
Abstract
Purpose:
To determine the prevalence of complementary and alternative medicine (CAM) use in patients with low back pain (LBP) and to identify its correlation with demographic factors, clinical condition and psychosocial factors.
Methods:
A cross-sectional study was conducted with 278 LBP patients. Use of CAM, demographic parameters and disease duration were determined. Self-reported health status and self-rated scales assessed the effect of disease on quality of life and emotional well-being, respectively. Satisfaction with orthopaedic care and belief partiality towards CAM were assessed.
Results:
In all, 72.3% patients sought CAM treatment. The most common choice of CAM was traditional Chinese medicine (TCM; n = 166), followed by massage therapy (n = 114) and chiropractic treatment (n = 45). Within TCM, acupuncture was the most popular treatment for LBP (n = 127). Only 32.5% patients informed their doctors of their CAM use. In univariate analyses, factors positively associated with CAM use included duration of LBP (odds ratio (OR) = 1.45, 95% confidence interval (CI): 1.06–1.97), use of CAM in close social circles (OR = 1.98, 95% CI: 1.15–3.43) and summary score for belief partiality towards CAM (OR = 1.18, 95% CI: 1.13–1.23). Variables negatively and significantly associated with status of CAM use include age (OR = 0.97, 95% CI: 0.95–0.99) and summary score for satisfaction with orthopaedic care (OR = 0.93, 95% CI: 0.88–0.99).
Conclusion:
CAM use in patients with LBP is prevalent and largely unknown to their doctors. Personal beliefs and their satisfaction with conventional medical treatment both play a part in their decisions to use CAM. Future studies may aim at understanding the effect of CAM on patient adherence to conventional medical treatment and patients’ perception of well-being and pain.
Introduction
Low back pain (LBP) is a disease with significant burden worldwide. In the World Health Organization (WHO) Global Burden of Disease 2010 study, LBP was ranked first in terms of Years Living with Disability (YLD). 1 With the ageing population, prevalence and burden of LBP is expected to rise and this is a phenomenon across different countries. 2 In the United States, the prevalence of LBP has risen significantly over the past two decades. 3 LBP is a major cause of disability and healthcare utilization, which imposes direct costs to the medical system, lowers labour productivity and increases economic burden. 4 In the United Kingdom, more than 100 million workdays are lost per year due to LBP. 4 Studies also pointed out that the prevalence of LBP is not only limited to developed countries but also observed in developing countries in Africa. 5 The ubiquitous nature of LBP in populations around the world showed that it is not a regional issue but a global problem.
Patients suffering from chronic diseases often turn to complementary and alternative medicine (CAM), either as supplementary to or in lieu of conventional medical treatments. 6 CAM commonly refers to any therapy that does not fall into the category of conventional medical treatment and represents a large and heterogeneous group of treatments formed by diverse health ideologies and beliefs. The National Centre for Complementary and Integrative Health gives a formal definition of CAM as ‘a group of diverse medical and healthcare systems, practices, and products that are not generally considered part of conventional medicine’. 7 Examples of CAM are traditional Chinese medicine (TCM), naturopathy, chiropractic medicine, acupuncture, herbal supplements, chiropractic manipulation and massage. It is generally believed that the use of CAM has been increasing in developing countries. According to a nationwide survey in the United States by Eisenberg et al., 8 the use of CAM (at least 1 of 16) has been increasing from 33% in 1990 to 42% in 1997. Moreover, the frequency of visiting an alternative therapy practitioner and the amount of expenditure on CAM spent by the US population is also escalating. 8 A more comprehensive review of the use of CAM by Harris and Rees 9 covered 50 surveys in 15 countries from 1998 onwards and showed strong evidence of substantial CAM use in these countries including the United Kingdom and Australia. Other studies in Europe and the United States support a prevalent use of CAM in the West. 10 –12
In addition to studies and surveys in Europe and America, several groups studied CAM use in Asian countries, including Japan, Singapore and Hong Kong. 13 –16 Lee et al. 14 showed a 1-year prevalence of 22% of CAM use among primary care patients in Singapore. One of their key findings was that CAM use was strongly associated with the ‘chronic disease triad’ of arthritis, musculoskeletal disorders and stroke, and that the use of CAM by patients was often not disclosed to their doctors, a result consistent with the findings in Australia and Italy. 11,17 The evidence above is substantial regarding the use of CAM as a prevalent, global trend on the rise in recent years. However, the reasons behind the choices of CAM use remain complicated by the heterogeneity of illnesses treated, with large variability of treatments, and cultural and demographic differences between populations.
