
Abstract
Objective:
Preoperative tracheal retraction exercise (TRE) to minimize the occurrence of postoperative oropharyngeal dysphagia after anterior cervical spine surgery.
Methods:
A total of 220 patients admitted for elective anterior cervical spine surgery from January 2013 to December 2014 were retrospectively reviewed. The patients were allocated into two groups: TRE group and control group (without TRE). Modified dysphagia scoring system (MDSS) was used for evaluating the presence and severity of dysphagia symptoms at 1 week and 1, 3, and 6 months after surgery. Demographics such as age, gender, smoking, type of procedure, number of levels operated, duration of surgery, intraoperative blood loss, and instrumentation were analyzed. The clinical outcomes in both groups were compared with Neck Disability Index (NDI), Visual Analogue Scale (VAS) for arm and neck pain, and Odom’s criteria for global outcome.
Results:
In the first week postoperatively, 86 patients (39.1%) developed dysphagia, which decreased to 72 (32.7%), 5 (2.3%), and 4 (1.8%) after 1, 3, and 6 months, respectively. The patients who received the TRE prior to surgery had significantly better MDSS scores (p = 0.032 for second-level, 0.022 for third-level, and 0.009 for fourth-level fusions) than control group patients who did not receive TRE at the first week of surgery. At the 1-month follow-up, the followed-up patients for second- to fourth-level fusions in the TRE group had improved MDSS scores than those in the control group (p = 0.041 for second-level, 0.025 for third-level, and 0.0011 for fourth-level fusions). MDSS scores showed no significant difference between both the groups at 1 and 3 months postoperatively for single level anterior cervical fusion. NDI and VAS scores didn’t yield any significant difference. Global outcome by Odom’s criteria was 88.6%.
Conclusion:
Preoperative TRE can significantly reduce the occurrence of postoperative dysphagia after ACDF surgery. During follow-up, the incidence of postoperative dysphagia was significantly lower and had resolved at 3 months in all patients.
Introduction
A potential complexity of anterior cervical spine surgery is “dysphagia” which is defined as problem in swallowing. The mechanism behind oropharyngeal dysphagia is difficulty in initiation of the swallowing process, which originates from abnormalities of sensory innervations, muscles, and structures in the oral cavity and pharynx. Its symptoms include difficulty in initiating swallowing, inability to hold or control saliva and food within the mouth, choking, coughing, nasal regurgitation, aspiration pneumonia, unexplained weight loss, and wet voice after swallowing. Smith and Robinson in 1955 were the first to describe the anterior approach to the cervical spine. This surgical approach has widely been practiced for the treatment of cervical spondylosis and degenerative disc-related diseases with anterior discectomy, interbody fusion, and instrumentation. 1,2 Although the Anterior Cervical Discectomy and Fusion surgery relieves radicular pain and improves neurological functions, one of its potential complications is early postoperative dysphagia, which remains a major clinical concern, and up to 79% of cases have been reported within the first week of surgery. 3 –7 A prospective study reported postoperative dysphagia incidence to be 50.2, 32.2, 17.8, and 12.5% at 1, 3, 6, and 12 months of intervals, respectively. 8 –11 However, its causes remain multifactorial; one of which is tracheal and esophageal retraction during the surgery to make the clear exposure of anterior aspect of the cervical spine which may lead to tension on the surrounding structures involved in the deglutition process. Majority of patients remain asymptomatic or may develop mild to moderate symptoms, whereas severe dysphagia can lead to malnutrition, aspiration pneumonia, esophageal perforation, and even death. Furthermore, the psychological and social impact of dysphagia on the patient’s quality of life has not been routinely reported in large studies. 12,13
Improved understanding of risk factors, multifactorial causes leading to dysphagia, and improvement of surgical techniques could aid in minimizing postoperative complications. Several studies have correlated demographics (age, gender, alcohol/tobacco consumption, hypertension, diabetes mellitus) and surgical factors such as duration of surgery, use of material, design and thickness of a cervical plate, intraoperative retraction time, ET tube cuff pressure, steroids use, number of levels operated, and revision versus primary surgery with the occurrence of postoperative dysphagia after anterior cervical spine surgery, but the results showed wide-range of variations and hardly could draw any firm conclusions. 14 –18
The aim of our study focused on the manual tracheal retraction exercise (TRE) and its efficacy on reducing the occurrence of postoperative dysphagia after ACDF surgery. Its implications into clinical practice could decrease the morbidity and health-related costs by minimizing the potential complications of anterior cervical surgery. We evaluated the outcomes of preoperative TRE and postoperative dysphagia during a 6-month postoperative period using modified dysphagia scoring system (MDSS).
