
Abstract
Purpose:
This study aimed to present radiologic analysis of minimal safe distance (MSD) and optimal screw angle (OSA) that enables to fix screws in a lateral mass safely without facet joint violation in open-door laminoplasty using a plate.
Methods:
A retrospective analysis was made of 22 patients (male: 17; female: 5), average age 62 years. Seventy-nine lateral mass screws were fixed among a total of 158 screws. MSD that doesn’t allow 5-mm screws to violate a facet joint was measured for C3–C7 and a comparative analysis was performed. If the MSD is not secured, the OSA to be given to the cephalad direction is calculated to avoid violation of the facet joint.
Results:
The screws violating inferior facet joints accounted for 34.1% of the screws fixed in inferior lateral mass. Joint surface to distal mini-screw distances were 3.18 ± 1.46 mm and 4.75 ± 1.71 mm in groups of facet joint violation and non-facet violation (FV), respectively (p = 0.001). When 5-mm screws were inserted into a lateral mass, MSD was 4.39 ± 0.83 mm. The average MSD of C3, C4, and C5 was 4.05 ± 0.78 mm, 4.10 ± 0.70 mm, and 4.26 ± 0.74 mm, respectively. There was no significant differences among levels (p > 0.05). The average MSD of C6 and C7 was 4.92 ± 0.81 mm and 4.80 ± 0.96 mm, respectively, showing significant differences from those of C3, C4, and C5 (p < 0.05). If 6 mm of the MSD isn’t secured, OSA showed in the cephalad direction of 11.5° for 5 mm and 22° for 4 mm approximately.
Conclusion:
We suggest that mini-screw on lateral mass can be fixed safely without FV, if they are fixed at MSD of 6 mm from a joint surface. Facet joint violation doesn’t occur if an OSA is given in the cephalad direction in case of not enough MSD for mini-screws.
Keywords
Introduction
Introduced for the first time by Hirabayashi, the open-door laminoplasty is currently adopted widely as a main therapy for cervical spondylotic myelopathy patients. 1,2 Many authors introduced techniques using various instruments, such as ceramic block, allograft, stay suture, and wire. Recently, rigid fixation with mini-plate between the lateral mass and the lamina comes into spotlight and it is reported to lower the probabilities of hinge closure and restenosis. 3 –9
In the cervical spine, a facet joint is sloped downward toward the posterior. When an open-door laminoplasty is performed using a mini-plate, a facet joint violation can occur, if inferior screws are fixed in the lateral mass. This can accelerate facet joint degeneration and axial symptom 10 (Figure 1). If the sagittal trajectory is parallel with a facet joint, the probability of facet joint violation would be low, but it is difficult to make an entry parallel with the facet joint, if a plate is adjusted to the posterior margin of the lateral mass and screws are fixed perpendicularly. Therefore, it is possible for screws to avoid violating a neighboring facet joint, when the plate is positioned in the upper part of the lateral mass. There has been no report on how far a screw fixation in the plate and the lateral mass should be separated from the facet joint surface. This study aimed to present radiologic analysis of minimal safe distance (MSD) and optimal screw angle (OSA) that enables to fix screws in a lateral mass safely without facet joint violation when open-door laminoplasty is performed using a precontoured plate.
