
Abstract
Purpose:
This study is performed to identify risk factors for delirium in osteoporotic hip fractures and to evaluate the hospitalization cost and clinical outcomes of delirium in osteoporotic hip.
Methods:
A total of 221 patients with osteoporotic hip fractures were assessed for eligibility between 2010 and 2014. Among them, 37 patients with delirium were allocated into the delirium group (group D) and 37 patients without delirium were allocated into the non-delirium group (group ND) by matching demographic factors. Risk factors such as time between admission and operation, body mass index, American Society of Anesthesiologists status, cognitive impairment, preoperative urinary catheter, electrolyte imbalance, preoperative hemoglobin, polymedication (medications > 5), pneumonia, anesthesia time, operation time, estimated blood loss, and total amount of transfusion were evaluated for correlation with incidence of delirium. The hospitalization cost was evaluated, and clinical outcomes such as readmission, mortality, and activity level at 1-year follow-up were evaluated.
Results:
In multivariate analysis, polymedication (p = 0.028) and preoperative indwelling urinary catheter insertion status (p = 0.007) were related to the incidence of delirium in patients with osteoporotic hip fractures. Group D showed a significantly higher hospitalization cost compared to group ND. However, delirium did not have a significant effect on length of hospital stay, readmission rate, postoperative 1-year mortality, and activity level.
Conclusions:
Polymedication and preoperative urinary catheter were related to perioperative delirium. In addition, delirium in osteoporotic hip fractures may not have a detrimental effect on clinical outcomes; however, hospitalization cost seemed to be increased due to delirium.
Introduction
Osteoporotic hip fracture is a well-known socioeconomic burden, and it would have grown in number by the year 2040. 1 –5 It accounts for 14% of fractures in the elderly; however, the economic costs were 72% of orthopedic surgery in the elderly. 6 According to the literatures, estimated costs of hip fracture care in the United States may reach 62 billion by 2040. 5,7 It is essential for healthcare providers to reduce the cost of care in osteoporotic hip fractures with respect to the socioeconomic value. Delirium is defined as loss of cognitive function and perception with altered awareness and attention. It is relatively common with an incidence of 10–61% in patients with osteoporotic hip fractures after the surgery. 8 In general, delirium is known as an independent risk factor for higher mortality, morbidity, lower functional outcome, and longer hospital stay with a high economic cost. The control or prevention of delirium might be important for reducing the socioeconomic burden as well as for improving the patient’s personal health and quality of life. 9 Zywiel et al. reported that delirium increased the length of hospital stay and was associated with significant incremental episode-of-care cost. 10 Delirium during acute hospitalization can be prevented and success in preventing delirium might reduce the total cost of hospitalization. 11 Acute hospitalization cost was found to be responsible for 57% of total costs of caring for a hip fracture and it would be important to reduce the hospitalization cost. 6 On the contrary, the preventive intervention for delirium could be overpriced, and the cost-effectiveness might matter. Therefore, it might be helpful to evaluate the risk factors for delirium and consider the risk factors from the economic viewpoint. There has been little study on delirium in osteoporotic hip fractures with respect to the economic cost during acute hospitalization. We do not know which risk factors related to the incidence of delirium are really preventable and whether the intervention for prevention is helpful in lowering the cost of care in osteoporotic hip fractures or not. Therefore, it might be reasonable to evaluate the risk factors by matched analysis with uncontrollable factors, for example, age, gender, fracture type, operation method, and body mass index (BMI). We hypothesized that delirium may negatively affect the cost of hospitalization in patients with osteoporotic hip fractures and there may be some risk factors related to the incidence of delirium and also correlated with hospitalization cost. The aim of this study was to identify risk factors for delirium in osteoporotic hip fractures that affect the cost and to compare the hospitalization cost and clinical outcomes between patients who had osteoporotic hip fractures with delirium and without delirium by the age, gender, fracture type, operation method, and BMI-matched analysis.
Materials and methods
We received the institutional review board approval of the author’s institution.
