
Abstract
Purpose:
This study compared the clinical outcome of K-rod dynamic internal fixation versus microendoscopic discectomy (MED) for the treatment of single-segment lumbar disc herniation.
Methods:
This retrospective study included 34 patients with L4-L5 single-segment lumbar disc herniation who underwent K-rod dynamic internal fixation (n = 18) or MED (n = 16). The pain was evaluated by the Oswestry disability index (ODI) and visual analogue scale (VAS). The neurological function was assessed by the Japanese Orthopaedic Association (JOA) scores. The height of intervertebral space was calculated using X-ray images, and the disc degeneration was evaluated based on Pfirrmann scores. The mean follow-up time was 31 months (range, 18–46 months).
Results:
In both groups, the ODI scores, VAS scores and JOA scores were significantly improved at the last follow-up compared with the preoperative values (p < 0.05). There was no significant difference in the improvement of ODI, VAS and JOA scores between the two groups (p > 0.05). The height of intervertebral space in the surgical segments, proximal segments and distal segments, was significantly greater in the K-rod group than in the MED group. The disc degeneration occurred more in the MED group than in the K-rod group (p < 0.05).
Conclusion:
K-rod internal fixation and MED produce satisfactory outcomes in the treatment of single-segment lumbar disc herniation. K-rod internal fixation is superior to MED in preventing adjacent segment degeneration.
Introduction
Lumbar disc herniation occurs when the nucleus pulposus in the centre of the disc protrudes posteriorly and often compresses the adjacent lumbar nerve root, leading to low back pain and radiating nerve pain. 1 Symptomatic lumbar disc herniation affects approximately 3% of general population, and approximately 15–20% of these patients require surgical intervention. 1,2 The surgical approaches for lumbar disc herniation include conventional open discectomy, microendoscopic discectomy (MED) and percutaneous endoscopic discectomy. 3 MED has been reported to be a safe and effective technique for the treatment of lumbar disc herniation and has some advantages over conventional open surgery such as less surgical trauma, minimal intraoperative blood loss, shorter length of hospital stay and less post-operative recovery time. 4 –7 However, MED has also been reported to be associated with more dural tear, root injury and recurrent herniation compared to open surgery. 8,9 In addition, a recent meta-analysis compared the outcomes of MED versus open discectomy for lumbar disc herniation and found that MED was associated with less blood loss, shorter length of hospital stay and longer operation time. 10
Disc degeneration can induce spinal instability, and spinal fusion surgery is sometimes required to reduce spinal instability. 11 However, spinal fusion surgery has been reported to increase the degeneration of adjacent segments. 12 Dynamic stabilization system has been found to decrease adjacent segment degeneration, reduce the loading on the intervertebral disc and improve spinal stability. 13 The K-rod system is one type of the dynamic stabilization devices, which is designed to maintain natural motion of the vertebrae and thus prevent adjacent segment degeneration. The K-rod system has been used for the treatment of lumbar disc herniation with satisfactory outcomes. 14 In this study, we compared the outcome of K-rod dynamic internal fixation versus MED for the treatment of single-segment lumbar disc herniation.
Materials and methods
Patients
The medical ethics committee of our hospital approved this study. This retrospective study included 34 patients with L4-L5 single-segment lumbar disc herniation who underwent K-rod dynamic internal fixation (n = 18) or microendoscopic discectomy (n = 16) at our hospital between December 2010 and July 2013. All patients presented with back pain with radiating pain or numbness in the lower limb and positive Bragard’s sign. The diagnosis of lumbar disc herniation was confirmed by computed tomography (CT) or magnetic resonance imaging (MRI). Patients who were refractory to conservative treatment or recurrent patients after conservative treatment were included in the study. Patients with age >55 years, osteoporosis, severe lumbar instability with lumbar degenerative spondylolisthesis and severe spinal deformity were excluded. All patients were followed up for more than 1 year after surgery
Surgical procedure
Patients in the K-rod group were administered general anaesthesia. The patients were in a prone position with elevated abdomen, and the diseased segments were identified and marked under a C-arm fluoroscope. A vertical midline posterior lumbar incision was created. The paravertebral muscles were dissected along the spinous process. The bilateral lamina and interlaminar space were exposed in subperiosteal fashions and extended to the lateral margins of the facet joints. The pedicle screws were inserted at L4 and L5 with the entry points at the apex of the lambdoidal ridge. The K-rod system used in this study consisted of titanium alloy pedicle screws, polyetheretherketone (PEEK) rod (diameter, 5 mm) and titanium alloy tubes (Figure 1). All K-rods were cut to appropriate lengths and passed through the head of the screws. The rods were kept in a straight position, and an anti-rotation device (Paonan Biotech Co. Ltd, Taiwan) was used to prevent the bending of the rods. Interlaminar fenestration decompression was performed by removing part of the lamina, the edge of the facet and the ligamenta flava. Then, to reduce the compression of the nerve root, the nucleus pulposus and its surrounding degenerative tissues were removed. After the drainage tube was placed, the incision was closed.