In Hong Kong, while there are no recent data on the prevalence of LBP, its prevalence is expected to be on the rise in the near future, given a rapidly ageing population. Due to the global trend of high CAM use, it is also believed that the majority of the LBP population will turn to CAM. In Hong Kong, no previous data are available on the use of CAM for LBP in patients. However, earlier studies explored the health beliefs and attitudes of Hong Kong Chinese regarding TCM, the most popular CAM of choice in Hong Kong. 16,18 A qualitative study by Lam 18 showed that many patients in Hong Kong used TCM and conventional medicine concurrently and considered conventional medicine have more side effects on their bodies. Due to their ethnic and cultural background, patients in Hong Kong may have very different health concepts than patients in Western countries. It is suggested that conventional medical professionals should be aware of this situation when interacting with these patients in order to build a good patient–doctor relationship. Additionally, Xue et al. 19 conducted a study on personal use of CAM among registered nurses in Hong Kong and found that 80% had used at least one form of CAM, and over 40% would recommend it to their patients.
Given the vacuum of information regarding CAM use in patients with LBP in Hong Kong, it is necessary to determine the prevalence of CAM use in patients currently receiving conventional medical treatment for LBP and explore possible factors that influence the use of CAM treatment in this population.
Materials and methods
Study design
A cross-sectional study was performed of consecutive subjects recruited from a tertiary spine orthopaedic clinic (SOPC) in Hong Kong, between September 2016 and February 2017. This clinic was run on a weekly basis seen by orthopaedic surgeons, covering over 1 million individuals in the region. Patients must be referred by primary care clinicians in either the public or private sector to attend this clinic. Eligibility criteria included patients over 18 years of age and who were followed up at the clinic for LBP. Exclusion criteria were newly referred patients without a proper clinical diagnosis or patients who were unable to understand or comply with the study. Ethics approval was obtained by the local institutional review board. Informed consent was obtained prior to the interview. The study response rate was 76%, resulting in a total of 278 patients consenting for interview.
Questionnaire
To determine CAM use, a 10-min questionnaire (Online Appendix) was either administered by the interviewer for the illiterate or self-administered. The questionnaire comprised four sections: (1) demographics, (2) clinical information, (3) CAM use and (4) satisfaction with care and belief partiality. A subject was considered to be a CAM user if the subject sought CAM treatment specifically for LBP since diagnosis. The questionnaire was first piloted for 18 additional patients not included in the final analysis. The questionnaire was then modified for clarity and the length shortened before administered to the 278 study participants.
Parameters under study
Demographic factors explored were age, sex, education level (primary school or below, secondary school and tertiary education or above), socioeconomic status and religious belief. Type of housing (public housing, Home Ownership Scheme flats, private rental, private ownership, shoebox unit, institution, no permanent housing) was used as a surrogate for socioeconomic status.
Clinical information included self-reported health status, duration of LBP (under 6 weeks, 6 weeks to under 3 months, 3 months to under 1 year, 1 year to under 3 years, 3 years or above), self-rated illness impact on quality of life, self-rated illness impact on emotional well-being, and whether conventional medical treatment was the first treatment sought. Single-item questions on self-reported health status (‘In general, would you say that your health is “very poor”, “poor”, “fair”, “good” or “excellent”’?) was used to assess impact of chronic illness, as documented in the SF-36 Health Survey scale and used in previous studies on CAM use. 14,20 Illness impact on quality of life and emotional well-being were each self-assessed on a scale of 1 to 10.
A list of 21 common CAM treatments were provided for LBP, and subjects were given the option of adding other CAM types that they are using. TCM is an umbrella term for a variety of treatments administered by different types of providers, and TCM is further divided into prescribed herbal medicine, herbal medicine in finished dose, acupuncture, bone setting and cupping therapy. Influence on the patient’s use of CAM by close social circle was evaluated by a question on whether family, relatives or friends used or recommended CAM. For subjects who have used CAM, three questions were asked to explore the source of information on CAM, whether the attending doctor was informed of their CAM use, and the chief reason for not informing the attending doctor of their CAM use.