Subject enrollment
A total of 221 patients over 65 years of age and diagnosed as having femoral neck fracture or intertrochanteric hip fracture by International Classification of Diseases (ICD-9) at the authors’ institution between January 2010 and February 2014 were assessed for eligibility. We excluded the patients who were lost to follow-up (n = 18), patients with high-energy injuries (n = 2), patients who refused to undergo surgery (n = 4), and patients who received revision hip surgery (n = 3). None of the patients had a history of pathologic fracture and infection. None of the patient was diagnosed as delirium at the time of admission. We defined high-energy injury as an injury caused by traffic accident (n = 1) and fall from a height of more than 1 m (n = 1). The remaining 194 patients were allocated into two groups, which were the osteoporotic hip fracture with delirium (group D, n = 37) and without delirium (group ND, n = 37) groups, by matching the age, gender, fracture type, operation method, and BMI (Figure 1).

The flowchart of subject enrollment.
Fracture type and operation methods
All operations were performed by a single surgeon. Twenty-four femoral neck fractures were treated by bipolar hemiarthroplasty (EcoFit® system; Implantcast, Buxtehude, Germany), 48 intertrochanteric fractures were treated with closed reduction and internal fixation with gamma nails (The Gamma 3 Locking Nail System®, Stryker, MI, USA), and the remaining two intertrochanteric fractures were treated by bipolar hemiarthroplasty.
Diagnosis and treatment of delirium
Delirium was detected by the nurses and orthopedic residents with the short version of Confusion Assessment Method (CAM) tool. The short version of CAM is composed of four features: (1) acute onset and fluctuating course; (2) inattention; (3) disorganized thinking; and (4) altered level of consciousness. Features (1) and (2) should be present with a combination of either (3) or (4) to diagnose delirium. Confirmation of the diagnosis was performed by the consultant psychiatrist, and quetiapine fumarate (Seroquel®; Astrazeneca UK, 25 mg to 50 mg once at bedtime) was administered as the first drug of choice at the author’s institution and it was administered until discharge. Additionally, all the patients with delirium were provided other treatments, such as environmental modification, cognitive-emotional support, and education for the family.
Assessment of preoperative risk factors
We assessed the time between admission and operation, American Society of Anesthesiologists (ASA) physical status, cognitive impairment, insertion of indwelling urinary catheter, polymedication (medication > 5), electrolyte imbalance, preinjury Koval’s grade, 12 and preoperative hemoglobin. Cognitive impairment was diagnosed by the mini-mental state examination (range, 0–30: 24–30, no cognitive impairment; 18–23, mild cognitive impairment; 0–17, severe cognitive impairment) at admission.
Assessment of intraoperative and postoperative risk factors
We assessed the anesthesia method (general or spinal anesthesia), operation time, anesthesia time, estimated blood loss (EBL), the amount of transfusion, and perioperative pneumonia. EBL was assessed by the following calculation: VI = EBv × (Ho − Hf)/2 (VI = EBL, EBv = estimated blood volume, Ho = preoperative PCV, Hf = postoperative PCV, and PCV = pack cell volume). 13
Follow-up and outcome evaluation
The patients were routinely followed up at a 6-month interval until 1 year after the operation, and then 1-year interval follow-up was performed. The hospitalization cost, length of hospital stay, mortality rate at 1 year postoperatively, readmission due to morbidity, and Koval’s grade at 1 year were evaluated. The hospitalization cost included the cost of infrastructure, medications, materials, instruments, fees of the surgeon, anesthesiologist, consulting physician, and so on. The hospitalization cost was converted from Won (Korean Currency) to US dollars by applying the mean exchange rate in June 2015. Koval’s grade represents the activity of patients, and patients were classified as independent community ambulatory (I), community ambulatory with cane (II), community ambulatory with walker or crutches (III), independent household ambulatory (IV), household ambulatory with cane (V), household ambulatory with walker or crutches (VI), and nonfunctional ambulatory (VII). They were also simply classified into ambulatory outdoors (I–III) or shut-in patients (IV–VII) for clarifying comparative analysis of follow-up studies.
Statistical evaluation
Student’s t-test was used to evaluate differences between the groups for continuous variables and the χ 2 or Fisher’s exact test was used for the comparison of categorical variables. Multivariate regression analysis was performed to evaluate the risk factors for delirium. SPSS 18.0 (SPSS, Inc., Chicago, IL, USA) was used for statistical analysis, and p < 0.05 was considered to indicate statistical significance.