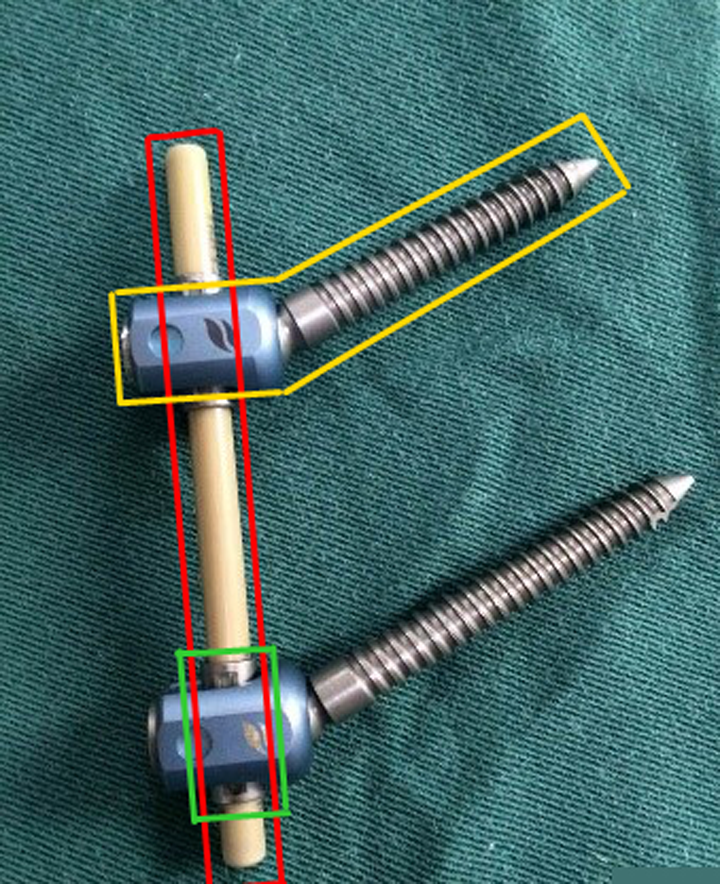
The K-rod system used in this study. Yellow square: titanium alloy pedicle screws; red square: PEEK rod; Green: titanium alloy tube; PEEK: polyetheretherketone.
Patients in the MED group were in a prone position with elevated abdomen. The diseased segments were identified and marked under a C-arm fluoroscope. The patients underwent local infiltration anaesthesia with lidocaine. The patients were awake during the operation, and were informed to describe the presence of nerve root stimulation symptoms, thus avoiding intraoperative damage to the spinal nerve root. A 1.6-cm longitudinal incision was created at 1.5 cm lateral to the midline posterior lumbar region. The incision centred over the spinal needle and deepened to the deep fascia. The paravertebral muscles were dissected along the spinous process. After dissection of the paravertebral muscles in subperiosteal fashions, the needle was targeted superiorly at the disc level of the herniation. The target site was the low border of the lamina of the superior vertebrae. After a series of dilators were sequentially inserted, a final working channel was created by inserting a tubular retractor and was confirmed by real-time radiological images. The endoscopic instruments were then installed. After the soft tissue on the bottom of the working channel was cleared, the part of the lamina, the internal edge of the facet and the ligamenta flava were removed. Then, to reduce the compression of the nerve root, the nucleus pulposus and its surrounding degenerative tissues were removed. After the endoscopic instrument and tubular tractor were removed, the incision was closed. All surgeries were performed by the same surgeon (J. Zhao).