The patient’s satisfaction with care was evaluated by a questionnaire scale of 10, with a total of 12 items. Six items were in the domain of ‘satisfaction with orthopaedic care’ (waiting time, consultation time, perceived benefits from treatment, personalized view of patient, doctor empathy and trust in doctor; 1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, 5 = very satisfied), and seven items were in the domain of ‘belief partiality towards CAM’ (perceived benefit of CAM use, perceived benefit of CAM as a supplement to conventional medical treatment, convenience, cost, belief in curative effect of CAM, better suitability with personal needs and fewer side effects). Items used in assessment of satisfaction with orthopaedic care were decided upon following literature search for care quality assessment. 14 Items used in assessment of belief partiality towards CAM were drawn in part from a qualitative study 18 that showed Chinese CAM users often believe TCM is curative, has side effects and can serve as an alternative when conventional medical treatment fails. 18 The scores for satisfaction with orthopaedic care and belief partiality towards CAM were calculated by summing all items in each domain, respectively.
Statistical analysis
Outcome measure used for statistical analysis was any CAM use since the initial clinic visit. Binary logistic regression was performed with point estimates of odds ratio (OR) of association and 95% confidence intervals (CIs) in univariate analyses. Independent variables included age, sex, type of housing (as surrogate of socio-economic status), self-reported health status, duration of LBP, self-rated impact of LBP on quality of life, self-rated impact of LBP on mental health, whether conventional medical treatment was sought as a first-line treatment for LBP, types of conventional medical treatment treatments received under orthopaedic care, use of CAM in close social circle, satisfaction with orthopaedic care and belief partiality towards CAM. All statistical analyses were performed using SPSS version 24.
Results
Patient demographics
Table 1 lists patient demographics. The median age of the 278 patients interviewed was 63.5 years, and 69.4% were female. A total of 64.7% of patients attended secondary school or above, and 42.2% lived in privately owned house. Up to 59% of patients had no religious beliefs. With regard to clinical information, 62.5% of patients had a self-reported health status of fair or above, and 67.6% had LBP for more than 3 years. The median self-rated disease impact on quality of life and on mental well-being was both 7 out of 10. In all, 76.6% patients sought conventional medical treatment as the first-line treatment for their LBP, and a large proportion (59.4%) had received oral medication together with physiotherapy and/or occupational therapy as part of their treatment under orthopaedic care.