Results
The demographic data of patients are summarized in Table 1. The mean age of the cohort was 81.4 ± 6.7 years (27 males and 47 females). Perioperative delirium occurred at mean postoperative 0.97 ± 2.5 days (range, preoperative 4 days to postoperative 10 days). In multivariate regression analysis with risk factors, polymedication (p = 0.028, OR [Odd ratio] = 3.401, and 95% CI [Confidence Interval] = 0.998 − 11.589) and preoperative indwelling urinary catheter insertion status (p = 0.007, OR = 4.898, and 95% CI = 1.548 − 15.500) were related to the incidence of delirium in patients with osteoporotic hip fractures (Table 2). Overall length of hospital stay in this study was mean 18.3 ± 10.6 days, and no significant difference was observed between groups D and ND (Table 3). Readmission due to morbidity occurred in 16 of 74 (21.6%) patients. Morbidities that resulted in readmission in group D were pneumonia in three cases, septicemia in two cases, cardiovascular events in two cases, cerebrovascular events in two cases, vestibular neuritis in one case, and diabetic ketoacidosis in one case. Morbidities related to readmission in group ND were pneumonia in two cases, gastric ulcer in one case, cardiovascular event in one case, and common bile duct stone in one case. The overall hospitalization cost was mean US$6973.4 (range, US$3924–US$17,222), and group D showed a significantly higher hospitalization cost compared to group ND (US$7736.55 ± US$2947.73 vs. US$6333.97 ± US$1698.24, p = 0.017). Among the risk factors evaluated, operation time (p = 0.005 and k = 0.494) and anesthesia time (p = 0.019 and k = 0.419) were related to the hospitalization cost. The mortality rate at 1 year postoperatively was 17.5% (13 of 74 patients). The mortality rate at 1 year postoperatively in group D (9 of 37 patients) was twice as high as that in group ND (4 of 37 patients), but there was no significant difference between groups D and ND. The readmission rate in group D (11 of 37 patients) was also twice as high as that in group ND (5 of 37 patients), but there was no significant difference between groups D and ND (Table 3). No significant differences were observed between groups D and ND with respect to the decrease in activity at the 1-year follow-up, which was evaluated by Koval’s grade (Figure 2). According to the binary classification of the activity level into ambulatory outdoors and housebound, there was no significant difference between groups D and ND with respect to change in the activity level at the postoperative 1-year follow-up (Table 4).
Demographic data of groups D and ND.a

CRIF: closed reduction and internal fixation with gamma nail; BPHA: bipolar hemiarthroplasty; BMI: body mass index; SD: standard deviation.
aAge, gender, fracture type, and operation method were matched between the two groups in this study.
bGroup of patients who had fragility hip fractures with delirium.
cGroup of patients who had fragility hip fractures without delirium.
Risk factors (delay in operation: admission to surgery and trauma to surgery).