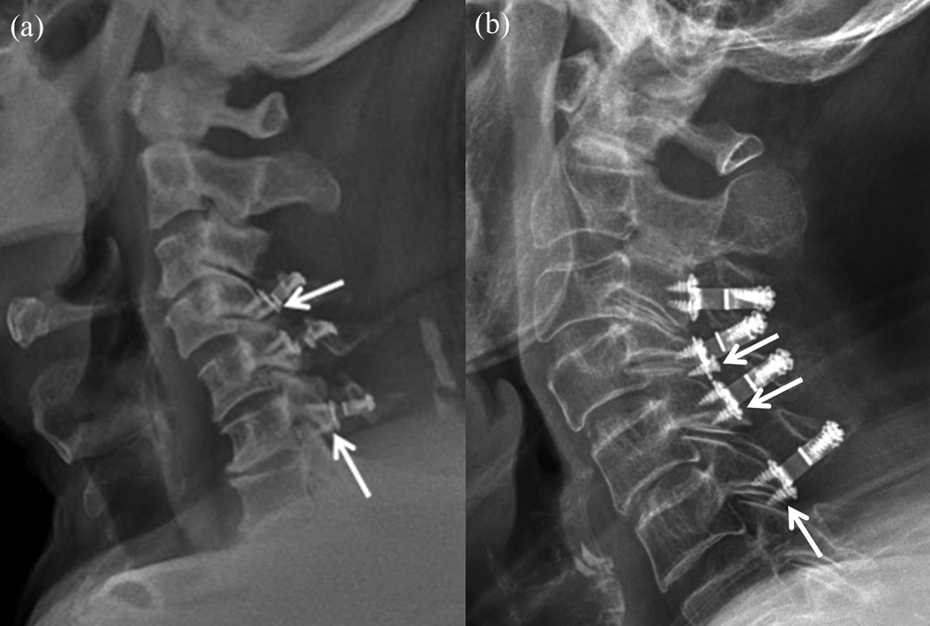
If a plate is fixed at the lower part of a lateral mass, inferior lateral mass screws violate a facet joint, thus causing axial symptom. (a) C4 and C6 inferior screws violated the facet joint. (b) C4, C5, and C6 inferior screws violated the facet joints.
Material and methods
We retrospectively examined the medical records of 22 patients (male: 17 and female: 5) who had undergone a single open-door cervical laminoplasty due to cervical spondylotic myelopathy from July 2012 to July 2014. The patients were 62 years old on average (scope: 30–80). A total of 158 screws of 5 mm were fixed. Of them, 79 screws were fixed in the inferior lateral mass. All the patients showed symptoms and physical features that corresponded to cervical spondylotic myelopathy and underwent imaging tests using C-spine X-ray, cervical computerized tomography (CT), and magnetic resonance imaging. The patients were provided with precontoured plate (Centerpiece®, Memphis, Tennessee, USA) for the laminoplasty.
Evaluation
Postoperative cervical spine CT was evaluated with all the patients who had undergone a single open-door laminoplasty. Inferior facet joint violation was checked in the sagittal image of CT, and a comparative analysis was made of the distances from plate to facet joint surface between facet violation (FV) and non-FV groups (Figure 2). An “MSD” was sought that does not allow 5-mm screws to violate a facet joint, when they are inserted. The distance between a facet joint surface and a non-facet joint point was defined as an “MSD,” when screws were inserted vertically into the posterior margin of a lateral mass at a level that corresponded to the midportion of the lateral mass on the sagittal CT cut (Figure 3). “MSDs” were measured for C3–C7 in all the patients, and a comparative analysis was performed to determine whether there were significant differences among levels.

The inferior margin of a plate and the distance of a facet joint surface were divided into a FV group and a non-FV group and compared with one another. FV: facet violation.
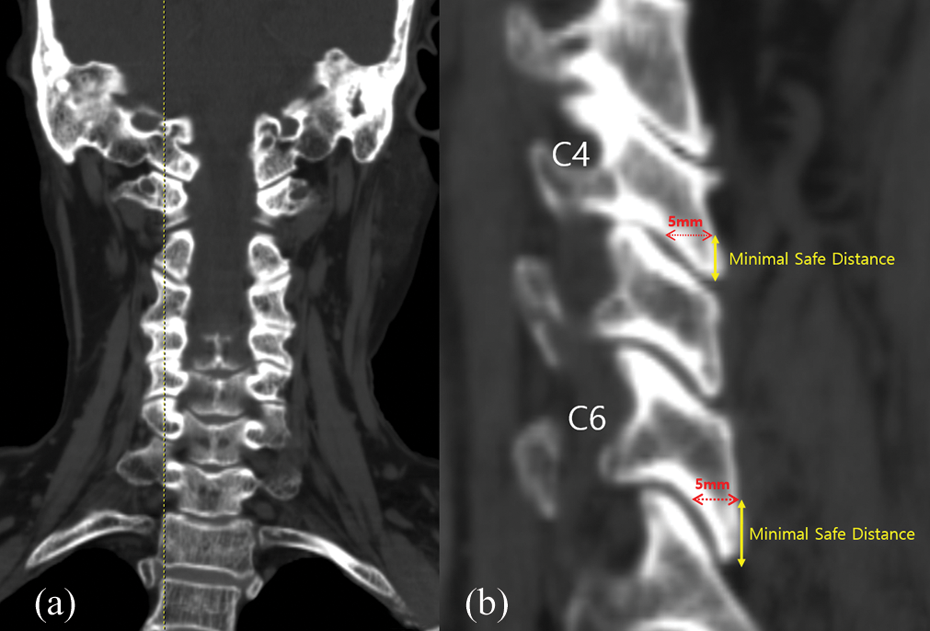
The distance between a facet joint surface and a point of non-facet joint was defined as “MSD”, when screws are inserted vertically into the rear side of a lateral mass at a level that corresponds to the midportion of the lateral mass on the sagittal CT cut. MSD: minimal safe distance; CT: computerized tomography.