Materials and methods
This study was approved by the Institutional Review Board of Shanghai East Hospital, Tongji University School of Medicine. Between January 2013 and December 2014, 220 patients (116 males and 104 females, with mean age = 58 years, ranging from 48–83 years) underwent first- to fourth-level ACDF surgery for the treatment of cervical spondylotic myelopathy/radiculopathy between C3 and C7, secondary to degenerative disc disease at this center by a single surgeon. The patients were allocated into two groups: TRE group (n = 111) and control group (without TRE; n = 109). Exclusion criteria included anterior cervical corpectomy surgery, preoperative dysphagia, previous anterior cervical surgery, rheumatoid arthritis, and any other neurological or neurodegenerative diseases. All patients’ medical records were retrospectively reviewed. The presence and severity of dysphagia was evaluated using MDSS (Table 1). After thorough physical examination and routine investigations, patients’ baseline characteristics were recorded, including age, gender, medical and surgical history, smoking/alcohol consumption history, total operative time, number of operated levels, and estimated blood loss.
Modified dysphagia scoring system.

Preoperative tracheal exercise method and frequency
Since the day of admission, patients in the TRE group received TRE under the strict supervision of a junior spine surgeon. During the TRE, the patient lied in supine position with rolled pillow underneath the shoulder to maintain the neck in slightly extended position (Figure 1(a)). The surgeon stood by the right side of a patient and placed his right thumb and four fingers laterally underneath the neck skin through the medial edge of the right sternocleidomastoid muscle and tracheal sheath. Firstly, the tracheal sheath was relaxed by moving it to the right and left sides at least for 1 min and then stretching was done to the left side to a minimum of 1 cm apart from the anterior midline of neck and left relaxed itself after each stretching (Figure 1(b)). TRE was conducted five times a day with 15 counts every time at an interval of 3–4 h. The patients in the control group did not receive TRE since the day of admission.
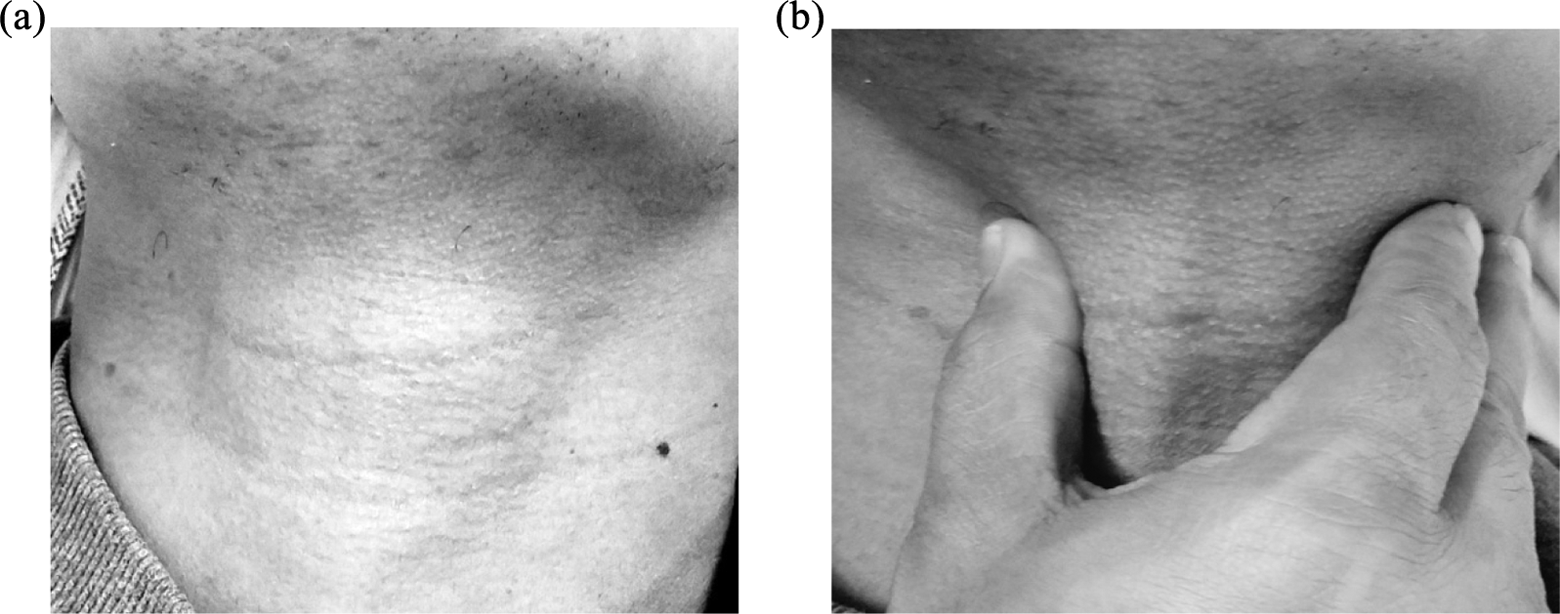
Tracheal retraction exercise. (a) Neck in slightly extended position and (b) tracheal sheath stretching to the left from the anterior midline.
Surgical technique