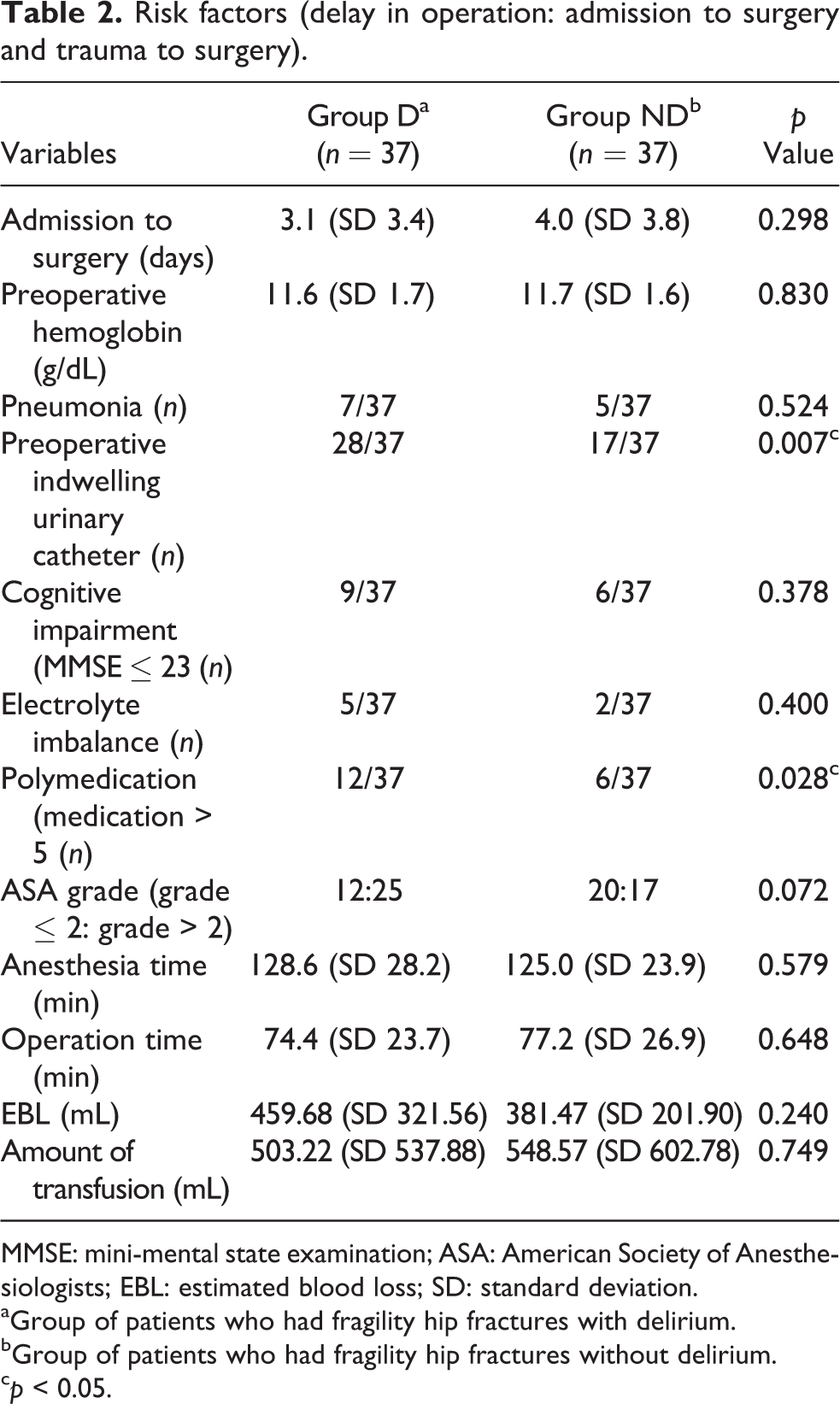
MMSE: mini-mental state examination; ASA: American Society of Anesthesiologists; EBL: estimated blood loss; SD: standard deviation.
aGroup of patients who had fragility hip fractures with delirium.
bGroup of patients who had fragility hip fractures without delirium.
c p < 0.05.
Comparisons of outcomes between groups D and ND.

SD: standard deviation.
aGroup of patients who had fragility hip fractures with delirium.
bGroup of patients who had fragility hip fractures without delirium.
c p < 0.05.
