clinical outcomes at a follow-up of 4 years. 31 Several authors from their exclusion criteria showed that access to a migrated or sequestered disc prolapse behind the vertebral body is technically difficult by either an open or endoscopic transdiscal approach. In this circumstance, it has been suggested that a transcorporeal route may be advantageous 43 and due to the very narrow surgical field through the vertebral body, the use of an endoscope with a high visual angle may be ideal. 44
Use of a laser in addition to rongeurs, cutting blades and radiofrequency disc coblation was reported in nine of the trials. This was usually a side-firing Ho:YAG probe used for the removal of remnants of the posterior herniation and/or foraminoplasty. It was not possible to apportion any disc destruction to the laser or manual instruments, nor to relate reported complications to either technique. There was no report of laser use through a posterior approach where entry to the foramen was universally made by high-speed burr.
Many patients do present with multilevel cervical disease. This is a confounding factor in any analysis of clinical outcomes following cervical disc surgery as it is always difficult to pinpoint symptoms to a single level. The average patient cohort in the analyses presented was small and larger studies are clearly required to limit this effect in any comparative group. It was not clear in any of the trials as to the criteria for a given procedure when an adjacent or separate level showed ‘minor’ disc damage, which clearly could have influenced outcome.
One place for endoscopic surgery, as indicated in our local series, 41 is as an adjunct to disc arthroplasty or fusion to reduce the need for multilevel total disc excision. Due to the small instrument calibre, CESS is optimally positioned as a treatment for localized or foraminal pathology rather than for a broad prolapse with significant cord compression, as illustrated in Figure 4. A weakness of this study was that the data did not allow the surgeon to distinguish improvements secondary to the endoscopy or from the other surgery performed. All that can be stated is that endoscopy at one level did not appear to detract from production of overall satisfactory outcomes in these patients.
Less evidence was available in the literature to support the posterior approach to the cervical spine but the available evidence was strong. It is clear that posterior foraminotomy has a place in the surgeon’s armamentarium, but it should be noted that the results from the only RCT were compared against those after ACDF 11 and data are still required to prove the expected additional benefits of endoscopy over those of an open approach. One advantage might be the lesser injury to the cervical facet joints with a reduced chance of development of a progressive kyphosis. Won et al. 37 in their paper suggest that cervical hypo-lordosis of less than 10° may not be a contraindication for endoscopic foraminotomy, provided the change in cervical curvature is non-structural. It should also be recognized that although the posterior approach may preserve movement at the affected level, not resecting the anterior foraminal osteophytes may allow the development of recurrent stenosis with the passage of time and longer term outcome data are required.
Conclusion
Cervical endoscopic surgery is increasingly practiced around the world, with the aim of minimizing disc damage and retaining intra-discal height without insertion of a ‘spacer’ device. However, few high-quality studies currently exist and the majority of these have limited follow-up. We therefore recommend that surgeons prospectively record patient reported outcomes and satisfaction ratings in all patients undergoing CESS. In addition, level 1 clinical trials should be organized, ideally with 5- to 10-year patient follow-up, to underwrite the conclusions presented.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JNAG received payments for teaching and travel from joimax GmbH
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.