Follow-up
All patients were followed up at 1, 3, 6 and 12 months after surgery. One year after surgery, the patients were followed up yearly. The pain was evaluated by the Oswestry disability index (ODI) and visual analogue scale (VAS). The neurological function was assessed by the Japanese Orthopaedic Association (JOA) scores. All patients underwent anteroposterior and lateral X-ray and 3.0T MRI. Using X-ray images, the height of intervertebral space was calculated as the average distances between the adjacent vertebral bodies at the anterior and posterior border (Figure 2). Using midsagittal T2-weighted MRI images, the disc degeneration was evaluated based on Pfirrmann scores (Figure 3). 15

Lateral X-ray images showing the height of the intervertebral space before (a, c) and after (b, d) surgery in the K-rod group (a, b) and MED group (c, d). MED: microendoscopic discectomy.

The MRI images showing the disc degeneration based on Pfirrmann scores before (a, c, e, g) and after (b, d, f, h) surgery in the K-rod group (a, b, e, f) and MED group (c, d, g, h). MED: microendoscopic discectomy; MRI: magnetic resonance imaging.
Statistical analysis
Analyses were performed using SPSS 12.0. Numerical values are presented as mean and standard deviation. Student’s t-test was used to compare the difference between groups. Categorical data were compared with χ 2. For ranked data, Wilcoxon rank-sum test was used to compare the difference between groups. Probability values less than 0.05 were considered statistically significant.
Results
Table 1 summarizes the baseline characteristics of patients in the two groups. There were no significant differences in sex, age and adjacent segment degeneration between two groups (p > 0.05; Table 1). The operation time and intraoperative blood loss were significantly less in the MED group than in the K-rod group (p < 0.05; Table 1). All patients had complete follow-up information. The mean follow-up time was 31 months (range, 18–46 months). There was no significant difference in the follow-up time between the two groups (Table 1).
The baseline characteristics of patients in the two groups.

MED: microendoscopic discectomy.
a p > 0.05.
b p < 0.05 versus K-rod group.
The preoperative ODI scores, VAS scores and JOA scores were not significantly different between the two groups (p > 0.05; Table 2). For patients in both groups, the ODI, VAS and JOA scores at the latest follow-up improved significantly compared with the preoperative values (p > 0.05; Table 2). There was no significant difference in the improvement of ODI, VAS and JOA scores between the two groups (p > 0.05; Table 2).
The ODI, VAS, and JOA scores in both groups.
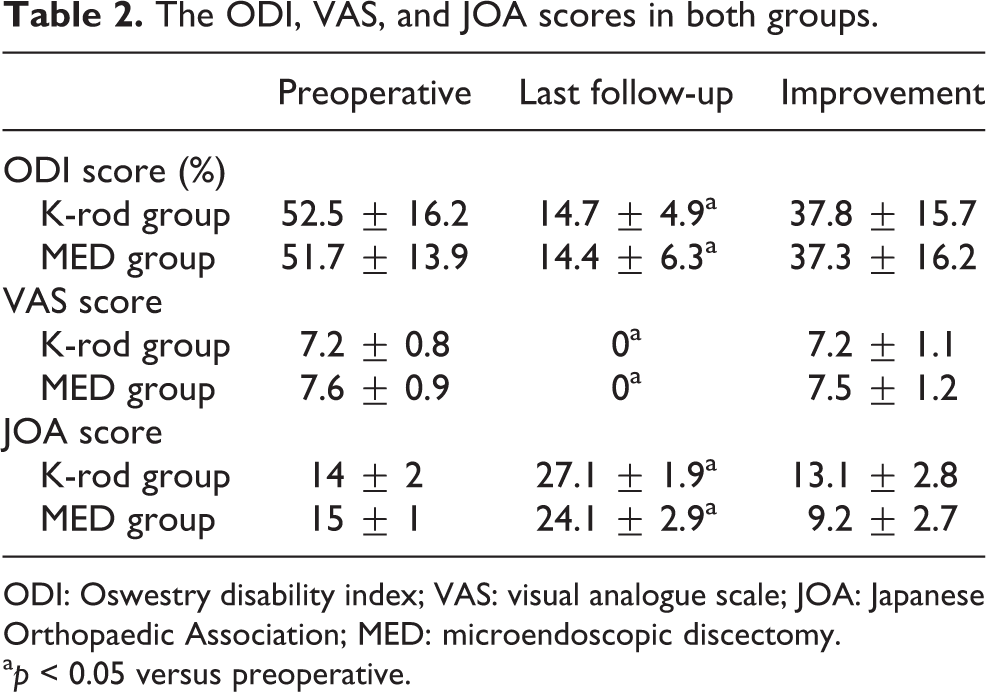
ODI: Oswestry disability index; VAS: visual analogue scale; JOA: Japanese Orthopaedic Association; MED: microendoscopic discectomy.
a p < 0.05 versus preoperative.