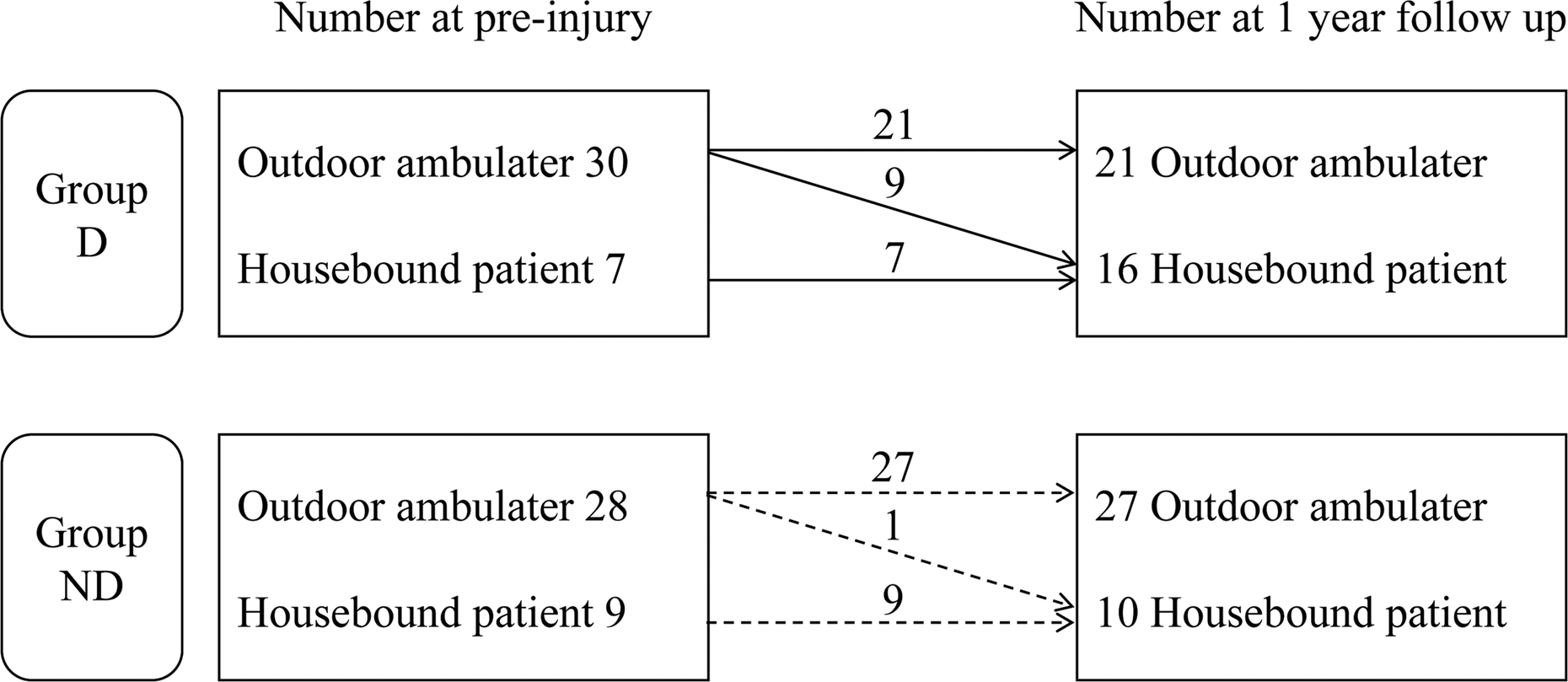
The changes in activity level in groups D and ND at the 1-year follow-up (p = 0.239).
Changes in the activity level (Koval’s grade).

aGroup of patients who had fragility hip fractures with delirium.
bGroup of patients who had fragility hip fractures without delirium.
Discussion
Evaluation of the economic cost during the management of osteoporotic hip fractures considering outcomes such as the length of stay, hospitalization cost, and readmission rate has been performed by several authors. 14 –18 The healthcare cost of osteoporotic hip fractures has been increasing rapidly and the hospitalization cost seems to account for a large portion of the total sum of healthcare cost in osteoporotic hip fractures. The poor general health condition of patients with osteoporotic hip fractures was found to be related to high mortality and morbidity as well as high economic cost. Delirium is a relatively common disease occurring in elderly patients and it is also known to represent the inadvertent outcomes. 19 –21 However, evaluation of the economic cost of delirium has not been sufficiently studied and the possible risk factors related to delirium were not evaluated previously.
We hypothesized that delirium might increase the length of hospital stay, hospitalization cost, readmission rate due to morbidity, mortality, and compromise of activity after operation. Furthermore, there may be some risk factors related to the incidence of delirium.
Patients who received five or more medications had 3.4 times higher risk of delirium than patients who received four or less medications, and patients with an indwelling urinary catheter before surgery had 4.9 times higher risk of delirium than patients without a preoperative indwelling urinary catheter. Approximately, US$1400 more were spent for hospitalization cost in patients with delirium than in patients without delirium. However, the reduction of hospitalization cost might not be accomplished by the management of risk factors related to delirium in osteoporotic hip fractures because polymedication and preoperative indwelling urinary catheter status were related to the general health condition that could not be controlled. In patients with delirium, the economic cost was related to the operation time and anesthesia time. The operation time and anesthesia time were related to the economic cost in general. Readmission rate, mortality rate at postoperative 1 year, and decrease in the activity level were not affected by delirium. Length of hospitalization was not significantly increased in patients with delirium.