When implanting a 5-mm mini-screw, approximately 6-mm MSD is required to prevent the facet joint from being destroyed, so that the distal mini-screw can be inserted perpendicular to the lateral mass surface. If MSD is not sufficient due to degenerative changes of the lateral mass, the OSA of the distal mini-screw should be inserted in the cephalad direction to avoid violation of the facet joint. The value was calculated from the tangent of a right triangle formed by the length of the screw and the hypotenuse (Figure 4).
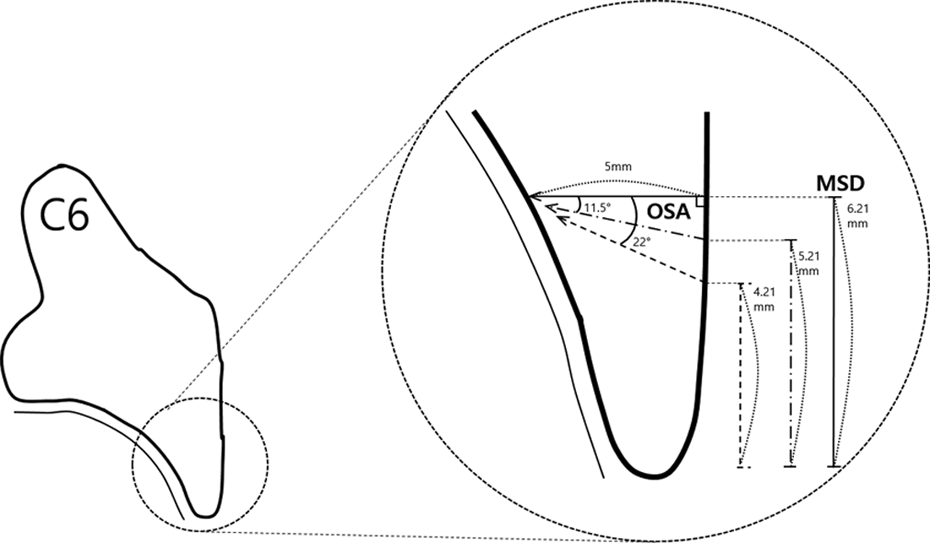
When implanting a 5-mm mini-screw, approximately 6-mm MSD is required to prevent the facet joint from being destroyed, so that the distal mini-screw can be inserted perpendicular to the lateral mass surface. If MSD is not sufficient due to degenerative changes of the lateral mass, the OSA of the distal mini-screw should be inserted in the cephalad direction to avoid violation of the facet joint. The value was calculated from the tangent of a right triangle formed by the length of the screw and the hypotenuse. MSD: minimal safe distance; OSA: optimal screw angle.
At the time of follow-up, it was examined whether there were screw loosening and breakage through an anteroposterior or flexion-extension lateral radiograph and whether axial neck pain occurred after FV surgery.