Patient demographics.
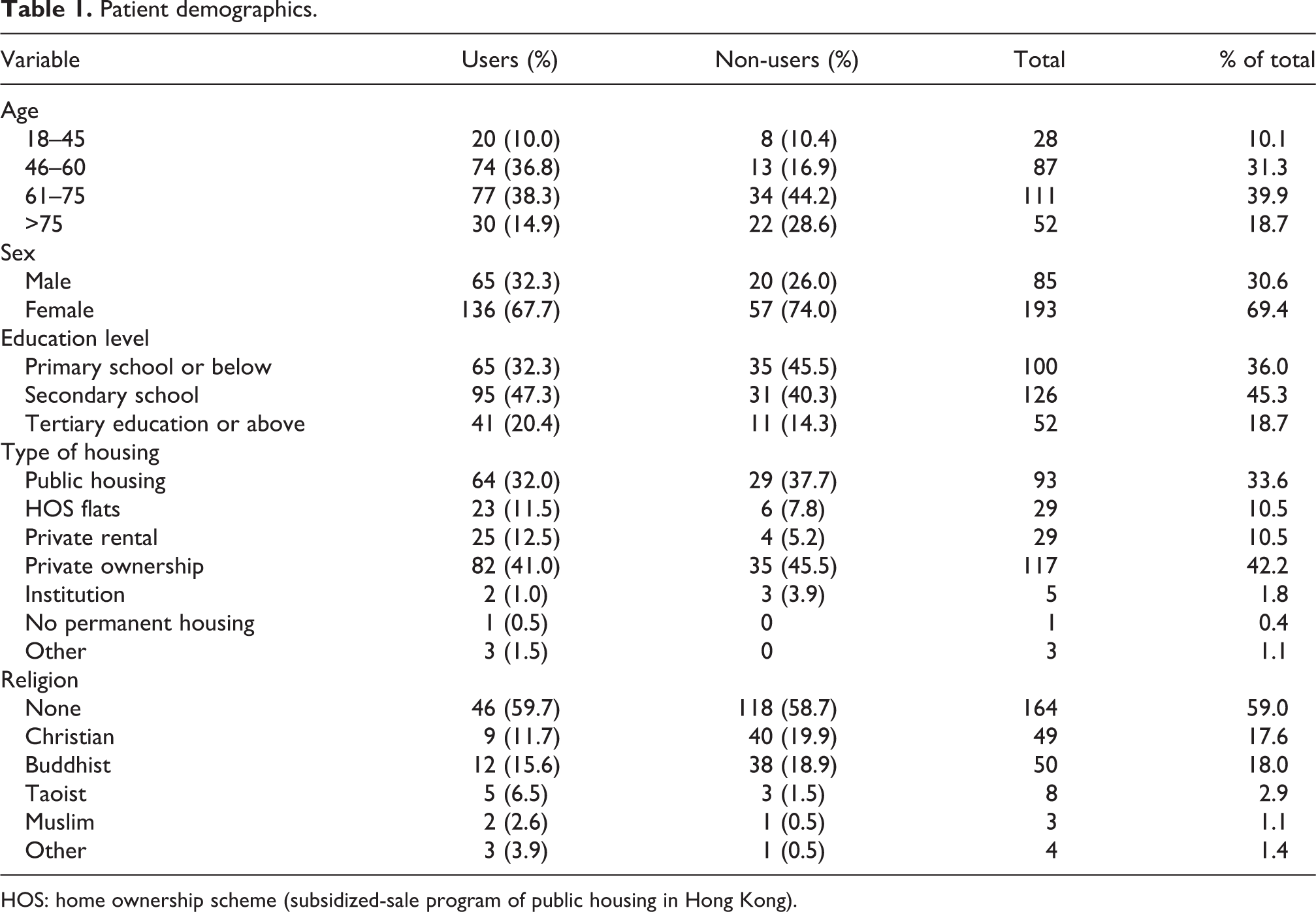
HOS: home ownership scheme (subsidized-sale program of public housing in Hong Kong).
Prevalence
The prevalence of CAM use in patients already receiving Western medical care was 72.3%. For those who used CAM, 76.1% used more than one type of CAM. As shown in Figure 1, the most common CAMs used were TCM (n = 166, prevalence = 59.7%), massage therapy (n = 114, prevalence = 41.0%) and chiropractic treatment (n = 45, prevalence = 16.2%). The most popular TCM treatments were acupuncture (n = 127, prevalence = 45.7%), bone setting (n = 72, prevalence = 25.9%) and cupping therapy (n = 66, prevalence = 23.7%; Figure 2). For those who used CAM, the most common sources of information regarding CAM treatments were from friends and colleagues (60.4%), followed by CAM practitioners (21.9%) and family members (21.9%; Figure 3). Only a proportion of patients (32.5%) informed their attending doctors of their CAM use, and the most common reason for not informing the doctor was that the doctor did not bring up the topic during consultation (79.3%), as shown in Figure 4.

Frequency of types of CAM. CAM: complementary and alternative medicine.

Frequency of types of TCM. TCM: traditional Chinese medicine.

Frequency of sources of CAM information. CAM: complementary and alternative medicine.

Reasons for not informing orthopaedic surgeons of CAM use. CAM: complementary and alternative medicine.
Correlates of CAM use
Variables found to be significantly associated with CAM use in univariate analyses of the binary outcome are listed in Tables 2 and 3. Several variables showed significant association with CAM use, including Buddhist beliefs (OR = 13.33, 95% CI 1.24–143.47), duration of LBP (OR = 1.45, 95% CI 1.06–1.97), use of CAM in a close social circle (OR = 1.98, 95% CI 1.15–3.43) and summary score for belief partiality towards CAM (OR = 1.18, 95% CI 1.13–1.23). Three items in the domain of belief partiality towards CAM use was in particular significantly associated with CAM use: perceived benefit of CAM as a supplement to conventional medical treatment (OR 1.46, 95% CI 1.01–2.10), ‘better suitability with personal needs’ (OR 1.91, 95% CI 1.13–3.22) and ‘fewer side effects’ (OR 1.48, 95% CI 1.05–2.10). Variables negatively and significantly associated with status of CAM use included age (OR = 0.97, 95% CI 0.95–0.99) and summary score for satisfaction with orthopaedic care (OR = 0.93, 95% CI 0.88–0.99).