The causes of postoperative cognitive problems have not been clearly elucidated. 22 Advanced age, history of cognitive impairment, alcohol abuse, preoperative medication, urinary retention, anesthetic agent during operation, and electrolyte imbalance are the well-known risk factors for postoperative delirium. 23 –25 We also found that polymedication (medication > 5) and preoperative indwelling urinary catheter insertion status were risk factors for delirium with matched analysis. Polymedication represents poorer preoperative physical condition and multiple comorbidities. It might indicate that poorer general physical condition is related to delirium. Most of the patients who received polymedication in our study were suffering from diabetes and hypertension. Some authors say that the vascular risk factors increase postoperative delirium. It might be attributed to intracerebral atherosclerosis, which causes hypo-oxygenated brain and postoperative delirium. 26,27 Postoperative delirium often occurs because of pain, stress, and anxiety. Indwelling urinary catheter can cause feeling of urination and it can be stress to patients. This stressful condition might cause delirium. 28 It is well-known that there are multifactorial causes of delirium; however, the control or prevention of delirium may not be accomplished perfectly because the incidence of delirium was mainly affected by the patient’s individual general health condition. Kates et al. emphasized that a high-quality care program can reduce the cost of osteoporotic hip fractures, and early intervention and lowering the drug cost seemed to be effective. 17 The economic cost study with propensity score matching revealed that delirium was related to the length of hospital stay, cost of delirium care, and demands of aftercare since the discharge. 10 In our study also, we found that the operation time and anesthesia time were factors related to hospitalization cost and no direct patient-related factors were found to be related to the cost except for delirium in our study. We did not perform a detailed analysis of cost between groups D and ND; however, we assumed that poor general health condition which is responsible for delirium might increase the hospitalization cost due to delay in recovery after the operation. The length of hospital stay, clinical outcome, and readmission rate were not related to delirium, and this result was contrary to previous results. 10,29 –32
We hypothesized that delirium may be associated with poor clinical outcomes, such as poor functional status, residual pain, and several comorbidities. Unexpectedly, there is no significant difference in clinical outcomes, which was evaluated by Koval’s grade. We suggested that delirium is temporary mental alteration status, which not leave behind sequelae. So, there was a little influence in long-term follow-up studies.
The current study was an age, gender, fracture type, operation method, and BMI-matched analysis, and such a study has never been attempted previously. We tried to identify the risk factors related to medical problems rather than demographic characteristics which were already determined. Therefore, the results of risk factors related to delirium in this study might be different from those in previous studies. This was the first study to perform delirium-related economic cost analysis in Korea. Furthermore, the current study may suggest that delirium in osteoporotic hip fractures could be the leading cause of hospitalization cost increase and this should be prudently considered in the bundled payment system.
This study has several limitations. First, the number of the subjects included in this study was relatively small and statistical power evaluation was not performed. There was no significant difference between groups D and ND with respect to the postoperative 1-year mortality rate and readmission. But the lack of significance may depend on relatively small number of the subjects. Second, the retrospective nature of this study may have caused selection bias and other confounding factors may not have been regulated adequately, which could have distorted the results. Third, we did not evaluate the duration of delirium, and when the symptom persisted longer, the results could be worse.
In conclusion, the risk factors for delirium were history of polymedication administration and preoperative indwelling urinary catheterization, and this finding could be interpreted as the poor general health condition in patients with osteoporotic hip fractures was the main cause of delirium. Delirium may not have a detrimental effect on clinical outcomes; however, the hospitalization cost was increased in patients with delirium compared to patients without delirium.
Conclusions
Delirium in osteoporotic hip fractures may not have a detrimental effect on clinical outcomes. However, the hospitalization cost seemed to increase due to delirium. In addition, polymedication and preoperative urinary catheter were related to perioperative delirium. Therefore, it is recommended extra attention to patients with underlying diseases or urinary difficulty be paid after operation as they are considered vulnerable to delirium.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.