At the last follow-up, no broken nails, rods and pedicle screw loosening occurred in any patients. No operation-associated complications and perioperative deaths occurred in either group. No patients had aggravated clinical symptoms or neurological functions.
The preoperative height of intervertebral space was not significantly different between the two groups (p > 0.05; Table 3). At the last follow-up, the height of intervertebral space in the surgical segments was significantly greater in the K-rod group than in the MED group (p < 0.05; Table 3).
The height of intervertebral space in two groups.

MED: microendoscopic discectomy.
aChanges in the height of intervertebral space was calculated as the difference between the height of intervertebral space at last follow-up and preoperative height of intervertebral space.
b p < 0.05 versus K-rod group.
The preoperative Pfirrmann score was not significantly different between the two groups (p > 0.05). Post-operative disc degeneration occurred in 7 (13.0%) of 54 segments in the K-rod group, which was significantly less than that in the MED group (38%, 18/48 segments; p < 0.05; Table 4). In the K-rod group, compared with the preoperative values, at the last follow-up, three proximal segments and four distal segments had one grade change in Pfirrmann grade scores, and no segments had more than one grade change in Pfirrmann grade scores. The Pfirrmann score of the surgical segment did not change before and after surgery. In the MED group, at the last follow-up, five proximal segments and four distal segments had one grade change in Pfirrmann grade scores, and one proximal segment and no distal segments had more than one grade change in Pfirrmann grade scores. Eight surgical segments had one grade change in Pfirrmann grade scores, and no surgical segments had more than one grade change in Pfirrmann grade scores. The disc degeneration occurred more in the MED group than in the K-rod group (p < 0.05; Table 4).
The Pfirrmann grade from MRI.
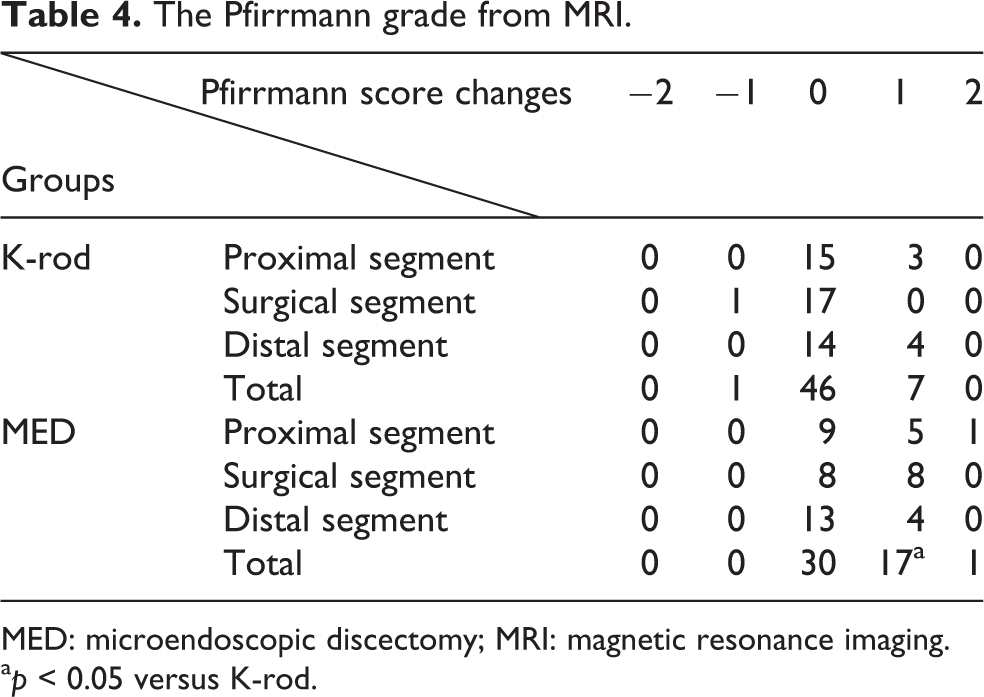
MED: microendoscopic discectomy; MRI: magnetic resonance imaging.
a p < 0.05 versus K-rod.