All the patients underwent the right-sided Smith–Robinson surgical approach under general anesthesia with endotracheal intubation. Cervical interbody fusion was done using a polyether ether ketone spacer, local bone grafts harvested from osteophytes, and titanium plate fixation. S-retractor underneath the longus colli muscle was used for intraoperative retraction of the trachea/esophagus instead of self-retaining retractors in all cases. Irrigation was not performed after placing the cage. A drain was placed in the retropharyngeal space in all cases and removed the next day when discharge was <30 ml.
Evaluation on follow-up
The patients in both the groups were evaluated using Neck Disability Index (NDI), the Visual Analogue Scale (VAS) for neck and arm pain, and Odom’s criteria for clinical outcome assessment. Also, the patients answered MDSS questionnaires at 1 week and 1, 3, and 6 months postoperatively by telephonic interview. Patients’ dysphagic symptoms were graded according to their clinical presentation as: 0 = none, 1 = mild, 2 = moderate, 3 = severe. Patients with no episodes of swallowing difficulty/problems were graded as “none,” whereas patients with occasional and rare episodes of dysphagia with specific food were graded as “mild.” Difficulty with large volumes or rapid swallowing of liquid or unable to swallow certain solid foods was regarded as “moderate,” whereas difficulty with all liquids and frequent swallowing difficulty with majority of solid foods were regarded as “severe.” The sum of total number of points at different follow-up time intervals was statistically analyzed.
Statistical methods
The data were processed using statistical software. Analysis of variance with Tukey’s test was applied for the comparison in demographics and preoperative data. χ 2 Test was used to determine significant differences and postoperative improvement in the clinical outcome scores between the two groups. The value p < 0.05 was considered statistically significant.
Results
The baseline demographics such as age, gender, smoking/alcohol consumption, and operated levels of two groups were evaluated and found to be statistically insignificant (Table 2). Moreover, clinical outcomes scoring systems such as NDI score and VAS score for neck and arm pain showed no significant intergroup difference. Postoperatively, NDI and VAS scores presented significant improvement in both the groups as compared to preoperative values (p < 0.05). However, intergroup difference between TRE and control groups was insignificant postoperation (Table 3). The global outcome utilizing Odom’s criteria demonstrated insignificant difference between the two groups. Overall, success rate (excellent or good) was 87.4–89.9% (Figure 2).