Surgical procedure
All patients underwent single open-door laminoplasty by one surgeon in the same institution. A patient was located in prone position after endotracheal intubation. Then, appropriate padding was performed using a sponge pillow to protect the patient’s face. Three-point fixation was not used as a routine to protect cranium. Head stabilization was obtained by simply taping alone. Thereafter, the patient was located in a reverse Trendelenburg position to decrease venous pressure. Standard posterior midline approach was performed. The posterior element was exposed that lateral edge and top and bottom facet joints were seen in the lateral mass into which screws were to be inserted. Spinous process was arranged with a bone cutter, and a hinge side trough was made using a burr, with 1–2 mm inner cortex of the lamina left behind at the medial border of facet joints. And an open side trough was made in the opposite lamina using a burr. Thereafter, the laminar hinge was opened gently using the laminar spreader and kept open using a plate, and then two screws were fixed at the upper and lower parts of the lateral mass and a screw was fixed in the lamina. Fluoroscopy was used to check the alignment of a patient before surgery and the state of plate fixation.
Statistical analysis
Statistical analysis was performed using SPSS 20.0. “MSDs” were measured twice in the both lateral masses of a patient, and all values were expressed in average ± standard deviation. An analysis was made of distances from facet joint surface to plate between the groups of FV and non-FV using the Mann–Whitney U test. A comparison was made of differences in “MSD” among levels using the Wilcox signed rank test. Additionally, a value was calculated that corresponded to 95 percentile of “MSD,” and a comparative analysis was made of differences among levels. A difference was accepted as significant, if the probability was less than 5% (p < 0.05). Interobserver and intraobserver reliability analysis using the intraclass correlation coefficient (ICC) values was performed to determine consistency among observers. Comparison of the ICC values was performed using the Z-test. A difference was considered significant for a p value of less than 5% (p < 0.05).
Results
Thirty-two, 42, 44, and 40 screws were fixed at the superior and inferior portion of a lateral mass in C3, C4, C5, and C6 levels, respectively.
According to a CT image, a facet joint was violated by 27 screws fixed in the inferior lateral mass, which accounted for 34.1% of screws fixed in the inferior lateral mass. Of the 27 screws, 3, 5, 9, and 10 screws were located at C3, C4, C5, and C6 levels, respectively (Table 1).
FV percentage of inferior lateral mass screw.

FV: facet violation.
At each level where laminoplasty was performed, joint surface to plate distances was 3.18 ± 1.46 mm and 4.75 ± 1.71 mm in the groups of facet joint violation and non-FV, respectively. This shows that there were significant differences between the both groups (Table 2).
Differences in distances between plates and facet joint surfaces.

When 5-mm screws were inserted into a lateral mass, the “MSD”, which is so separated from the inferior facet joint as not to involve a joint, was 4.39 ± 0.83 mm on the average according to a calculation using a CT sagittal image (Table 3). The average “MSDs” of C3, C4, and C5 were 4.05 ± 0.78 mm, 4.10 ± 0.70 mm, and 4.26 ± 0.74 mm, respectively. There was no significant difference among levels (p > 0.05). The average “MSD” of C6 and C7 was 4.92 ± 0.81 mm and 4.80 ± 0.96 mm, respectively, showing significant differences from those of C3, C4, and C5 (p < 0.05; Table 4).
Minimal safe distance.

MSD: minimal safe distance.
Similarities between levels in “MSD”.

MSD: minimal safe distance.
The average MSDs from C3 to C7 are approximately 5.87, 5.39, 5.76, 6.21, and 6.80 mm, respectively. To obtain the OSA, the difference between the length of the screw and the MSD can be set to the base and height of the right triangle. Then, OSA values can be obtained by substituting values for the height/base of the tangent formula in the right triangle. Assuming that a 5-mm mini-screw is implanted at a difference of 1 or 2 mm from the given MSD at each level, the base is equal to 5 mm and the height is 1 or 2 mm. When the tangent formula is substituted, tan θ = 5 mm/1 mm and tan θ =5 mm/2 mm. If the value of tan θ is obtained, a 5-mm mini-screw should be inserted in the direction of the cephalad at about 11.5° for 1 mm and 22° for 2 mm (Table 5).