Categorical variables significantly associated with status of CAM use in univariate analysis.
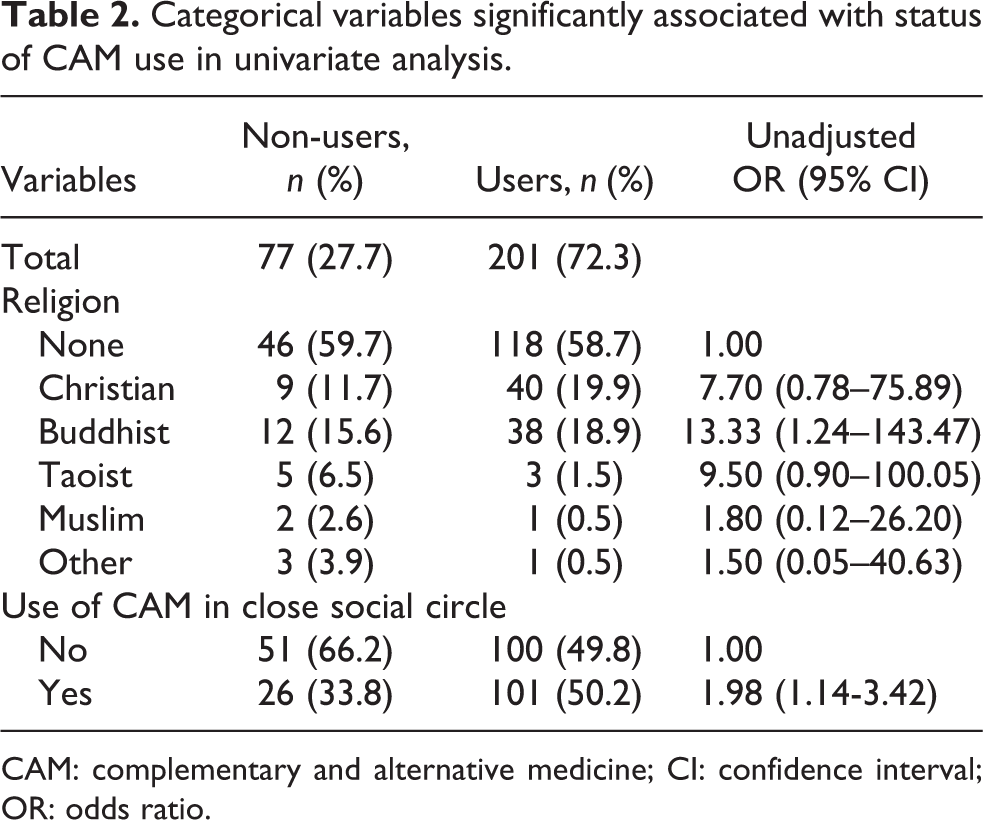
CAM: complementary and alternative medicine; CI: confidence interval; OR: odds ratio.
Non-categorical variables significantly associated with status of CAM use in univariate analysis.

B: unstandardized coefficient; CAM: complementary and alternative medicine; CI: confidence interval; df: degrees of freedom; LBP: low back pain; SE: standard error; OR: odds ratio.
It was worth noting that education level, overall health status and perceived impact of illness on quality of life and emotional well-being failed to show significant associations with CAM use in the univariate analyses.
Discussion
Our results showed that 72.3% of patients with LBP who presented to a public spine tertiary referral clinic for LBP would seek CAM treatments despite continued follow-up, and up to 77% seek active first-line treatment with Western medicine including drugs and physiotherapy. There are no previous reports on prevalence of CAM use for patients followed up at a public clinic for LBP in Hong Kong, and reported estimates of prevalence of CAM use around the world vary greatly depending on population, types of CAM and time period defined for prevalence. However, the rates of use reported here are even more than the 2012 average household survey (42% general use) conducted by the Census and Statistics Department of the Government of Hong Kong Special Administrative Region. The public sector accounts for the great majority of specialist care in Hong Kong. Public hospitals in Hong Kong are district based, though cross-district attendances are not uncommon. While no significant association was found between socioeconomic class and CAM use, it is possible that varying socioeconomic demographics and availability of CAM services in the area may limit the generalization of our results to all patients with LBP, in Hong Kong.