Patient data of two groups.

TRE: tracheal retraction exercise.
Clinical outcomes data of two groups.
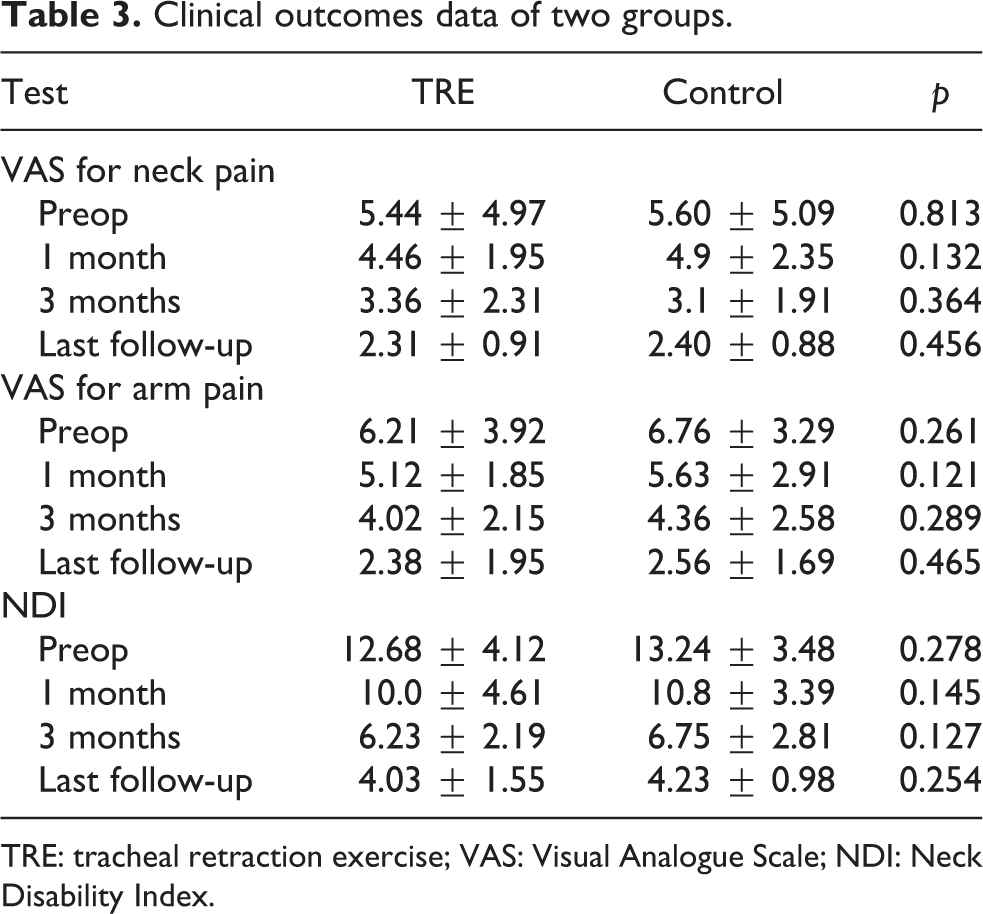
TRE: tracheal retraction exercise; VAS: Visual Analogue Scale; NDI: Neck Disability Index.

Odom’s outcome.
Eighty-six of the 220 patients developed dysphagia at 1 week postoperatively. Table 4 displays the dysphagia scores at each followed-up time interval for cervical spine patients subdivided into one to four fusion levels after surgery. As visible, the single-level fusion in both the groups showed no significant difference. At the first week of surgery, patients who underwent second- to fourth-level fusions showed significantly better dysphagia scores in the TRE group than the control group (p = 0.032 for second-, 0.022 for third- and 0.009 for fourth-level fusions). Also at 1-month postoperation, patients in the TRE group who underwent second- to fourth-level fusions showed better dysphagia score than the control group (p = 0.041, 0.025, and 0.011). At 3- and 6-month postoperation, the dysphagia scores between the TRE and control groups showed no difference for second to fourth level.