Discussion
In this study, we investigated the clinical outcomes of patients with single-segment lumbar disc herniation after K-rod dynamic internal fixation or MED. We found that both approaches effectively reduced the pain and improved the neurological function. At the last follow-up, the height of intervertebral space in the surgical segments, proximal segments and distal segments was significantly greater in the K-rod group than in the MED group. In addition, the disc degeneration occurred less in the K-rod group than in the MED group. Our findings suggest that the K-rod fixation is superior to the MED in reducing disc degeneration in the treatment of lumbar disc herniation.
Spinal fusion is commonly required for management of lumbar instability. However, it can be associated with some complications such as adjacent segment degeneration, since spinal fusion shifts of the rotation centre over the disc, thus leading to an increased stress on the disc of the adjacent mobile segments. 16,17 Dynamic stabilization system without fusion, which allows ideal mobility of the vertebra, can reduce the loading on the intervertebral disc and thus improve spinal stability and reduce adjacent segment degeneration. 13,18 In this study, we found that K-rod internal fixation reduced adjacent segment degeneration. The elastic PEEK rod used in this study has an elastic modulus of about 5 GPa, which is more similar to that of the cortical bone (12 GPa) than titanium alloy (110 GPa). 19,20 The approximation of the PEEK rod to the physiological stiffness of the vertebral column may allow column load sharing, thus reducing loading forces of the adjacent segments. In addition, slight mobility of the elastic K-rod during the spinal motion allows the ideal mobility of the intervertebral space, thus reducing the compressive pressure on the intervertebral disc of the adjacent segments.
It has been reported that dynamic stabilization internal fixation can produce a similar spinal stabilization with an improved spinal mobility compared with spinal fusion. 18 In a retrospective study of 39 cases with lumbar disc herniation, Di et al. found that K-rod system preserved lumbar motion, reduced pain symptoms and produced no obvious effects on adjacent segment degeneration. 14 In the present study, we compared the effect of K-rod internal fixation versus MED for the treatment of lumbar disc herniation and found that K-rod produced a similar effect on pain reduction and reduced adjacent segment degeneration compared with MED, suggesting that K-rod may be superior to MED in preventing adjacent segment degeneration in the treatment of lumbar disc herniation. However, Sengupta et al. suggest that dynamic stabilization system should be used for the treatment of early disc degeneration, and fusion should be selected for advanced disc/facet degeneration and gross instability. 21 In addition, although dynamic stabilization system is useful to prevent degenerative disc diseases of lumbar spinal segments in patients with lumbar disc herniation after nucleotomy, it should not be used in patients with obvious vertebral deformation and those required extensive decompression surgery. 22
MED has some advantages such as less surgical trauma, less blood loss and short length of hospital stay. 4 –7 In this study, we found that MED was associated with shorter operation time and less blood loss compared with K-rod internal fixation. However, due to the limited working area, the degenerative disc may not be completely removed during MED, and the remnant tissues may lead to disease recurrence. In addition, MED has been found to be associated with more dural tear, which requires open surgery to repair. 7,9,23 In the present study, we found that although MED and K-rod internal fixation produced similar effect on pain reduction in patients with lumbar disc herniation, MED was associated with more adjacent segment degeneration compared with K-rod internal fixation. Therefore, based on our study, K-rod system can be used in patients with lumbar disc herniation, especially in young patients with concerns about adjacent segment disease following MED.
Our study has some limitations. First, in this study, we used plain radiography to identify the occurrence of screw loosening due to its low cost. Plain radiography is less sensitive to detect screw loosening and thus may miss the detection of the complication in some patients. More sensitive techniques such as CT or low-dose CT should be used in the future study to identify whether there are differences in screw loosening between the two methods for the treatment of single-segment lumbar disc herniation. Second, the sample size of this study is relatively small. Further studies with a large sample are required to confirm the conclusion of our study. Third, the follow-up time is relatively short. A longer follow-up period may better identify the long-term effect of K-rod and MED on adjacent segment degeneration. Future study will be performed to investigate the long-term clinical outcome of K-rod internal fixation in patients with lumbar disc herniation.
Conclusion
We found that K-rod internal fixation and MED produced satisfactory outcome in the treatment of single-segment lumbar disc herniation. We also found that K-rod was associated with less adjacent segment degeneration compared with MED. Our study suggests that K-rod internal fixation is superior to MED in preventing adjacent segment diseases when used in the treatment of single-segment lumbar disc herniation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.