As expected given the large Chinese population in Hong Kong, TCM was found to be the most popular CAM type used by LBP patients in our study. However, TCM is an umbrella term for a variety of treatments delivered by a wide variety of regulated and unregulated providers, we categorized TCM into specific treatments. Acupuncture was found to be the most popular TCM treatment among our LBP patient group, which may be due to the expanding group of conventional medical professionals and CAM practitioners providing acupuncture services, in view of international guidelines to use acupuncture for LBP. 21 We found that a large proportion of patients (67.5%) neglect to inform their doctors of their CAM use, which is consistent with the findings in other studies in Singapore, Australia and Italy. 11,14,17
In our study, age was found to be inversely related to CAM use. Previous studies in Singapore and in Western countries have found higher prevalence of CAM use in the middle-aged populations. It is important to note that the median age of the population sampled was 63.5 years. Old age may prevent CAM use due to factors such as concurrent dementia, loss of independent living and mobility restrictions. As expected, CAM use was found to be positively associated with belief partiality towards CAM, and in particular to the ideas that CAM could provide supplemental benefit to ongoing conventional medical treatment, had fewer side effects and was better personalized to the individual.
Multiple studies attempted to shed light on the reason why people may prefer to use CAM to alleviate LBP. 6,22 –24 Kanodia et al. 25 evaluated the perceived benefits of CAM use in an attempt to understand the motivation for CAM treatment in patients with back pain. Results showed that around 60% of their respondents perceived a great deal of benefits with CAM use, although the specific factors and therapies associated with these kinds of benefits are still unknown. These findings are fairly consistent with earlier studies by Wolsko et al. 26 Ghildayal et al. 27 used a multiple logistic regression approach to evaluate functional status as a predictor of CAM use in a US population of LBP patients. This was fairly consistent with Gaul et al. 28 who conducted two questionnaire-based surveys in Germany and Austria to analyse the attitudes of LBP and headache patients towards CAM use and reported that a majority of the LBP population used CAM and perceived a great deal of benefits.
It has been suggested previously that dissatisfaction with Western medical treatment may push patients to seek CAM care. 6,14 We found a significant negative association between satisfaction with orthopaedic care and CAM use. Our measure of satisfaction score covered both the doctor–patient relationship and the clinical setting of public orthopaedic SOPCs, but no significant associations were found with specific inadequacies of orthopaedic care that influenced CAM use. Hence, the ability of doctors to perform psychotherapy or simply counselling may be the defining factor for adherence to Western medicine or satisfaction of care.
The WHO estimated the 1-year prevalence of LBP as 15–45%, with an adult incidence of 5% per year. 29 Our study only included a relatively small sample size of 278, and future studies should aim to expand both sample population size and selection locations to include more public SOPCs in different districts of Hong Kong. Further studies can stratify patient population by diagnosis, though it must be warned that patients with LBP often have nonspecific causes requiring diagnosis by exclusion and a protracted period of investigations. Factors that may warrant further exploration in the future include whether the unregulated status of many CAM practitioners affect CAM use in patients, previous use of CAM for other medical problems and any effect of CAM use on adherence to Western medical treatment.
Conclusion
In Hong Kong, CAM use by patients with LBP is highly prevalent, which largely remained unknown to their orthopaedic doctors. TCM was the most popular CAM type, and acupuncture was the most prevalent TCM of choice. CAM use was positively predicted by duration of LBP, use of CAM in close social circles, belief partiality towards CAM and low satisfaction with orthopaedic care. Due to the rising trend of CAM use in the general population, it is prudent to further examine its role in clinical care and its effect on adherence to conventional medical treatment.
Footnotes
Authors’ note
This was a medical student-led Health Research Project during 2016–2017, a program initiated by the School of Public Health at the University of Hong Kong.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplementary material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.