Average dysphagia scores during different follow-ups in different groups.

TRE: tracheal retraction exercise.
Discussion
The anterior approach to the cervical spine is a standard procedure for treating numerous spinal disorders. The procedure is considered to be safe and effective with good to excellent clinical outcomes. The occurrence of oropharyngeal dysphagia after anterior cervical spine surgery remains an under-recognized complication. The etiology and pathophysiological mechanism leading to postoperative dysphagia still remains poorly interpreted. Local ischemia of the surrounding tissues and oropharyngeal wall during surgery induced by medial retractor blades is thought to induce a reperfusion injury along with tissue swelling and edema formation after surgery which can subsequently cause early postoperative dysphagia. 19 –23
Smith-Hammond et al. reported that the incidence of dysphagia in an anterior cervical approach was significantly higher (almost 50%) as compared to a posterior cervical approach (20%). This study suggests that not only nerves’ stretch injury and esophageal edema are related but also some mechanisms are involved for causing dysphagia. Although, patients undergoing posterior lumbar approach lying in prone position with intubation same as posterior cervical approach did not develop dysphagia. 24
Previous studies reported that incidence of dysphagia after the anterior cervical spine surgery varied from 1% to 79% within the first week of surgery which declined to 50.2% at 1 month, and achieving a plateau between 13% and 21% at 12 months. 10 –12 In our study, the incidence of moderate or severe dysphagia was 32.7% at 1-month follow-up which slightly was lower than the reported average rates indicating that there is no standard method for accurately determining dysphagia. Consequently, different studies have varied dysphagia rates depending on the diagnostic criteria used. At the 6-month follow-up, no patient complained of swallowing difficulties. Several studies, including ours, show that dysphagia is a transient clinical problem and resolves over time. There were no rehospitalizations or reoperations for dysphagia or soft tissue swelling.
Although there is no definitive correlation between age and dysphagia, the mean age of nondysphagic and dysphagic patients was different in our study (54 and 59 years, respectively). The gender as a conclusive risk factor for developing postoperative dysphagia has yet not been proved. Fewer studies reported the incidence of dysphagia was higher in women as compared to men. The etiology of this finding is unclear, but it may be associated with the smaller anatomy of neck in females. 18 However, in this study, no significant gender ratio differences were observed. Our study showed that smoking was not a significant risk factor.
The role of cervical levels in developing postoperative dysphagia has also been evaluated. Jang et al. reported that the upper cervical levels at C3 relatively dispose to higher rates of dysphagia than the lower cervical levels at C4 and below. Although no significant correlation was found, the authors proposed that higher cervical levels require more powerful retraction due to the obstacle posed by the lower jaw. As a result, the forceful retraction would increase the chances of developing dysphagia. 15 Smith-Hammond et al. used Dysphagia Disability Index as a diagnostic criterion to compare patients undergoing surgery for higher subaxial cervical levels with lower subaxial cervical levels. However, no statistically significant difference was observed between the two groups. 24 Conversely, patients operated at C4–C5 and C5–C6 showed higher incidence of dysphagia in our cases. This finding could be related to the most operated two cervical levels (C4–C5 and C5–C6) in our center.
External compression to muscle tissue impairs local blood flow by increasing interstitial hydrostatic pressure. If the compression lasts for long time, muscle fibers and neural and musculature structures are damaged. 19,20 In lumbar spinal surgery, retracted paraspinal muscles demonstrated muscle fiber necrosis and structural changes with interstitial edema. 22 If we decrease the retractor pressure, local trauma and ischemia are less likely to occur.
Besides soft-tissue swelling which has the dominant role in the developing postoperative dysphagia, other causative factors have also been associated with deglutition dysfunction which includes injury to the superior laryngeal nerve, denervation of pharyngeal plexus by medial retractor blades causing esophageal dysfunction. Finally, elevation in intraesophageal pressure due to prolonged retraction may cause local ischemia and injury to the esophagus, 25 –28 although the difference in retraction time between the TRE and control groups in this study was not statistically significant.