OSA for variable MSD at each level.

MSD: minimal safe distance; OSA: optimal screw angle.
There were no other complications, such as screw breakage, loosening, and infection, according to the last radiographic follow-up. Axial neck pain was observed in 5 of 14 patients with FV: the 3 showed C3 and C4, C4 and C5, and C5 and C6 facet joint violations; 1 showed C4 and C5 and C5 and C6 facet joint violations; and 1 showed C5 and C6 facet joint violation. No significant difference was found between the measurements made by a single observer and those made by different observers. ICCs of inter and intraobserver reliability are 0.827 and 0.837, respectively.
Discussion
O’Brien et al. performed a laminoplasty using an axillofacial mini-plate and screws. Since then, the laminoplasty using a plate has made a remarkable development in technique and plate design. 11 The disadvantages of the laminoplasty were hinge closure like “spring back phenomenon” and restenosis in the spinal canal. Their occurrence could be reduced using a mini-plate. 3,12 In our case series, there is no plate-related hinge closure. However, since plate-fastening screws into lateral mass violated a neighboring facet joint, complications such as posterior axial neck pain and neck range of motion (ROM) limitation after surgery should be checked.
Jiang et al. also reported that 36% of cervical laminplasty group has shown axial cervical pain, which didn’t reveal the fundamental risk factors for postoperative pain. 13 Yeh et al. reported that moderate-to-severe axial neck pain was shown on 42% of patients after 3 months cervical laminplasty. 9 Facetal violation of mini-screws of precontoured plate could negatively influence the postoperative axial pain and range of motion, but there are still ongoing debate on the risk factors.
Chen et al. recently reported that damaged facet by mini-screws has more axial pain and postoperative limitation of cervical motion. 5 Optimal area of lateral mass mini-screws using computer program software incorporating CT scan was proposed using only 7-mm screws by Chen et al. 4 However, this method has the limitation that the boundary of the lateral mass is randomly drawn through the software and cannot be used easily during the operation. And the implant angle of the mini-screw was not considered. The implant angle is the part that can affect the results sufficiently.
In the cervical spine, there were personal differences in the longitudinal length of the lateral mass, in the change of morphology by degenerative change, and the angle between facet joint and vertical line. Accordingly, “MSD” values showed a broad distribution. Fixed with a distance of 6.0 mm from the facet joint surface, screws could be fixed with a facet joint violation probability less than 5% at C3, C4, and C5 (Table 3). However, C6 showed a significant increase in “MSD”, compared to C3, C4, and C5. If screws were fixed with a distance of 6.0 mm, there was a high possibility of FV. Therefore, a plate should be fixed in a high position at C6, and the probability of FV seems to be safe (5% or less), when screws are fixed with a distance of at least 6.2 mm. C7 is often not included in opening laminoplasty but in rare cases that need to be included, C7 lateral mass presents a special challenge due to transitional anatomy. The screws at C7 probably need to be more cephalad and angled to avoid the caudad facet joint (Table 3). The lower cervical spine is approached, the more verticalization of the facet joint draws to the thoracic spine, which increases an “MSD”. Considering the mean MSD in our study, if the MSD was not obtained during surgery due to degenerative changes of the cervical spine, we think that the OSA gives a cephalad direction of about 10° when the 1-mm MSD is shortened. This suggests a guideline for inserting mini-screws safely.
This study also has limitations. First, it is difficult to make an equal application, if there is morphological variance in the cervical spine due to degenerative change and so on. Second, no account was taken of inter-individual difference for facet joint angle. Lastly, the present study is a retrospective one with a few numbers of cases and no control group. This is a simple radiologic analysis and calculation not enough to reflect all clinical relevance in terms of neck pain and decrease of range of motion. This makes it necessary to make broader prospective follow-up studies.
Conclusion
MSD and OSA are important to safe mini-screw fixation without FV. If the MSD is 6 mm, a 5-mm mini-screw can be safely inserted. If the MSD is shorter than 6 mm, it is advisable to insert it in a cephalad direction of about 10° for every 1 mm shorter.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.