Recent findings suggest that certain intraoperative preventive measures may minimize postoperative dysphagia after anterior cervical spine surgery. A retrospective review by Apfelbaum et al. described the measures to minimize ET-mediated compression of the RLN during retraction for anterior cervical surgery which consisted of monitoring and releasing of cuff pressure after medial retractor placement, allowing the ET to recenter within the larynx. However, this procedure may cause pressure-related injury to the RLN. 29 –31 It is known fact that high endotracheal tube cuff pressure increases the incidence of postoperative dysphagia, sore throat, and hoarseness. Study by Arts et al. suggested that maintaining ET tube cuff pressure at 20 mmHg might prevent dysphagia after anterior cervical spine surgery. 32 In our study, ET cuff pressure was maintained at the standard 20 mmHg in all the patients to reduce any possible causes for dysphagia.
Mendoza-Lattes et al. presented that lower perfusion of adjacent tissue and higher retraction pressure on the esophagus lead to an increase incidence of postoperative dysphagia. 16 As stated earlier, development of postoperative dysphagia was correlated with increased medial retractor pressure which causes decreased surrounding tissue perfusion during the surgery. If the retractor pressure on the esophagus is less than required, the surgical field will become obscure, which may hinder the surgical process; as a result, operative time may increase. Therefore, we applied the preoperative TRE. The aim of TRE was to enhance the flexibility and smoother mobilization of trachea/esophagus during anterior cervical spine surgery. We assumed that TRE has the indirect role in reducing the retractor pressure by facilitating flexibility and the smooth mobilization of tracheal-esophageal sheath during surgery so minimal retraction pressure applied through the S-retractor will cause less damage and injury to local surrounding tissues. In our study, the TRE group had low incidence of postoperative dysphagia suggesting that TRE may have reduced the postoperative complication.
Odom’s criteria are widely accepted as the standard and have been extensively used to report clinical outcome after cervical degenerative disc surgery. 33 In this study, patients operated at second to fourth levels had a significant improvement in different outcomes scoring system such as NDI, VAS, and Odom’s score. However, minor improvements were observed in patients operated at single level. According to Odom’s criteria, 70% were classified as excellent or good. In the present study, 87% of cases were satisfied with the outcomes of the surgery.
Despite current trends in understanding dysphagia, this study might have several limitations. Firstly, being a retrospective review, it is subject to patients’ recall lapses. Secondly, the data recovered were subjective (patient self-report is more reliable and credible) based on whether patients had dysphagia or not and accordingly, further interviewed to determine the severity of dysphagia. We did not perform any objective evaluation like videofluoroscopic swallowing or fiberoptic endoscopic evaluation and barium swallow studies, which could have explained more plausible reasons for dysphagia. Furthermore, neck swelling, hematoma, and soft tissue swelling can also be the contributing factors to dysphagia. Our study mainly focused on preoperative TRE and its effect on postoperative dysphagia. The etiology, risk factors, and other factors contributing to postoperative dysphagia could not be evaluated. In this study, we did not conduct longer duration follow-ups as our aim was to determine the immediate occurrence of postoperative dysphagia in both the groups after surgery.
Conclusion
In summary, TRE proved to be an affordable and risk-free maneuver. TRE can be practiced at the bedside for minimizing the postoperative dysphagia, especially in patients with multilevel anterior cervical spine fusion. By 3 months, dysphagia had resolved in all cases. We could only assume that less retractor pressure that TRE enhances by making trachea/esophagus more flexible with smoother mobilization has a significant effect on reducing the postoperative dysphagia after ACDF. Further evaluation of TRE effects on reducing postoperative dysphagia still remains to be investigated.
Footnotes
Acknowledgments
The authors thank the patients consent with permission and also thank doctors Xiaoming Liu, Yufeng Huang, and Weidong Zhao for their valuable help.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the Key Discipline Construction Project of the Pudong Health Bureau of Shanghai(PWZx2014-02) and the National Natural Science Foundation of China(81371994).